
Abstract

During the last two decades, several minimally invasive techniques have been developed to treat the incompetent great saphenous vein (GSV). In the late 1990s, various endovenous laser treatments were generally used.1,2 During this procedure the temperature of the venous wall tissue and blood remaining in the vein can reach temperatures of over 800℃. This causes carbonization and a release of steam bubbles and gases.3–5 During and after the endovenous laser ablation (EVLA) procedure patients often report a barbeque-like taste. Even the treating surgeon can sometimes smell an indistinct odour. The sensation of flavour is due to three main chemoreceptor systems:6,7 olfaction (sense of smell by nose), gustation (sense of taste by tongue) and trigeminal (sense of irritation of trigeminal receptors). The sense of smell is used to detect patterns of volatile compounds, while the sense of taste is used to detect non-volatile chemicals.
Electronic noses (e-noses) have been developed as a simplified ‘electronic’ model of the human olfactory system and were used in the present study to analyse the breath produced during EVLA. In our centre EVLA 980 nm bare tip is being used for the treatment of the GSV and small saphenous vein, using tumescent anaesthesia only.
In this study we hypothesized that e-nose assessment can detect changes in exhaled breath molecular profiles during the EVLA procedure. We also hypothesized that non-physiological and elevated volatile organic compounds (VOCs) can be identified and quantified by gas chromatography-mass spectrometry (GC-MS) during EVLA. 8 We aimed to associate these observations with the subjective tastes and odours as reported by the subjects.
This is an experimental study in patients eligible for EVLA, and agreed to have local tumescent anaesthesia. Inclusion and exclusion criteria for surgery and method of treatment have been fully described in a previous publication. 9 The study was approved by the medical ethical committee Noord-Holland, The Netherlands, and a written informed consent was signed by all patients.
Exhaled breath of 12 patients was analysed using the Cyranose 320 e-nose (Smiths Detection, Pasadena, CA, USA), a hand-held portable chemical vapour analyser, containing a 32-polymer nano-composite sensor array. 10 Patients needed to be sober and non-smoking for at least three hours, in order to avoid confounding factors for breath analysis. 11 Fifteen minutes before the EVLA, they breathed for five minutes through a non-rebreathing valve (Hans Rudolph, Kansas City, MO, USA) using an inspiratory VOC filter (A2, North Safety, Middelburg, The Netherlands) to avoid contamination by environmental VOCs. An expiratory silica reservoir was used to dry the expired air and a nose clip was used to prevent nasal air leakage. One single vital capacity manoeuvre was done while the expiratory port was connected to a 10-L Tedlar bag. The subject exhaled the full expiratory vital capacity into the bag with an expiratory resistance of 20 cm H2O. 12 The same procedure was repeated during the actual EVLA procedure 3–5 minutes after the start of the heating of the laser wire. Then a second Tedlar bag was filled with a single vital capacity volume. Within ten minutes the Tedlar bag was connected to the e-nose for analysis. Patients recorded whether they did have (yes = 1) or did not have (no = 0) a ‘barbeque-like’ taste and/or smell during the procedure.
The breathprints were analysed using SPSS software (version 18). A paired t-test was assessed to calculate the difference in breathprint measured at both timetables. Then correlation coefficients of these results and changes in perceived taste and smell were calculated. As an explorative procedure, in two out of 12 patients, GC-MS was introduced to perform specific compound analysis. Contents of the same bags were transferred to an adsorption tube which was subsequently analysed by GC-MS. GC-MS analysis was performed on an Agilent 6890GC with a 5975 MSD (Agilent, Santa Clara, CA, USA). Thermal desorption of the sample tubes was done using a system provided by Gerstel (Mülheim an der Ruhr, Germany). Data acquisition and analysis were carried out using Agilent Chemstation and NIST mass spectral database (National Institute of Standards and Technology, USA). Gaseous calibration standards (10 ppmv toluene in nitrogen, Air Products, Amsterdam, The Netherlands) were made by using a home-built dilution system and loaded on adsorption tubes to check the sensitivity of the system.
