
Abstract
Objective
The study aimed to test a Nitinol®-based vein cuff model for external banding valvuloplasty.
Method
In 12 adult minipigs, the vena jugularis externa was covered for 42 days by a cuff with an inner diameter adapted to the outer vein diameter in supine position. By changing from supine into prone position hypostatically vein dilation was induced to simulate varicose vein dilation. Cuff position and the inner diameter of the vein lumen under the cuff were examined by computer tomography scanning. Also, histological analysis of the vein wall within the cuff was performed.
Results
The preset tubular shape of the cuff and the cuff position did not change in both prone and supine position, but due to fibrosis the luminal vein diameter within the cuff was decreased (P < 0.01) already after 21 days.
Conclusion
A foreign body response resulted in a fibrous capsule covering the cuff which might limit cuff functionality.
Introduction
Primary venous insufficiency occurs when there is weakness of the vein wall or of the venous valve leaflets.1–6 External banding valvuloplasty (EBV) of the vein can be used in cases of primary vein incompetence to restore valve function. EBV of the great saphenous vein (GSV) in patients with varicose veins showed satisfactory results. 7 In addition, EBV prevents the loss of the GSV as a potential bypass graft in contrast to other surgical methods for the treatment of GSV insufficiency like high ligation and stripping, radiofrequency ablation and endovenous laser therapy. The premise for the EBV is that normal valve cusps are present in early-to-moderate varicose veins. There are pathological and clinical evidence in humans and conclusive results in animals that this is true.3,8–10
The rationale of the EBV procedure is to restore/regenerate valvular function by reducing the valvular annulus calibre bringing the valve cusps back to their correct positions restoring a sufficient valve closure. EBV is therefore a therapeutical approach of biomaterial-supported regenerative medicine. 11 For EBV, cuffs based on silicon, polyethylene terephtalate (PET) or thermomechanically expanded polytetrafluoroethylene (ePTFE) have been applied.7,12–15 PET is processed as spin-fibres into tapes with a size adapted to the blood vessel circumference. These cuffs are positioned around the blood vessel at the valve site and closed by suturing. The latter enables strong adaptation of the cuff diameter but the implantation with suturing of PET and ePTFE cuffs is time consuming. Moreover, none of the currently used cuffs for EBV are able to maintain the typical cross-section of the vein. To overcome these disadvantages, a cuff was developed from a NiTi alloy, which is commercially available under the trade name Nitinol® (Endosmart, Stutensee, Germany) for fast, minimally invasive implantation. The cuff material is processed into a tubular shape. The superelastic properties of Nitinol® warrant that shape changes of the cuff caused by external stress are re-adjusted to the preformed shape at body temperature. In this way, a stable cross-section of the vein shall be sustained so that a functional closure of the valve cusps can be re-achieved. Nitinol® additionally exhibits improved wear resistance.12,16 Its higher limit of elastic strain recovery as well as the improved wear resistance reduces surface cracking, corrosion and fracture. Biocompatibility, stability and safety of the Nitinol®-based cuff should be tested in animal models prior to clinical testing. 17 For such preclinical studies, pigs are frequently used as animal models because of their cardiovascular anatomy and physiology, 18 which show a broad range of similarities to humans.19–22 Minipig models especially are widely used for such in vivo studies due to their easy handling, housing and care. In addition, their growth rate is limited compared with common farm pigs.23–25 To our knowledge, there are no previous in vivo studies where the Nitinol®-based cuffs for EBV were evaluated. The present study aimed to evaluate the feasibility of implanting the Nitinol®-based cuff in minipigs, the capability of the cuff to limit vein dilation and to maintain the typical vein cross-section, and the influence of the cuff on vein patency over a period of 42 days.
Materials and Methods
Cuff manufacturing
Cuffs (SmartCuff 4-0, Endosmart, Stutensee, Germany) were manufactured from medical grade Nitinol materials (ASTM F2063-00)
16
and preshaped as tubes with different inner diameters (3.0, 4.0, 5.0 and 6.0 mm) to adapt to the vein calibre. In a recently published study,
9
a cuff length of 12.5 mm has been proven to limit dilation of varicose veins at physiological and pathological blood pressures. For this reason, we decided to also use a cuff with a length of 12.5 mm for the in vivo testings. As shown in Figure 1, the cuff was composed of four interconnected arched bands. Four cuff closure clasps which are integrated in one end of the cuff can be hooked into the vents of the other cuff end to interlock the cuff. The cuff was manufactured (Endosmart, Stutensee, Germany) in accordance with the Good Manufacturing Practice, the specifications of the EU Directive 93/42/EWG, the ISO standards 14155-1, 14155-2 (2003), the MEDDEV 2.7.1 (April 2003) and the EK-MED 3.9 (4/2006). To minimize possible tissue alterations caused by the rough surface, the cuff was electropolished after laser cutting. All cuffs were sterilized by ethylene oxide (gas phase: 10% ethylene oxide, 54°C, 65% relative humidity, 1.7 bar, gas exposure time: 3 hours, aeration phase: 21 hours) before use.
