
Abstract
Objectives
Deep vein thrombosis (DVT) is a leading cause of cardiovascular disease. We tested the hypothesis that there is a consensus regarding the treatment of acute DVT among clinicians experienced in DVT management.
Method
A Delphi consensus approach was used to gather expert opinion regarding attitudes towards the treatment of acute proximal DVT and management of specific cases. Strength of preference for various treatment strategies across a number of case scenarios was quantified. Univariate and multivariate analyses were performed to quantify the influence of various factors on treatment modality selected.
Results
Respondents strongly agreed that DVT was a significant health problem and that further research was a priority. A multidisciplinary team approach with access to various treatment strategies was encouraged. Pregnancy and recent surgery independently predicted preference for medical treatment, whereas proximal DVT and May–Thurner syndrome were associated with interventional strategies.
Conclusion
Acute proximal DVT is a significant health problem for which a variety of treatments are available. This study demonstrates that no consensus exists as to the optimum strategy for certain patient groups. Trends in opinion based on local experience and case-series exist, but the results of ongoing randomized trials will ultimately inform best practice.
Keywords
Introduction
Deep vein thrombosis (DVT) is one of the leading causes of cardiovascular disease, and is particularly common among hospital inpatients. It is responsible for a significant amount of additional morbidity and mortality in this population. 1 It is anticipated that the burden of thromboembolic disease will increase over time, due to an ageing population and increasing exposure to risk factors for DVT.
One of the most significant complications following DVT is post-thrombotic syndrome (PTS). Up to 50% of patients with significant proximal DVT will develop this, of which a further 50% will report severe symptoms and 10% will develop leg ulceration. Many patients are of working age with a mean age of 56, meaning that DVT has significant socioeconomic costs. 2 Studies of the natural history of DVT suggest that patients with severe, extensive, proximal DVTs remain at high risk of subsequently developing PTS.3–5 These same studies suggested that where early clot lysis was achieved, valvular function was more frequently preserved resulting in less long-term venous obstruction. 5
These observations have led some clinicians to advocate a more aggressive, interventional approach to clot lysis rather than the traditional strategy of systemic anticoagulation and elastic compression stockings, which may not be effective in reducing clot burden. 6 A range of invasive interventions are available from catheter-directed thrombolysis or mechanical thrombectomy to open thrombectomy. 7 The indications for these treatments are not well defined at present, even though up to 30% of patients with acute proximal DVT may fulfil the necessary criteria for interventional treatment strategies. 8 The precise role of inferior vena cava (IVC) filters and venous stents has yet to be defined. 6
We gathered the opinions of some experts in the field of DVT treatment from several different disciplines regarding indications for treatment and the use of different techniques. The primary objective was to identify areas of consensus and those where opinions differed. The secondary objective was to identify the clinical factors underlying experts’ preference for interventional rather than medical management of acute DVT.
Methods
Delphi consensus: technique and panellists
The modified Delphi consensus is an accepted means of gauging expert opinion regarding the use of new treatment strategies in the absence of existing definitive evidence, and has been used to assess the application of vascular interventions and DVT prophylaxis in the past.9–11 To minimize bias, opinions were sought from experts with an interest in and experience of managing acute DVT from the disciplines of haematology, interventional radiology and vascular surgery.
Delphi questionnaire
The questionnaire was developed in concordance with methods described in previous studies. This included expert opinion in devising the range of questions included in the questionnaire and in designing the clinical vignettes. The questionnaire comprised two stages. The first stage canvassed general opinion of the significance of DVT within the wider context of the UK National Health Service (NHS), satisfaction with the conventional standards of management and the need for research in this field (Table 1). The second stage featured 14 hypothetical patient scenarios with relevant demographic and clinical information. 12 This comprised patient age, thrombus age and DVT location (IVC, iliac, femoral, popliteal, calf) in addition to binary variables including smoking status, use of the oral contraceptive pill, use of anticoagulation at the time of DVT onset, presence of known prothrombotic condition, the presence of malignancy, recent trauma, recent surgery, May–Thurner syndrome, pregnancy or phlegmasia cerulea dolens. In formulating their responses participants were asked to assume that thrombus age could be determined precisely according to the reported onset of symptoms. This was an assumption used to facilitate this study and may not reflect clinical practice.