All GC-MS analysis was performed using the PLS Toolbox for MatLab (The Mathworks Inc., Natick, MA, USA) by Eigenvector Research Inc. (Wenatchee, WA, USA). The raw GC-MS data (3000 × 436 = 1.308.000 data points per spectrum) were first reduced using methods described by Windig. 13 That is to say, mass chromatograms (chromatograms at a specified mass) that did not pass a set of quality criteria were deleted from the set. Of the original 436 mass chromatograms, only 30 were retained in the analysis. The five major peaks can be ascribed to ethanol, acetone, isoprene, N,N-dimethylformamide and phenol, and are either compounds degassed from the Tedlar bag material or are normal constituents of exhaled breath. In other words, the main peaks observed, and their variance, have no relation to the bad odour problem. This observation is in good agreement with the findings of the e-nose measurements.
Twelve patients with incompetent GSV and treated with EVLA were analysed. Seven out of 12 patients perceived changes in taste or smell. The e-nose detected a significant difference in breathprint between the measurements before and during the EVLA treatment. (P = 0.020; Figure 1) Other components did not show a significant difference. There was no association between the breathprint and changes in perceived taste or smell (P > 0.09).
Change in breathprints of the e-nose during EVLA. The x-axis represents the study phase (before and during EVLA procedure). The y-axis represents the breathprints expressed as principal component, a dimensionless composite signal based on the 32 sensors of the e-nose. Each symbol-line represents an individual patient. EVLA, endovenous laser ablation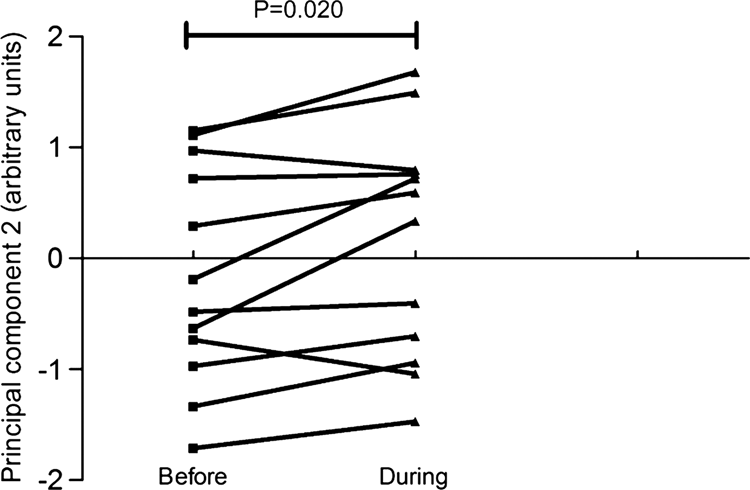
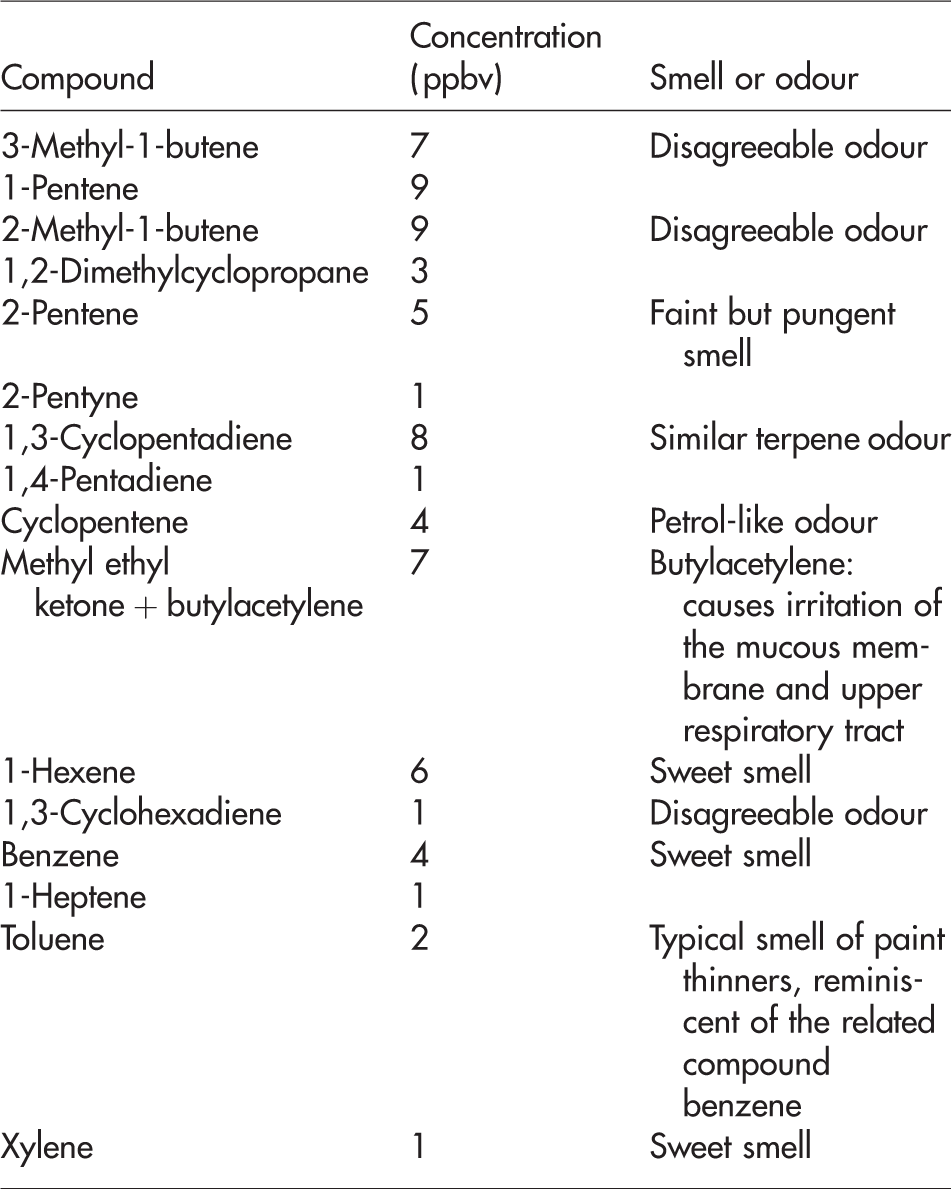
Summary of gas chromatography and mass spectrometry results during ablation. Sixteen new compounds or compounds with at least a two-fold higher concentration which are distinguished in samples taken during ablation
Exhaled human breath can contain thousands of VOCs in gas phase. 10 E-noses are able to analyse the VOC spectrum by composite nano-sensor arrays in combination with artificial intelligence based on learning algorithms. Each sensor represents partly different fractions of a VOC mixture, and the array exhibits good discrimination along with high sensitivity, short response time and reversible behaviour. Studies show that e-noses are able to detect (lung) diseases by pattern recognition (so called breathprints).11,12,14 Whereas e-nose analysis captures ‘fingerprints’ of