Stereo-microscopical images of the vein cuff (length: 12.5 mm; furled cuff (a, magnification 2.5×), opened cuff (b, magnification 3.5×); closed cuff (c, magnification 3.5×)
In vivo study design
In 12 pigs, a vein cuff was implanted around the left external jugular vein. Before the implantation and three, 14, 28 and 42 days thereafter, the cuff position and the inner diameter of the external jugular vein lumen under the cuff were examined using computer tomography scanning (CT) in both supine and prone positions.
For histological analysis of the vein wall six animals were sacrificed (with 1 M KCl [intravenous], 10 mL/animal) after 21 days of implantation and six animals 21 days later.
The present study examined the capability of the vein cuff to limit vein dilation without shifting caudally and rostrally, and to maintain the typical cross-section and micromorphological structure of the vein. The external jugular vein of the right side was sham operated as a control.
Animals, housing and care
In vivo experiments were approved by the Regional Office for Health and Social Welfare (LaGeSo) of Berlin and performed at the animal facility of the Charité University Clinic, Campus Virchow (Berlin, Germany), Department of Experimental Medicine (certified by ISO 9001), with adult female pigs (n = 12, age: 21 months) from the breed GöttingenTM Minipig (Ellegaard, Denmark; body weight 35.3 ± 4.8 kg). The animals were housed in groups of six in an environmentally controlled room (12/12 light/dark-rhythm, 15–24°C, 55 ± 10% relative humidity) and cared for according to the guidelines of the European Societies of Laboratory Animal Sciences.
Anaesthesia
Prior to CT imaging and surgery, anaesthesia was administered. For one day before anaesthesia, the animals were deprived of food, but had free access to water. The minipigs were premedicated by intramuscular injections of 0.5 mL atropine (Atropinum sulfuricum, 1 mg/mL, Eifelfango, Bad Neuenahr-Ahrweiler, Germany) and anaesthetised by intramuscular injection of ketamine (27 mg/kg, UrsotaminTM, 100 mg/mL, Serumwerk, Bernburg, Germany), xylazine (3.5 mg/kg, RompunTM TS, 20 mg/mL, Bayer Vital, Leverkusen, Germany) and 3 mL azaperone (StresnilTM, 40 mg/mL, Janssen Animal Health, Bad Homurg, Germany). Continuous intravenous infusion of an electrolyte solution (IonosterilTM, Fresenius, Bad Homurg, Germany) was given to the animals. For venous cuff implantation, anaesthesia was maintained after endotracheal intubation with a mixture of isofluran (1.5–2.0 vol%) and O2. Ventilation parameters were set to maintain an expiratory partial pressure of CO2 (etCO2) within 35–40 mmHg and an oxygen saturation (SpO2) above 95 vol%. For amplifying the analgesia, 2 mL fentanyl (Fentanyl, 0.1 mg/mL, Janssen-Cilag, Neuss, Germany) was injected intravenously every 30 minutes during the surgical intervention.
Implantation procedure
The present study used a hypostatically induced vein dilation model. The model is based on the finding that the diameter of the external jugular vein of the GöttingenTM minipig (Ellegaard, Dalmose, Denmark) increases in the case of changing from supine to prone position (Figure 2). This position change caused a significant (P < 0.01) increase in the inner external jugular vein diameter of 4.3% (the luminal vein diameter was 7.4 ± 1.5 mm in supine position and 9.0 ± 1.0 mm in prone position, n = 12). The luminal diameter of the femoral vein did not change significantly when the position of the animals was changed from supine to prone position (4.7 ± 1.3 mm in supine and prone position). As a result, the femoral vein could not be used to induce hypostatic vein dilation.
