
Abstract
Objective
To show that adequate therapy for lymphoedema is able to restore ability to work.
Materials and Methods
The population of patients with primary lymphoedema registered in the university clinical centre diagnosed with primary or secondary lymphoedema and presumed by the national social institution as completely unable to work was selected for the retrospective analysis and divided into two groups. Group 1 consisted of 25 patients treated with a complex decongestive therapy programme daily for 3–6 weeks. The study population comprised 19 women and six men from 14 to 61 years of age (mean 31.5). In all 25 patients, complete inability to work was certified by the social institution before the treatment started. Group 2 consisted of 47 patients, 14 men and 33 women, aged from 26 to 71 years (mean 39 years) treated by so-called standard methods, who resigned from the proposed intensive treatment. In all 47 patients, complete inability to work was declared by the social institution before the treatment. Ability to work and oedema reduction were assessed by the treating physician.
Results
The intensive phase of treatment succeeded in 3870–15,330 mL oedema reduction in Group 1. After the end of therapy, 21 patients were able to work or study without any limitation and patients returned to their regular professional activity. Among four others, two were on welfare for at least 10 years, for another one welfare was their only income and one person was receiving a social pension. In none of the patients from group 2 was any significant oedema reduction observed. Every patient from group 2 maintained the social pension due to ineffective treatment.
Conclusions
Complex decongestive therapy is a very efficient form of treatment in advanced primary and secondary lymphoedema. It allows returning to work after a short period of temporary disability without the necessity of a social pension.
Introduction
Advanced lower extremity lymphatic oedema is a serious therapeutic problem. It affects about 300 million people around the world and it often causes disability due to the lack of radical treatment. 1–3 In contrast to well-developed care over patients with upper limb oedema, especially of those after oncology treatment in the area of axillary fossa, the possibility to gain qualified assistance for people with lower extremity elephantiasis is restricted. Limited awareness of therapeutic possibilities among both patients and their families and medical staff leads to the tendency to exclude this group of patients from normal social life.1,3,4 On the one hand, such a situation is a consequence of continuous limb condition aggravation which is a result of natural history as well as implementing inappropriate medical treatment. On the other hand, problems with movement and with keeping an adequate level of personal hygiene (e.g. the occurence of malodorous lymph leak) eliminate patients from active professional life. Additionally, such a situation is deepened by doctors who in many cases refer patients to a disability pension certificating permanent work disability. 5
Decisions on disability pensions in the National Social Security Institution (NSSI) are performed after examination by a physician contracted by the NSSI. The pathway is started by the patient in order to prove that his or her health condition deteriorated disabling full- or part-time productive work. A patient is supported by a general practitioner's (GP) letter, describing health conditions and pathologies in relation to actual frames of the patient's job. NSSI orders the medical examination. A patient is assessed physically, and the entire medical documentation is analysed. NSSI doctors assess the ability to work in studied and performed employment. A decision is based on subjective assessment and additionally on internal NSSI guidelines. The decision can be verified by special commission consisting of three NSSI specialists in different medical fields. NSSI and the patient may finally challenge the decision in court. Currently obtained certification guidelines in Poland in advanced cases of lymphoedema, based on rules accepted in Germany, cause most of the patients with proven advanced lymphatic oedema to be certified as permanently unfit for full- and part-time work. 5 Such an attitude worsens a patient's condition in many cases as a result of permanent elimination from broadly conceived social and professional life. This feeling of alienation is deepened by the patient's mobility constraints as well as the limitation of possibility to contact healthy people. Additionally, making it impossible for the patient to continue or to learn a profession exacerbates his or her financial situation, in addition to major-level mandatory co-financing of complex decongestant therapy (i.e. commute to specialist therapeutic centres, buying dressing materials as well as compression materials that are not re-imbursed by the National Health Insurance Institution). Ignorance, being a result of lack of knowledge concerning the lymphoedema therapy progress, and also automatic allowance of disability pensions are leading to the ‘vicious circle’ effect, making it impossible for the patient to return to normal professional activity.
What the study adds
Following the international consensus, it was well known that intensive decongestion therapy gives good results in lymphoedema reduction. 1 Our study is the first to compare such results with certification practice in NSSI.
The results of the study should be analysed by the doctors of Social Security Institutions in order to assess the real probability of restoration of ability to work in different treatment modalities.
