
Abstract
Chronic cerebrospinal venous insufficiency (CCSVI) is a hypothesis through which cerebral venous drainage abnormalities contribute towards the pathogenesis of multiple sclerosis. CCSVI venoplasty is already practised worldwide. We report the case of a 33-year-old lady with multiple sclerosis who underwent left internal jugular venoplasty resulting in iatrogenic jugular thrombosis requiring open thrombectomy for symptom relief. This occurred without insertion of a stent and while fully anticoagulated. Clinicians should be aware that endovenous treatment of CCSVI could cause paradoxical deterioration of cerebral venous drainage. Patients with complications post venoplasty are now presenting to geographically distant vascular units.
Introduction
Chronic cerebrospinal venous insufficiency (CCSVI) is a hypothesis through which impaired cerebral venous drainage can lead to iron deposition in the cerebrum of patients with multiple sclerosis (MS). 1 There is controversy as to the role of this phenomenon and its endovascular correction. 2,3 Patients are already receiving venoplasty and stenting of stenoses in the jugular and azygous veins 4 despite European guidance to the contrary. 3
Case report
A 33-year-old woman with a one-year history of relapsing-remitting MS was admitted to our unit one-week postbilateral jugular and azygous venoplasty at a foreign institution (Figures 1 and 2). Her prior venography revealed a short segment stenosis at the junction of the left internal jugular and brachiocephalic veins that had been venoplastied with a 10 × 40 mm balloon at 10 atmospheres. Postoperatively she received dagibatran 220 mg, aspirin 100 mg and daflon 1 g daily and was fully compliant. On the third postoperative day she developed pain and swelling in the left side of her neck, but travelled back to the UK and a further three days later was admitted to our unit with worsening symptoms. On examination she was apyrexial, with SaO2 96% on air, and there was a tender swelling over the left internal jugular vein.
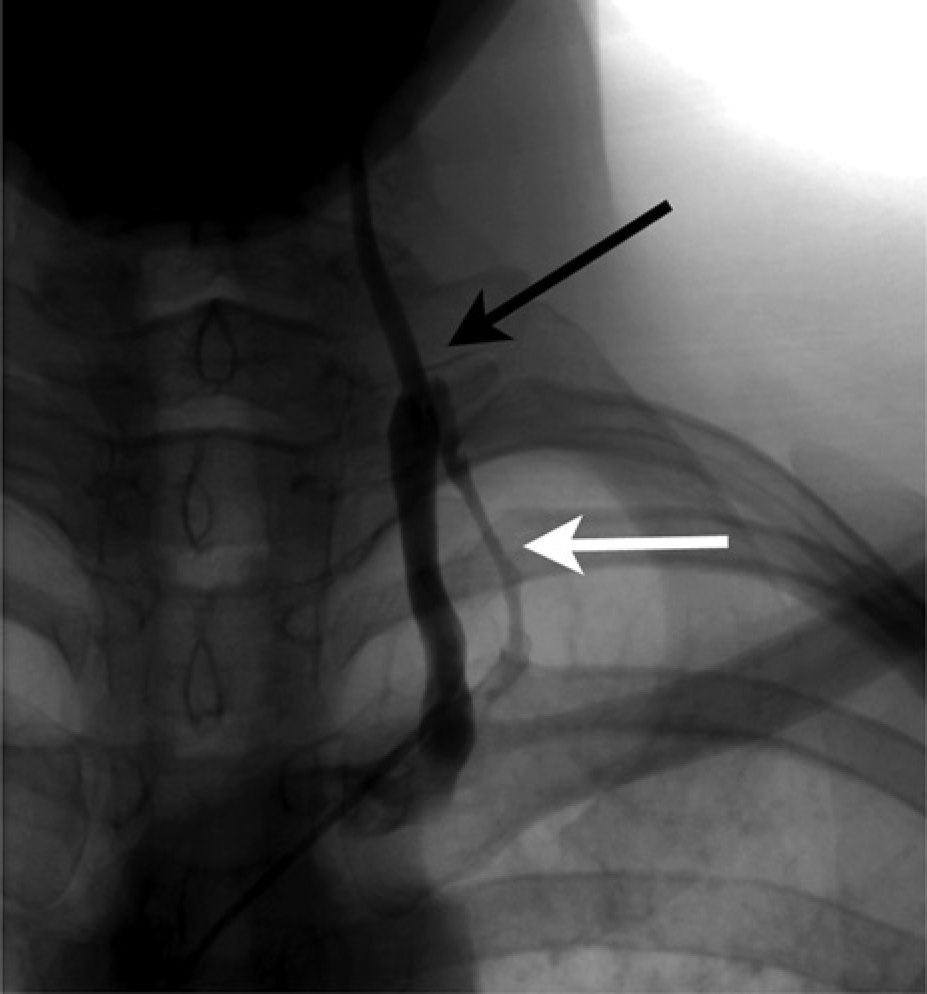
Venogram image showing apparent left internal jugular vein stenosis and venous collateralization surrounding the left brachiocephalic vein
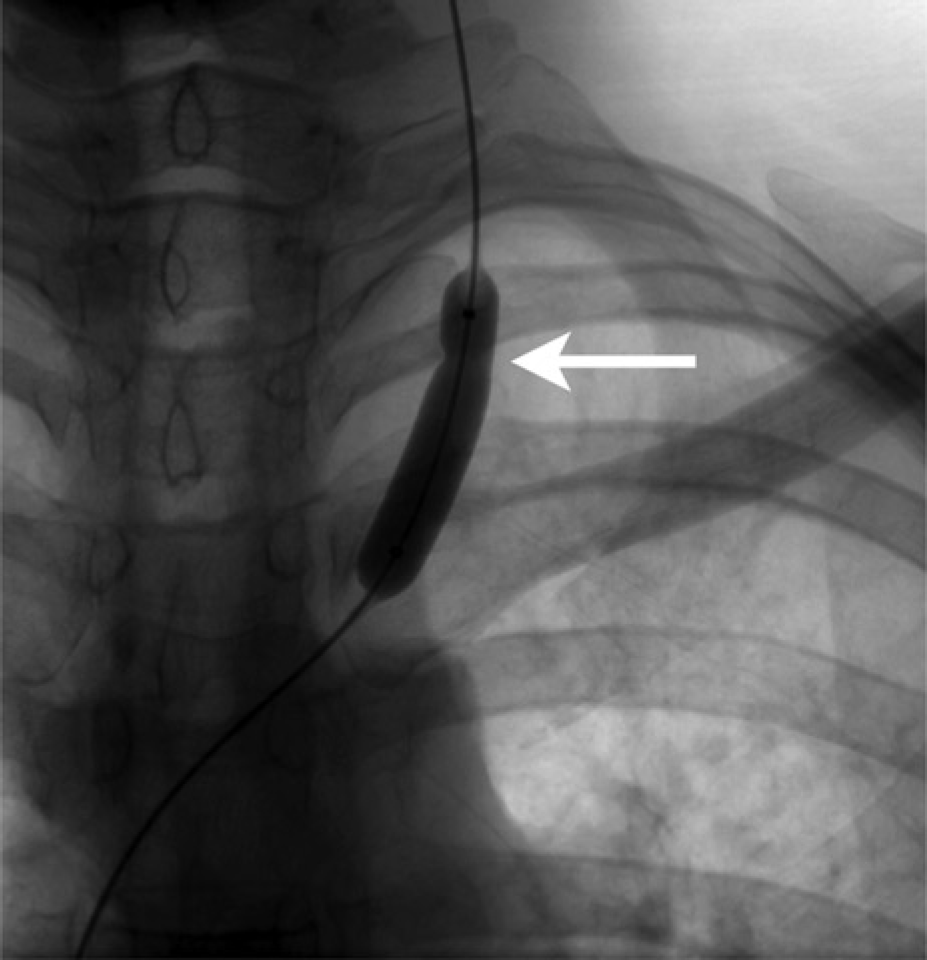
Venoplasty image showing waisting of balloon at site of presumed stenosis
Duplex ultrasound revealed occlusion of the left internal jugular vein with soft thrombus. She proceeded to computed tomography venography of the thorax, neck and brain (Figure 3). The thrombus had not propagated beyond the internal jugular vein and there was no evidence of pulmonary embolism.