Longitudinal section of the external jugular vein; inner diameter increase of the external jugular vein of a GöttingenTM minipig after change from supine (a, 7.4 ± 1.5 mm) to prone (b, 9.0 ± 1.0 mm) position; n = 12 minipigs; (1) external jugular vein, (2) internal jugular vein, (3) common carotid artery, (4) larynx; computer tomography scanning parameter: 80 mL iodinated contrast medium (XenetiX© 350), 120 kV, mean mA: 490, noise index: 15, collimated slice thickness: 64 × 0.625 mm, total detector width: 55 mm; rotation speed: 0.4 second−1; table feed per rotation: 55 mm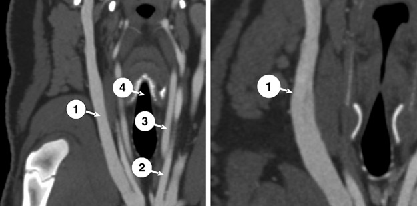
The left vena jugularis externa was covered by a cuff with an inner diameter adapted to the outer jugular vein diameter in supine position. To simulate varicose vein dilation, after surgery, the animals were changed into prone and standing position resulting in dilation of the external jugular vein except for the segment covered by the cuff.
Surgical procedures were performed under aseptic conditions on an implant site known to be exposed to considerable forces mainly caused by the superficial and deep skeletal muscles of the throat. An incision of 9 cm was made paramedian on the left side of the tracheal region in the middle part of the throat. The external jugular vein was prepared and a vein cuff with a predetermined inner diameter (3.0 mm, n = 1; 4.0 mm, n = 3; 5.0 mm, n = 6; 6.0 mm, n = 2) was implanted. Cuffs with different inner diameters were used to adjust the cuff to the external jugular vein diameters. The external jugular vein on the right side of the body was sham operated in the same manner as a control. Wound closure was performed by suturing (3-O VicrylTM, Ethicon, Norderstedt, Germany). Finally, the closed wound was disinfected with povidone-iodine (Betaisodona, Mundipharma, Limburg/Lahn, Germany) to prevent wound infection.
No anticoagulative substrate was applied after cuff implantation.
Computer tomography scanning
To evaluate the in vivo behaviour of the cuff, a CT scan of the throat was performed before cuff implantation and three, 14, 28 and 42 days thereafter. The CT scan was done using a 64-slice scanner (LightSpeed 64®; GE Medical Systems, Milwaukee, IL, USA). The pigs were scanned in both the prone and supine position to achieve different vascular pressures.
The scan protocol used contrast enhancement with automatic injections (intravenous) of a nonionic iodinated contrast medium (120 mL/animal, XenetiX© 350, Guerbet GmbH, Sulzbach/Taunus, Germany) via the vena auricularis caudalis.
The scan parameters were standardized (voltage 120 kV, maximal 600 mA with automatic mA-optimization at a noise index of 15, mean mA 490; collimated slice thickness: 64 × 0.625 mm; total detector width: 55 mm; rotation speed: 0.4 second−1; table feed per rotation: 55 mm), resulting in a scan speed of approximately 3 seconds for 30 cm scan length in the z-axis.
For volumetric assessment, 1.25 mm images were reconstructed without overlap and evaluated. Basic image analysis was performed using Advantage Windows 4.2 (GE Medical Systems) and AccuLite (AccuImage Diagnostics Corporation, South San Francisco, CA, USA).
The cuff position at three days after the implantation was compared with that at 14, 28 and 42 days after the implantation to monitor vein cuff dislocation. The position of the cuff was calculated as the ratio of the distance between the caudal end of the cuff and the bifurcation of the external and internal jugular veins (B, Figure 3), and the length of the external jugular vein from this bifurcation up to the junction of the maxillary and linguofacial veins (A). This ratio B/A had to be calculated because the length of the external jugularic vein can vary in different animals. The variance is possibly due to the different growth rate of the pigs as well as the elongation of the external jugularic vein caused by tilted head in supine position. The vein diameter was measured as inner diameter in a contrast medium-filled state.
Topography of the large blood vessels in an adult female minipig (age: 21 months); A: length of the external jugular vein, B: position of the vein cuff, defined as the distance between the caudal end of the external jugular vein and the caudal edge of the vein cuff; computer tomography scanning parameter: 80 mL iodinated contrast medium (XenetiX© 350), 120 kV, mean mA: 490, noise index: 15, collimated slice thickness: 64 × 0.625 mm, total detector width: 55 mm; rotation speed: 0.4 second−1; forward motion of the table per rotation: 55 mm. (1) Vena jugularis interna, (2) Vena jugularis externa, (3) Vena linguofacialis, (4) Vena maxillaris
Histology
After 21 and 42 days of implantation, the vena jugularis externa sinistra (including the surrounding vein cuff and peri-implantary tissues) and the vena jugularis externa dexter were explanted, fixed in formaldehyde 5 vol% solution and embedded in methacrylate (Technovit 7200 VLC, Heraeus Kulzer, Hanau, Germany). From the embedded samples, sections (10 μm) were prepared with a diamond-embedded cutting band and a surface grinding system (EXACT, Norderstedt, Germany) and subjected to stain with haematoxylin–eosin and Ladewig stain according to the protocols of Romeis. 26 One slide per sample (day 21: n = 6; day 42: n = 6) was analysed and each slide was evaluated at five different fields of view using a phase contrast microscope in transmission mode (Zeiss, Jena, Germany) and the image analysis software AxioVisio (Zeiss).