Materials and method
To judge the possibilities of patients with advanced forms of lower extremity lymphoedema taking up professional activity, we retrospectively analysed the professional and medical situations of two groups of patients who were diagnosed initially in our department, accessible for follow-up, gave informed consent to different oedema-reducing therapy programmes and were assessed as disabled to work by social welfare professionals for the reason of lower extremity lymphoedema:
Group 1: 25 patients treated in our department between 1999 and 2006 (Table 1). The group consisted of 19 women and six men aged 14–61 years (mean 35.1). Primary lymphoedema was diagnosed in 19 patients and secondary lymphoedema was diagnosed in six patients. All of them suffered from symptoms of advanced lymphoedema stage III according to the International Society of Lymphology (ILS) 2009 consensus. 1 First symptoms of transient oedema occurred within the period of six months to 29 years (mean 12.6 years) before implementing therapy. In 18 patients, the oedema involved both limbs, and in 13 cases the lesions were symmetrically advanced. In 18 cases, additional skin lesions were occurring such as warty skin, lymphorrhea, toe ulceration or deformity. Oedema involved, in all patients, foot, calf and thigh.
Group characteristics
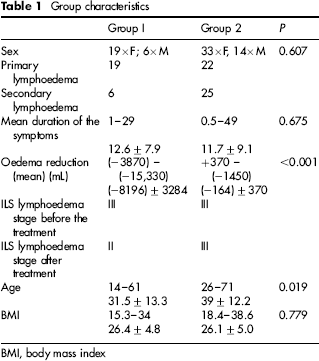
BMI, body mass index
All 25 patients were examined with the concern of disability to work and/or stating the disability level. In all cases, they were conceded to be completely disabled for full-time and part-time work, with permanent moderate or severe disability level.
With respect to all the patients, complex decongestive therapy was adopted (Table 2) containing manual lymphatic drainage, compression therapy with appropriately applied bandages, motor rehabilitation, pharmacotherapy and hygienic skin state caring. An intensive treatment phase lasting 3–6 weeks, containing everyday procedures, was led with respect to 15 patients in ward conditions.
Treatment modality summary (intensive phase)

After finishing the intensive treatment phase, the therapy was continued using periodic massages (one or two per week) and everyday compression therapy with the use of individually measured and custom-made hosiery with the third or fourth compression class, woven plainly with the seam. After the completion of intensive oedema reducing therapy, the return of patients to their current professional activity was assessed by the investigators common with the rules of certification in NSSI.
Group 2 (Table 1): 47 patients, 14 men and 33 women, aged from 26 to 71 years (mean 39 years):
Twenty-two patients with primary oedema from 12 to 49 years, with stage III (ILS); Twenty-five patients with secondary oedema from 6 months to 29 years, in stage III (ILS).
Treatment in group 2 was provided by GPs, quacks, ‘vascular doctors’ and by patients themselves, despite the initial diagnosis in our department.
A form of therapy (Table 2):
Seventeen patients repeated periodical hand massages, from this only in three cases, properly performed in combination with any form of compression. Others performed incorrectly (painful, in reverse order, with no compression). Eight patients bought their own wristbands for intermittent pneumatic massage, including 3× single-chamber, 4× four-cell, 1× 12-cell. Only in one case associated with stockings of standard class II compression. Twenty-four patients used compression therapy – only three cases correctly selected hosiery products. In nine cases, different uncertified bandages without compressing the ankles were used. Twelve patients used various uncertified hosiery products. Two patients did not use anything despite the stage of the disease accepting only extremity elevation for psychological reasons.
In all patients the reduction of the oedema in mL was assessed.
Results
With respect to all patients from Group 1, the whole planned therapeutic cycle was conducted which resulted in oedema reduction by 3870–15,330 mL (8196 mL on average) which was 48–65% of initial oedema. The range of oedema reduction was proportional to fluid compartments in subcutaneous tissue scale observed in ultrasound, and was inversely proportional to anamnesis length in location of lymphoedema (Table 3). Faster lesions accretion and their localization on the hip and calf, usually without foot involvement, fostered gaining better reduction of lymphoedema. Sex and weight had no significance.
Spearman correlation (rs) and calculated P value for oedema reduction and different variables in group 1
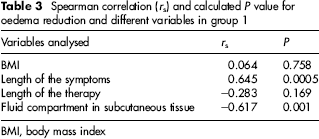
BMI, body mass index
Within three patients who suffered from unhealed wounds after earlier surgeries, after one week of therapy total oedema reduction was observed. Spontaneous ulcer epithelialization occurred in the case of one patient. With the two remaining cases medium thickness autological skin grafts were implemented and as a result, complete wound healing took place after another 2–3 weeks.
During the therapy, nine patients suffered from slight complications, i.e. superficial skin ulcers on the anterior calf's surface (n = 3), rash around the popliteal fossa (n = 2), foot neuropathic pains (n = 3) and skin abrasions (n = 1). Modification of used sponge or periodical, regional pressure constraint allowed lesions to heal within 2–7 days. The occurrence of complications mainly in the shape of ulceration and blisters unfortunately postponed expected therapeutic effect and extended the stay on the ward for one week in two cases.