Computed tomography venogram following venoplasty demonstrating occlusion of left internal jugular vein (white arrow)
Following a discussion with the neurovascular multidisciplinary team, she was anticoagulated with intravenous unfractionated heparin for five days, but her symptoms progressed to unilateral pulsatile tinnitus, headache and worsening neck pain. She was re-discussed and intervention recommended. The risks of pulmonary embolism with open thrombectomy were judged lower than the risks of thrombolysis and she underwent surgery on day 14 post venoplasty.
The patient was positioned head-down to avoid air embolism. Under loco-regional anaesthesia, a standard anterior approach to the carotid sheath was employed and a longitudinal venotomy made in the internal jugular with minimal bleeding observed. A 2Fr Fogarty embolectomy catheter (Edwards Lifesciences, Irvine, CA, USA) was passed superiorly and fresh thrombus evacuated, with good inflow observed. Inferiorly resistance was felt at the level of the clavicle. A Terumo M 0.90 mm diameter J tipped guidewire (Terumo, Leuven, Belgium) was used to cross the presumed stenosis. A 7Fr 0.89 mm Avanti + introducer (Cordis, Miami, FL, USA) was passed over the guidewire and venous blood was aspirated from the sideport. The decision was made to stop after backbleeding was observed to avoid damaging the brachiocephalic vein. The patient was anticoagulated with warfarin and left hospital four days later.
Anticoagulation was discontinued after six months at which time her coagulation profile was confirmed as normal. At six months she was fully independent and mobile with a stable neurological status despite the jugular remaining occluded sonographically (Figure 4).
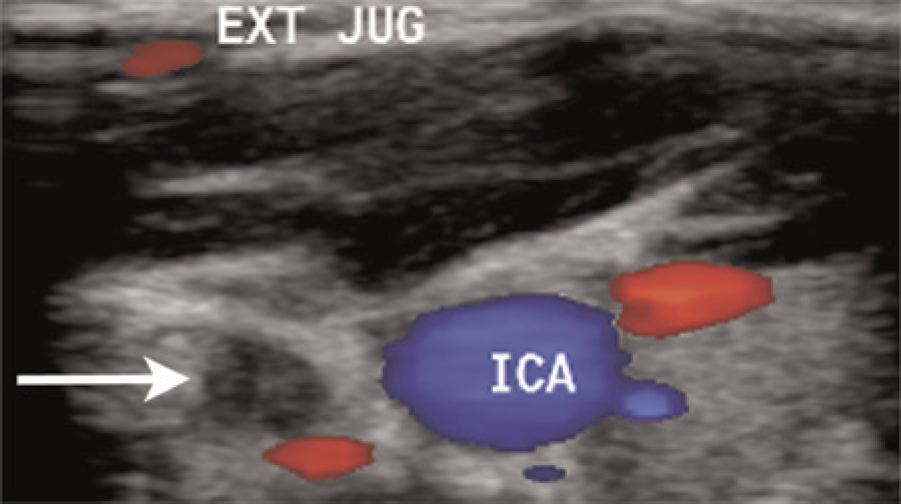
Six month Duplex ultrasound demonstrating re-occlusion of left internal jugular vein (white arrow). EXT JUG, left external jugular vein; ICA, left internal carotid artery
Discussion
This case illustrates several points relevant to the phlebologist. Firstly, patients treated abroad for CCSVI are presenting to their local vascular unit with complications. These patients will be missed from the complications of published case series. Secondly, patients can thrombose the jugular without stent deployment and despite anticoagulation. This is a new finding in this setting. Thirdly, despite the jugular remaining occluded, this patient's functional ability did not change over six months.
Phlebologists need a working knowledge of CCSVI as they are now likely to encounter these complications.