Visual analogue preference score

Scoring
DVT in the wider context of health care
Respondents were asked to rate their responses from 0 (unsure), then using a Likert scale from 1 (very strongly disagree) to 9 (very strongly agree).
Clinical scenarios
Respondents were asked to rate their responses on a visual analogue score shown in Table 1.
Statistical analysis
Responses to the vignettes were entered into a statistical model to determine key factors in the decision-making process for the management of DVT. Univariate and multivariate analyses were performed of demographic and clinical factors affecting the decision to use conservative management. For univariate analysis, dichotomous factors were analysed using the Fisher's exact or chi-squared tests; parametric continuous factors were analysed using Student's t-test, and nonparametric continuous data were analysed using the Mann-Whitney U test. Significant factors were entered into a binary logistic regression model for multivariate analysis of the decision to use interventional treatment. A forward variable selection procedure was used. Inclusion in the model required a significance level of α = 0.1. Significant results were reported from the model at a significance level of α = 0.05. All analyses were performed using PASW® version 18.0 software (SPSS, Chicago, IL, USA).
Results
Forty-five questionnaires were sent out to experts in the management of DVT across the specialties of haematology, acute medicine, vascular surgery and interventional radiology. There were 35 respondents (7%), but this varied between specialties with the highest rates being seen in interventional radiology, 14 (40%), and vascular surgery, 17 (49%).
DVT in the wider context of health-care delivery
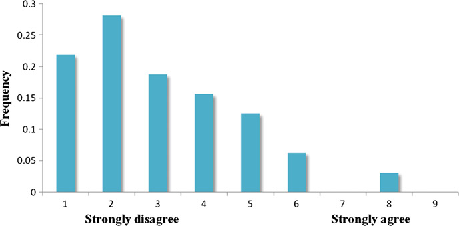
Correspondents agreed strongly that DVT is an important health-care issue (median 9, range 5–9) (Figure 1) and that it placed significant burden on the UK's health-care resources (median 9, range 5–9). Most agreed that new ways of treating DVT should form a priority area for researchers (median 7, range 3–9) and that current treatment pathways are inadequate (median 3, range 1–8) (Figure 2), although there was a greater spread of opinion on these issues and some felt current pathways were adequate.
Deep vein thrombosis is an important health-care problem. Responses to questionnaire on Likert scale from 1 to 9, signifying percentage of respondents that indicated each level of agreement Current treatment strategies are adequate for acute proximal deep vein thrombosis. Responses to questionnaire on Likert scale from 1 to 9, signifying percentage of respondents that indicated each level of agreement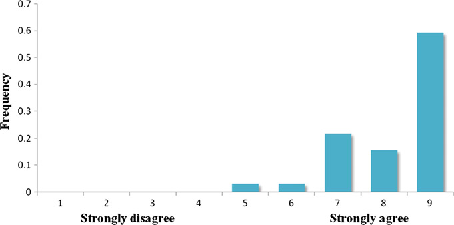
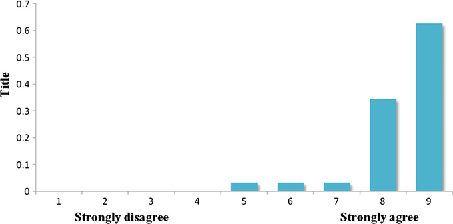
Responses varied widely concerning the efficacy of current anticoagulation regimens in achieving effective thrombus resolution (median 5, range 1–8) or preventing complications such as PTS when combined with compression stockings (median 4, range 1–9) (Figure 3) following acute proximal DVT, displaying a bimodal distribution. Most agreed strongly that interventional options should be routinely available to patients when treating proximal DVT (median 8, range 4–9) and that different strategies should be used for DVT in different anatomical locations (median 9, range 5–9) (Figure 4). Similarly most correspondents felt that patients should be managed by a multidisciplinary team (median 7, range 3–9), and that an inpatient stay was warranted if it would help to improve longer-term patient outcomes (median 8, range 4–9).