After completion of the complex decongestion treatment, 21 people were functioning in social life without major constraints, four patients were continuing to study daily – one in junior high school, one in high school and the remaining two attended higher education. Seventeen people were working within their profession, including eight patients within broadly conceived public administration; seven were leading their own business and the remaining two were blue-collar workers. From among the remaining four patients who did not work, two people have not been working for at least 10 years, for one the disability pension was the only source of maintenance, and one was receiving a social pension.
In group 2, all resigned from complex decongestive form of therapy, rejecting suggestions and comments on the application of existing therapies. In at least 40 cases, they stated that successful treatment can cause negative decisions on welfare or social pension. In all patients from group 2, the certification of complete inability to work was maintained after a three-year control period by NSSI. In patients refusing intensive treatment, oedema reduction was only 164 (+370 – [–1450] mL) in geometric measurement. Body mass index, length of therapy and length of symptoms had no influence on the results of the therapy in group 2 (Table 4).
Spearman correlation (rs) and calculated P value for oedema reduction and different variables in group 2
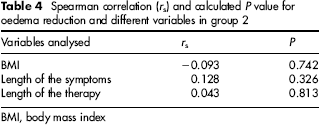
BMI, body mass index
Discussion
The physician working for NSSI in Poland has relatively few training materials which allow them to learn about the current state of medical knowledge concerning lymphoedema.5–7 Prevailing guidelines, on the other hand, quite laconically describe the state of the art on the subject of lymphoedema and stages of disease advancement. The work disability definition, stated in Polish normative records, assumes that the patient ought to qualify his or her professional engagement.8,9
It was stated, relatively arbitrarily, that only first and second lyphoedema stages do not determine complete work disability. 5 In the third stage of disease the necessity of specialist treatment is stressed, which in the opinion of people who prepare the guidelines, causes complete disability to work because of the permanent treatment necessity. The possibility of a return to professional activity is denied. Neither patients’ workplaces nor aggravations are analysed.7,9
Undoubtedly, advanced forms of lymphoedema at the level of foot, calf and thigh, because of their suggestive and ‘bizarre’ extremity appearance, determines the complete work disability certification as a natural solution for the majority of treating and assessing specialists.
According to current national guidelines, the intensive oedema-reducing treatment phase and the chronic sustain phase are not distinguished. The intensive phase lasts approximately six weeks and as a result, even most advanced forms of lymphoedema can be treated within temporary work disability as demonstrated in our material.4,6,10 –12
A few litres of oedema reduction significantly whittles away disability symptoms and, what is more, enables the patient to return to work if compression is correctly employed.13–15 Correctly led therapy necessitates patients’ and their families’ (or caretakers’) absorption; moreover, it accounts for a significant financial effort because of the lack of reimbursement in Polish conditions.16,17 For the time being, the minimum cost of the intensive therapy phase ought to be evaluated for 4000–6000 PLN (€1200–1800). This cost is an effect of compressive materials price and the necessity of everyday lymphatic massage.
One of the very important issues in the treatment of advanced forms of lymphoedema is the motivation of the patient. It is very important to stress that for majority of patients from group 2, the possibility of disability pension was extremely important, and overwhelmed the possibility of quality-of-life improvement after the therapy. Patients from group 1 were extremely motivated in order to achieve the possibility of full- or part-time work and even after three years of follow-up the reduction of the oedema was maintained at the level obtained after the intensive decongestive phase.
An important issue is to employ respective lymphatic oedema diagnostics. The currently offered solution is combined implementation of lymphoscintigraphy and magnetic resonance lymphography. This evaluation allows for a correct and both functional and qualitative valuation of the oedema. MRI lymphography is an especially useful tool to assess the primary reason for lymphatic oedema as well as to implement invasive treatment (tumour excision, microsurgical reconstruction of lymphatic vessels).18–20
Taking into consideration presented results of intensive oedema-reducing therapy treatment efficacy, prevailing work disability valuation guidelines for patients suffering from lymphoedema ought to be modified.
Our centre shares the opinion that lymphatic oedema can be effectively reduced to the level which enables the patient to return to professional activity within a short-term period. The high cost of the therapy necessitates, nevertheless, partial re-imbursement by NSSI and National Health Insurance found to implement presented treatment method popularly. The necessity of permanent compressive stockings can determine constraint to work ability within high temperatures; however, the current state of evidence makes this thesis rather speculative. Unfortunately, if the patient neglects the rules of effective oedema-reducing therapy after intensive treatment, the danger of work disability regression can occur. However, it does not exclude another tour of treatment implementation.
It is very important to note that in the majority of patients the benefit of treatment is not the important issue. The vast majority of the patients from the control group decided to conduct ineffective therapy to maintain the social pension instead of receiving income from normal work.
Conclusion
Advanced forms of lymphoedema can be effectively reduced within several weeks with complete ability to work restoration. Respective maintenance treatment eliminates the work disability certification.