Statistics
Sample size estimation based on similar in vivo studies was not possible because no in vivo data with Nitinol vein cuffs were available. Therefore, in this first study the minimal sample size of six animals per group was chosen (6 pigs were sacrificed after 21 days, the remaining 6 pigs after 42 days) for histological examinations. Data are reported as mean value ± standard deviation for continuous variables, or as selective frequency for categorical variables, and analysed by Student's t-test or the chi-squared test. A P value of less than 0.05 was considered significant.
Results
All minipigs recovered well after a surgical procedure and CT examination. No sign of infection or adverse reaction to contrast media was observed.
Jugular vein diameter in prone and supine position
Over the study period the mean inner diameter of the right and left external jugular vein was significantly (P < 0.05) smaller (6.1 ± 1.4 mm, n = 12) in supine position than in prone position (8.8 ± 1.8 mm, n = 12, + 44%).
Cuff closure and shape stability
The clasp-based cuff closure mechanism enabled quick cuff closure. Over the whole time period of implantation, the clasps of the vein cuff stayed hooked in the corresponding vents and maintained a stable and reliable interlock. No change in the predetermined tube shape or circular profile of the cuff was observed over the whole time period of implantation. Figure 4 shows an interlocked vein cuff in its predetermined tube shape and circular profile at three, 14, 28 and 42 days after the implantation (in prone position) in one animal. Three days after the implantation, surgery-induced emphysema was obvious at the implantation site, and it was absorbed later.
Vein cuff applied on the external jugular vein; shape and interlocked status over time (prone position). Longitudinal (upper row) and transversal (lower row) section of the external jugular vein; (1) vena jugularis externa, (2) arteria carotis communis, (3) vena jugularis interna; computer tomography scanning parameter: 80 mL iodinated contrast medium (XenetiX© 350), 120 kV, mean mA: 490, noise index: 15, collimated slice thickness: 64 × 0.625 mm, total detector width: 55 mm; rotation speed: 0.4 second; table feed per rotation: 55 mm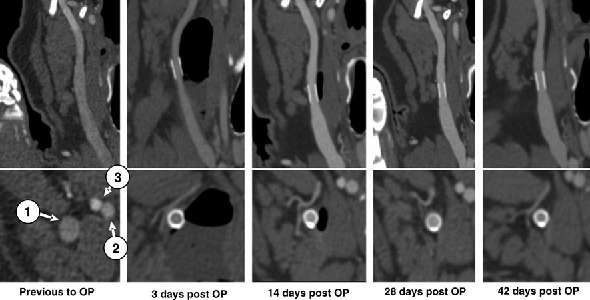
Cuff position
The mean length of the external jugularic vein in prone (supine) position (Figure 3, length A) was 88.0 ± 3.9 (92.8 ± 3.4) mm (n = 12). The mean shifted distance of the cuff was calculated as ratio of the distance from the caudal end of the vena jugularis externa up to the caudal end of the cuff (Figure 3, length B), and the total length of the external jugular vein (A). The cuff position showed no significant displacement within the 42 days of implantation.
Figure 5 shows the macroscopic changes around the implantation site. Immediately after the cuff implantation, microvascular bleedings in the adventitia were obvious and some connective tissue fibres were readily integrated into the cuff structure. After 42 days, the cuff was almost completely covered by a connective tissue-like capsule. Only small parts of the distal and proximal struts of the cuff were visible.
Vein cuff implantation site immediately (a) and 42 days (b) after implantation
Inner vein diameter
Three days after the cuff implantation, the intraluminal vein diameter under the cuff was measured using CT scanning. The intraluminal vein diameter within the cuff in prone (supine) position ranged between 38.8% (30.5%) and 30.9% (25.6%) of the predetermined cuff diameter (Figure 6).
