
Abstract
The aim of the study is to report a case of a rare congenital anomaly of the venous system and to emphasize its clinical importance. We describe a case of aplasia of the right common and external iliac veins in a healthy seven-year-old boy who was referred for Doppler ultrasound examination for further evaluation of an abnormal varicosity in the suprapubic region. Colour Doppler ultrasound revealed a dilated, arch-shaped vein. Contrast-enhanced magnetic resonance angiography showed the absence of the right common iliac vein and external iliac vein. It also clearly demonstrated the aberrant venous structure, originating from the right common femoral vein and draining to the left common femoral vein. In conclusion, in our case, the patient's life was threatened because the aberrant venous connection crossing within subcutaneous fatty tissue was not protected from external trauma and possible abdominal surgical interventions. Additional attention should be given to avoid such injuries, which can cause significant haemorrhage.
Introduction
Aplasia/hypoplasia of the deep venous system is a deficiency of the deep veins, including the vena cava, iliac, femoral, popliteal and axillary veins. Superficial veins could be the routes for venous drainage from the limbs. 1 Agenesis of the iliac veins is a rare congenital anomaly. The presence of suprapubic varicose veins must be investigated by clinical examination. They may occur in the case of thrombosis of the iliac vein or a developmental abnormality of the iliac vein. We describe a case of aplasia of the right common and external iliac veins with suprapubic varicosity in a seven-year-old boy.
Case report
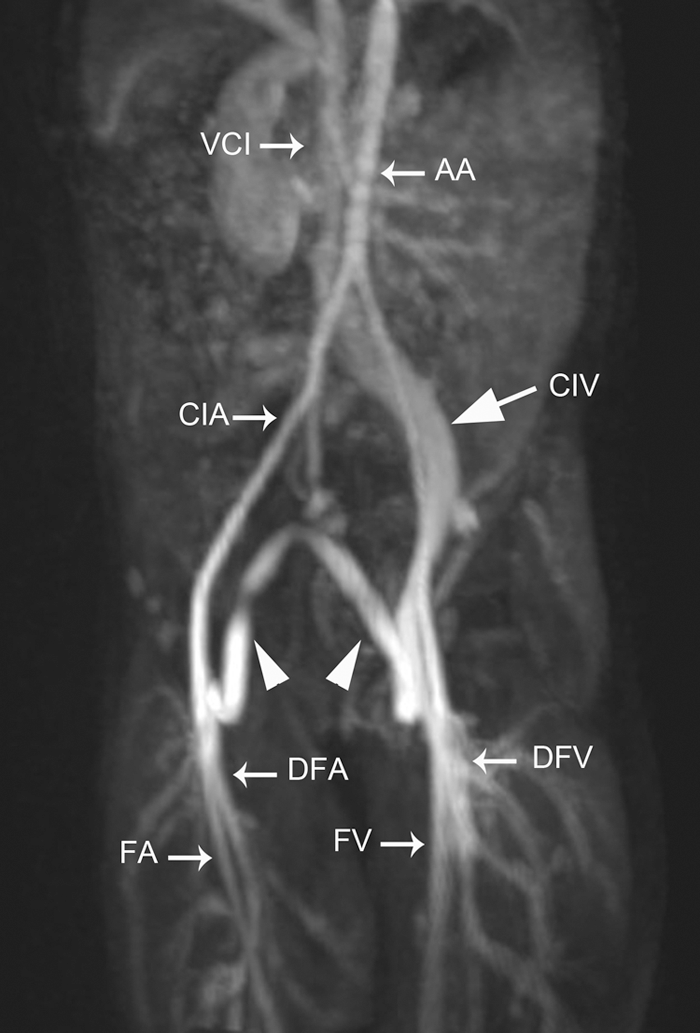
A healthy seven-year-old boy was referred for Doppler ultrasound examination for further evaluation of an abnormal varicosity in the suprapubic region (Figure 1) by a preschool health centre. The parents reported that the child had had this hump since birth. The patient had no previous notable medical history. Colour Doppler ultrasound revealed a dilated, arch-shaped vein. The anomalous course of the vein from the right femoral vein to the left femoral vein passed through subcutaneous fatty tissue at the suprapubic region. Contrast-enhanced magnetic resonance angiography showed the absence of the right common iliac vein and external iliac vein. It also clearly demonstrated the aberrant venous structure, originating from the right common femoral vein and draining to the left common femoral vein. The right internal iliac vein directly drained into the inferior vena cava (Figure 2). Varicosity or swelling in the lower legs was not observed, so additional management was not carried out and follow-up advised.