Anticoagulation and compression effectively prevent long-term complications of deep vein thrombosis. Responses to questionnaire on Likert scale from 1 to 9, signifying percentage of respondents that indicated each level of agreement Acute deep vein thromboses require different management strategies depending on anatomical location. Responses to questionnaire on Likert scale from 1 to 9, signifying percentage of respondents that indicated each level of agreement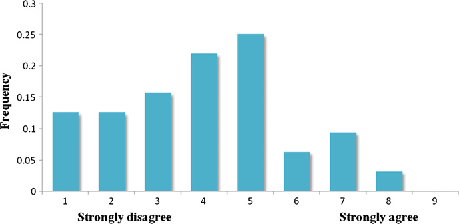
Clinical vignettes
Univariate analysis
In univariate analysis, younger patient age, more recent thrombosis, more proximal thrombus location, male gender, May–Thurner syndrome and the presence of a prothrombotic state or thrombosis despite anticoagulation were significantly associated with a positive decision towards more interventional management strategies. Active pregnancy, isolated femoropopliteal thrombosis, extensive co-morbidity, pre-existing PTS, airline travel-related DVT and recent trauma or surgery were significantly associated with conservative management. Smoking, phlegmasia cerulea dolens, oral contraceptive pill use, malignancy or respondent specialty had no significant effect on treatment strategy selection (Table 2).
Univariate analysis of factors affecting the decision to intervene (per scored patient-scenario)
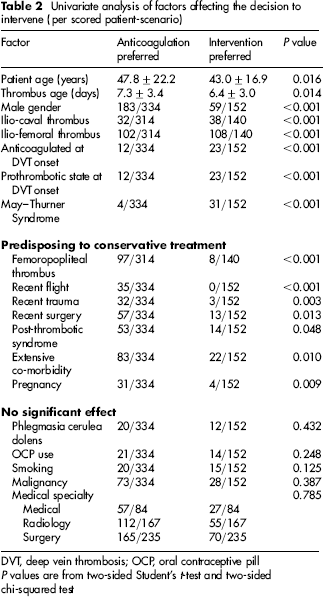
DVT, deep vein thrombosis; OCP, oral contraceptive pill P values are from two-sided Student's t-test and two-sided chi-squared test
Multivariate analysis
Pregnancy (odds ratio [OR] 15.564, 95% CI 4.535–53.424, P = 0.0001) and recent surgery (OR 4.033, 95% CI 1.689–9.630, P = 0.002) were predictors of a preference for medical treatment. Ilio-caval or iliofemoral DVTs (OR 0.218, 95% CI 0.093–0.514, P = 0.0001) and May–Thurner syndrome (OR 0.259, 95% CI 0.075–0.889, P = 0.032) were predictors of a preference for interventional treatment strategies.
Discussion
This study tested the hypothesis that there was consensus among experts in the management of DVT in the UK. The main findings were that there is some variation in general attitude towards the management of DVT, and that given standardized scenarios a variety of therapeutic approaches were advocated by different clinicians. Specific factors were identified that influenced clinicians’ decisions regarding the optimal management of patients with acute DVT in different clinical settings. This probably reflects the lack of high-quality clinical evidence available to guide decisions to treat patients.
Importance of DVT in health-care systems and the need for an interventional approach to acute proximal thrombi
There was strong agreement among respondents that current treatment may be inadequate for high-risk patients with acute proximal DVT. This is a potential target for ongoing research funded by bodies such as the UK National Institute of Health Research. One area of current interest is in assessing the effectiveness of more interventional management strategies for acute DVT such as catheter-directed thrombolysis. Evidence exists to support the hypothesis that early thrombus removal lessens the long-term sequelae of DVT – in cases of DVT managed conservatively in which early spontaneous clot lysis occurred, valvular function was more likely to be preserved. 5 The hypothesis is also supported by a Scandinavian trial of surgical thrombectomy versus anticoagulation alone, which reported improved patency, lower venous pressures, less oedema and fewer PTSs at 10 years’ follow-up in patients randomized to the interventional arm. 13
An interventional strategy of early clot removal would therefore appear an attractive option as this might prevent venous obstruction, valvular incompetence and venous hypertension from developing. 13 This theory was reflected by the expert consensus in this study that current treatment pathways are inadequate for acute proximal DVT and that future treatment of acute proximal DVT should include more interventional modalities.