Inner diameter of the left jugular vein from adult minipigs (body weight 35.3 ± 4.8 kg, age: 21 months) in prone (black dots) and supine position (white dots) related to the predetermined cuff diameter in % 3, 14, 28 and 42 days after implantation of a cuff; means±standard deviation, day 3 and 14: n = 12, day 28 and 42: n = 6, P < 0.05
The inner diameter of the left jugular vein was significantly decreased 28 days (P < 0.02) and 42 days (P < 0.01) after the cuff implantation. For example, in one animal (No. 5), the inner diameter of the vein within the cuff decreased from 2.4 mm (t0) to 1.1 mm (–54%; t = 28 days), and in the other one (No. 8) from 1.2 to 0.7 mm (–42%, t = 42 days). In the former case, the implanted cuff had a predetermined inner diameter of 5.0 mm and in the second case the predetermined inner cuff diameter was 4.0 mm. The vein wall thickness was calculated based on these data and the result indicated a significant increase after the implantation (P < 0.05). The vein wall thickness increased from 1.3 to 2.0 mm (+54%) and from 1.4 to 1.7 mm (+21%) in the first (No. 5) and the second (No. 8) animal, respectively.
At the right jugularic vein, which was used for sham surgery, no changes of the luminal diameter over time could be measured.
Histological changes of the venous wall within the cuff
Already after 21 days of implantation, due to a foreign body reaction, the cuff installed on the tunica adventitia was covered by an avascular fibrous capsule, in which practically no macrophages or other inflammatory cells were present at this time point (Figure 7). The foreign body reaction also resulted in a thickening of the tunica media and tunica interna within the first 21 days of implantation. The percent increase was 602.5% (from 28.4 ± 5.0 to 199.5 ± 84.7 μm) in the case of the tunica media and 127.3% (from 2.2 ± 0.3 to 5.0 ± 1.0 μm) in the case of the tunica interna (each n = 30).
Cross-section of a venous wall within a vein cuff 42 days after implantation; a1, a2: vein without vein cuff (control); b1, b2: vein with vein cuff (air bubble artefact on the tunica media); (1) struts off the vein cuff, (2) fibrous capsule covering the vein cuff, (3) tunica media with the transition zone between fibrotic and non-fibrotic tissue at the mark; haematoxylin–eosin staining; transmitted light microscopy, phase contrast mode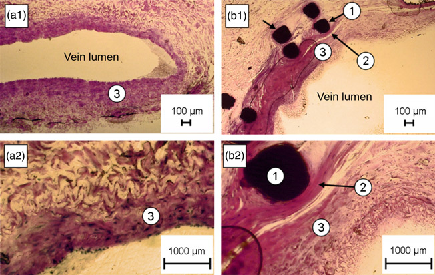
The thickness and the cell density of the fibrous capsule significantly decreased (from 392.8 ± 286.5 μm at day 21 to 68.3 ± 23.3 μm at day 42 [–82.6%]). In contrast, the thickness of the fibrotic tunica media and tunica interna remained stable (Figure 8).
(a) Decrease of the cell density in the fibrous capsule covering the vein cuff between day 21 and 42 of implantation; (b) changes in the thickness of the vein wall (tunica interna [white], the tunica media [grey]) and the fibrous capsule (shaded) around the cuff between day 21 and 42 of implantation; means±standard deviation, n = 30, *P < 0.05, ***P < 0.001
Sham surgery caused fibrosis in the skin. However, at the right jugularic vein, which was used for sham surgery, no signs of fibrosis were seen over time.