Photograph of a healthy seven-year-old boy with abnormal varicose veins in the suprapubic region (arrowheads) Right anterior oblique contrast-enhanced magnetic resonance angiography shows an aberrant venous structure (arrowheads), originating from the right common femoral vein draining into the left common femoral vein and a dilated left iliac vein draining into the inferior vena cava (arrow). VCI, vena cava inferior; AA, abdominal aorta; CIA, common iliac artery; CIV, common iliac vein; DFA, deep femoral artery; DFV, deep femoral vein; FA, femoral artery; FV, femoral vein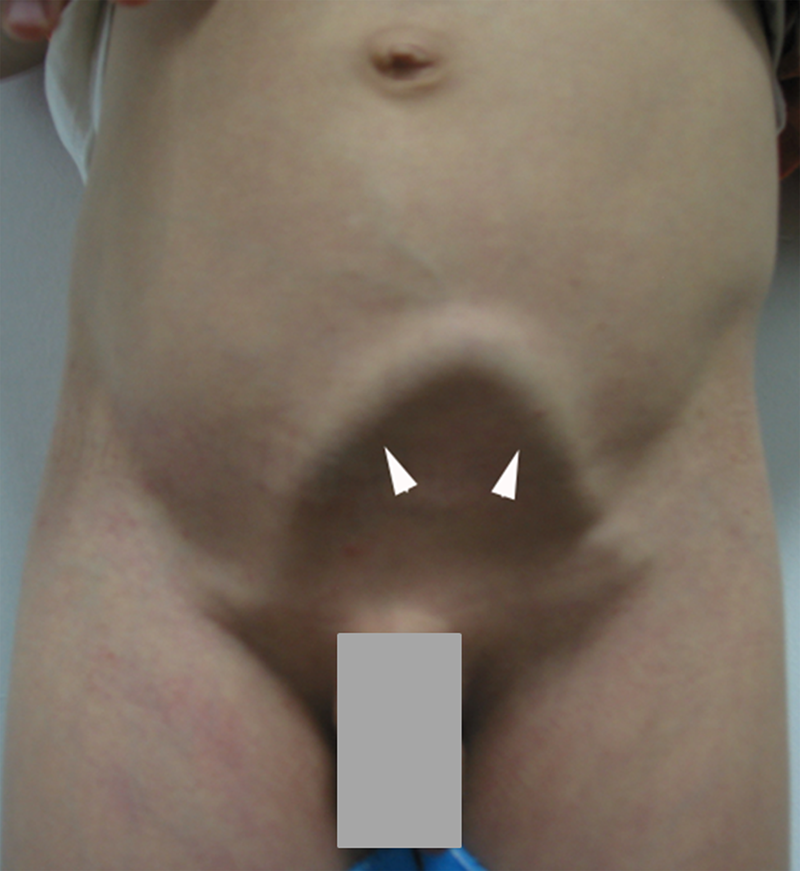
Discussion
The common iliac vein is formed by the union of the external iliac vein and internal iliac vein. It passes upward to the right of the lumbar vertebrae, where it unites with its fellow vein of the opposite side to form the inferior vena cava. 2 Venous drainage of the lower and medial part of the anterior abdominal wall is provided by superficial epigastric veins that empty into the great saphenous vein. 3
Early in the development, the cardinal veins form the main venous drainage system of the embryo body. The anterior cardinal veins drain the cephalic part and the posterior cardinal veins drain the caudal part of the embryo. During weeks 5–7, the sacrocardinal veins provide drainage of the right and left lower extremities after posterior cardinal vein atrophy. Internal and external iliac veins have formed out of this sacrocardinal plexus following diverse transformational processes.4,5 A maldevelopment of these veins or the anastomosis may account for the aplasia of the right iliac venous system, as seen in our case.
Aplasia of the common and external iliac veins unilaterally and bilaterally has been reported. 6 Aplasia of the iliac vein is a very rare congenital anomaly. It can be seen in association with other components of the Klippel–Trenaunay syndrome (KTS) such as capillary malformations and varicosities. 4 Venous abnormalities of the deep venous system such as aneurysmal dilation, duplication, aplasia and hypoplasia also occur in KTS. 6 Abnormalities of the iliac vein and inferior vena cava are uncommon. Some authors reported that 3–6% had an iliac vein hypoplasia or agenesis in the KTS.7–9 The popliteal vein is the most commonly affected deep vein of the lower extremities. 7
Aplasia of deep veins can also be seen with phakomatosis pigmentovascularis, which presents with pigmentary diseases (nevus of Ota and Mongolian spots) and vascular skin disease (nevus flammeus). 10 Patients with anomalies of the iliac vein are susceptible to deep venous thrombosis (DVT). Chung et al. 11 demonstrated that 45 of 56 patients with acute iliofemoral DVT had underlying anatomic vascular abnormalities. Iliac vein agenesis must be distinguished from iliac vein compression syndrome, i.e. May–Thurner syndrome (Cockett's syndrome). This syndrome is characterized by compression of the left common iliac vein by the right common iliac artery, leading to thromboses of the veins. 12
Kutsal et al. reported a case of aplasia of the right iliac vein in a 20-year-old man. It is a similar case with ours but this patient had widespread large capillary hemangiomas, venous stasis ulcers and varicose veins on the right thigh. Koplay et al. reported a case of aplasia of the left external iliac vein and an unusual arch-shaped aberrant venous connection passing through subcutaneous fatty tissue at the suprapubic level between the right external iliac vein and the left common femoral vein in a 38-year-old man. In addition, physical examination and laboratory findings of the patient were normal. In all three cases, including our case, the clinical aspect and anatomical course of the aberrant, arch-shaped vessel superficially passing in the abdominal wall are nearly the same. Both right and left iliac atresia produce the same derivation route. Only Kutsal et al. reported a probable variant of the KTS associated with the iliac aplasia. Koplay and our case were pure iliac malformations which had no other vascular abnormality and hemangiomas. Also both cases had no association with any syndromes.
Magnetic resonance imaging is an imaging technique for diagnosis of this entity that does not involve exposure to ionizing radiation. It can be used to exclude the presence of pelvic masses and deep venous thrombosis while simultaneously demonstrating the anatomical characteristics of this syndrome. 13 CT venography is definitely well suited to describing the normal anatomy and its variations as well as pathologies also providing nice data, and better three-dimensional reconstructions.5,7,14 To minimize the risks of significant venous haemorrhage during laparotomy, it is necessary to be aware of venous embryogenesis and to be able to identify the major venous anomalies.5,15
Conclusion
In our case, the patient's life was threatened because the aberrant venous connection crossing within subcutaneous fatty tissue was not protected from external trauma. The most important risk could be surgical intervention because the importance of the collateral vein is not appreciated if entering the abdomen for other reasons. Additional attention should be given to avoid such injuries, which can cause significant haemorrhage.