In the UK alone, approximately 59,000 new cases of DVT arise per year 14 and venous thromboembolism accounts for more deaths than the composite mortality of breast cancer, AIDS and road traffic accidents. 15 The resulting economic burden of patients with previous DVT is significant, costing the UK approximately £640 million per annum. 15 The economic importance of these data was not in doubt among expert respondents, who concurred strongly that inpatient treatment for interventional management of acute proximal DVT is an acceptable use of resources if it improves outcome and that the long-term complications of DVT form a significant burden on the resources of the NHS.
Despite this, and somewhat surprisingly, there was disagreement among respondents on whether anticoagulation alone could lead to effective thrombus resolution. Conventional anticoagulation prevents thrombus propagation, but lacks sufficient fibrinolytic activity to achieve satisfactory clot lysis in patients with severe, extensive, proximal DVTs who remain at a high risk of developing PTS.3–5
Clinical scenarios: which factors influence choice of intervention?
In multivariate analysis, proximal thrombus location was significantly predictive of expert preference for interventional treatment for DVT. This observation matches recommendations by the American College of Chest Physicians (ACCP) and a recent systematic review of thrombolysis for DVT, which suggest that clot removal is limited to proximal IVC and iliofemoral DVT.16,17 The expert consensus reflects strong evidence that caval or iliac thrombus result in higher rates of DVT recurrence 18 and PTS 19 than more distal DVT, meriting aggressive management and a strategy of clot removal.
May–Thurner syndrome, in which the overlying right common iliac artery compresses the left common iliac vein, was significantly predictive of expert intervention in regression analysis. In such examples of external venous compression, there is a good evidence base for the benefit of endovenous stenting to prevent re-occlusion, 20 with technical success rates of 95% and 96% one-year patency following stenting. 21
ACCP guidelines suggest that intervention for DVT provides greatest benefit in young and functionally active patients. 14 Although increasing patient age and the presence of extensive co-morbidity were significantly predictive of conservative management in univariate analysis, surprisingly this observation did not remain significant in multivariate analysis.
Similarly, thrombus age was a significant predictor of treatment choice in univariate analysis, but not the multivariate model. On a univariate basis, it appeared that experts were more conservative than current guidelines, with medical therapy being preferred after only a week of symptoms, and intervention being preferred within one week. Current ACCP guidelines recommend that thrombolysis for DVT should commence within 10 days of symptoms to ensure preservation of valve function. It is likely that this recommendation will be reviewed as it has not been supported by the early results of an ongoing randomized controlled trial (CaVenT) that demonstrated a significant increase in patency at six months’ follow-up after catheter-directed thrombolysis for iliofemoral DVT in patients treated up to 21 days after the onset of symptoms. 22 Furthermore, the USA ATTRACT trial is using 14 days as the cut-off for patient recruitment. 23
Although respondents to the survey were asked to assume that symptom duration reflected thrombus age, this has been shown to be a poor measure of thrombus volume and characteristics. 24 Thrombus itself may be heterogeneous, with older and fresher components, and the lack of expert consensus on this issue may reflect the need for further research to clarify the effect of thrombus age on successful intervention for DVT and the relationship of symptoms to thrombus age.
Interestingly, physician specialty had no significant impact on expert preference for interventional treatment in DVT. This suggests a lack of bias among the physician panel, and is encouraging evidence that trials of intervention for DVT would be well received by all clinicians who manage DVT.
Limitations
Expert consensus can be used to formulate clinical guidelines for practice where it is either impractical or unethical to conduct randomized controlled trials. This study was an exercise in seeking a snapshot of opinion regarding current practice in the setting of existing evidence, so no conclusions can be drawn regarding the appropriateness of the management strategies suggested by the responses to the clinical vignettes.
Conclusion
Acute proximal DVT is an important health problem, placing a significant burden on healthcare resources throughout the world. To date, there is no consensus as to which treatments are most effective in reducing long-term morbidity. It is likely that interventional treatments will play an increasing role in the armamentarium of those involved in the management of DVT, but the precise strategy selected should be tailored to individual patients according the best available evidence. The results of ongoing randomized controlled trials such as CaVenT, ATTRACT and CAVA will be essential in the synthesis of evidence-based clinical guidelines to inform management of acute proximal DVT.