VOC-mixtures, identification of individual molecular constituents requires standard analytical chemistry. This can be done using GC-MS, a technique capable of identification and quantification of individual VOCs. 15 In this experimental study we showed for the first time that the different smell sensation of patients during EVLA can be detected in exhaled breath. Exhaled breath captured a change in the molecular profile during the EVLA 980 nm procedure using a portable e-nose, while GC-MS showed changes in the levels of individual VOCs, e.g. unsaturated hydrocarbons and aromatics.
Non-physiological or compounds with at least a two-fold higher concentration were detected, which could be explained by the effect of pyrolysis. During the pyrolysis of complex organic molecules in blood and the vein wall tissue, a wealth of different compounds can be released. 16 This is likely to include acids, alcohols and various hydrocarbons. Since many compounds contribute to smell or taste and the odour threshold of each compound varies considerably, the sensation of smell and/or taste per person might be different. However, the subjective barbeque-like taste or indistinct odour reported by our subjects was not associated with the breathprint. Our data indicate that, although EVLA is an intracorporeal procedure, distribution and excretion of pyrolysis products takes place by the systemic circulation and the lungs. The question rises if endovenous procedures of other energy levels (EVLA 1470 radial tip) or radiofrequency (VNUS ClosureFAST) will also show signs of excretion of pyrolysis products. During these procedures, however, surgeons in our centre do not smell an indistinct odour and patients do not report barbeque-like taste. This does not exclude the fact that there is pyrolysis and excretion of hydrocarbons which could be detected by e-nose or GC-MS assessments. Until now, no studies are known which reported negative impact on health after endovenous treatment of incompetent veins and our findings also cannot show that the measured VOCs have an influence on health.
In conclusion, in this small study we did not find an association between the breathprints and changes of perceived taste or smell. This study does suggest that EVLA produces pyrolysis products that can be captured in exhaled air. The health implications of such compounds are as yet unknown.
Footnotes
Acknowledgements
The authors gratefully acknowledge Prof JA Rauwerda MD PhD, who launched the idea for this investigation, and JA Lawson MD PhD for his additional feedback in the final review.