Discussion
Recently, we investigated the Nitinol®-based vein cuff for EBV in vitro. Examination of the cuff surface structure, after sterilization with ethylene oxide, using scanning electron microscopy, profilometry and X-ray photoelectron spectroscopy indicated that it has quite a smooth surface (mean square roughness Rq 66 ± 33 nm) primarily composed of nickel, oxygen, titanium, carbon and silicon with nickel being the least fraction (Ni: 0.7%, Ti: 1.7%, Si: 15.8%, O: 29.5%, C: 52.3%) of the surface elements. Si and C seem to be contaminations caused by a final cuff polishing with silicon carbide at the end of the manufacturing process. Cell compatibility tests with continuous fibroblast-like cells (L929) showed the cells readily adhered to the cuff surface after 24 hours. Furthermore, no significant cytotoxic effect was observed (MTS test). 27 In an in vitro test set-up designed to analyse cuff functionality, the cuff successfully limited dilation of varicose veins (human vena saphena magna) at physiological blood pressures (<120 mmHg) and also in case of hypertonia (300 mmHg) to the inner diameter determined by the cuff. In this follow-up in vivo study, limited dilation of varicose veins was confirmed again. Therefore, varicose vein dilation was simulated by changing the animal's position from supine to prone, resulting in hypostatically driven physiological vein dilation. This model cannot represent the complex pathologic situation of varicose veins, but it has proven to be suited for evaluation of cuff biofunctionality. Independent from the filling state of the external jugular vein, the cuff stayed firmly closed in its circular shape by the clasp-based mechanism. As a result, the vein segment directly under the cuff dilated only up to the predetermined cuff diameter. This ensures a permanent maintenance of the typical vein cross-section, and thus an optimal competence of the valve cusps can be achieved. Additionally, the cuff closure mechanism and the cuff structure effectively prevented the cuff from shifting up- or downwards along the vein throughout the implantation period. There was no need for further fixation on the adventitia, e.g. by suturing as known from the currently available cuffs for EBV like the GORE-TEX® containing external valve support with GORE-TEX® covering a Nitinol® reinforcing frame (W. L. Gore & Associates, Flagstaff, AZ, USA), or the silicone-based Venocuff IITM (AllVascular, Sydney, Australia) which is reinforced by PET fibres.12,14,15,28 Immediately after the implantation, connective tissue fibres of the adventitia got pressed through the spaces between the cuff struts. This caused a strong fixation of the cuff on the vein and prevented the cuff from moving up- or downwards along the vein despite the fact that the implant site is exposed to considerable forces caused by the skeletal muscles of the throat. On the other hand, this strong adaptation of the cuff to the surrounding tissue can be a problem if the cuff has to be replaced for size adaptation or if the cuff position has to be changed for any reason. In these cases it will take more time to isolate the cuff from the connective tissue fibres without damaging parts of the vasa vasorum.
Moreover, the outer vein cuff diameter did not change significantly. However, a more than 30% decrease of the inner vein diameter and an increase of the vein wall thickness in the vein segment directly under the cuff were noted in one-third of the animals within the 42-day implantation period. Regarding this phenomena, it is speculated that the cuff might have caused compression during vein dilation and damage to the vasa vasorum resulting in change of the vein wall composition due to the limited oxygen and nutrient supply, which triggers the growth of fibroblasts to initiate scar formation. Lane et al. 28 also found a reduction of the inner vein diameter after implantation of a vein cuff (Venocuff IITM) and related this to fibrosis occurring in the vein wall directly under the cuff.
In addition to the fibrotic changes of the tunica media and tunica interna, a fibrous capsule with a relatively high cell density almost completely covered the vein cuff 21 days after the implantation. This seems to be due to foreign-body response which is well known as chronic inflammatory response to implants.29–31 This fibrous capsule formation is important in the prevention of implant failure because the capsule minimizes adverse effects of the implant on the peri-implant tissue. 32 Once the fibroblasts migrate into the wound, they switch their major function to protein synthesis with collagen representing the major component. This activity starts from three to five days postimplantation and the absolute amount of collagen reaches a maximum at 2–3 weeks.33,34 In the subsequent remodelling phase of wound healing, collagen destruction starts35–37 by extracellular collagenases and phagocytic attack on collagen fibres by fibroblasts 38 resulting in a decrease in the fibrous capsule thickness after about three weeks and later.
To meet the problems of the Nitinol®-based cuff further studies will focus on alternative materials for the vein cuff design. The use of polymers with shape-memory capabilities, 39 which were recently shown to limit fibrous capsule formation, 40 might be a promising alternative to Nitinol®. Shape-memory polymers are well characterized (in vitro and in vivo) multifunctional biomaterials, which provide high shape stability, tailorable mechanical properties and shape-memory capabilities.11,39,41 The latter can be used for automatic cuff adaption to the vein calibre and also for automatic cuff closure. Additionally, the shape-memory polymers are available as biodegradable substrates, 42 which can be loaded with bioactive molecules. Examples for degradable polymer networks with shape-memory capability are copolyester urethanes 43 or polymer networks based on macrodimethacrylates.44,45 Degradable shape-memory polymers would degrade after integration into the connective tissue 40 of the adventitia and could support venous wall regeneration, e.g. by providing suitable stimuli such as cytokines.
Declarations
Footnotes
Acknowledgements
We would like to thank Melanie Pietsch and Christoph Mrowitz for their assistance in this research and the Endosmart company (Stutensee, Germany) for allocating the cuffs.