
Abstract
Objective
To describe a case of a rare type of venous aneurysm (posterior tibial) with associated pulmonary embolus. We will discuss options and considerations germane to the diagnostic evaluation and possible interventions for this challenging clinical scenario.
Methods
Case presentation and literature review.
Results
A 36-year-old man presented to an outside hospital with a three-day history of left calf pain, acute shortness of breath and syncope elicited by exercise. Work-up demonstrated a pulmonary embolus and a posterior tibial venous aneurysm with mural thrombus. The patient presented to us 18 months later with persistent calf pain seeking an alternative to recommendations of lifelong anticoagulation. The patient was treated with surgical resection of the venous aneurysm with subsequent discontinuation of his anticoagulation. There were no surgical or thrombotic complications of this treatment course and the patient's discomfort improved.
Conclusion
Primary aneurysms of the tibial veins as a cause of pulmonary emboli are rare. A review of the literature suggests that anticoagulation alone does not provide effective amelioration of thromboembolic risk from lower extremity venous aneurysms. We have reported a case of successful surgical treatment of a posterior tibial venous aneurysm and recommend that surgical correction be strongly considered for accessible venous aneurysms.
Introduction
The aetiology of primary venous aneurysms is poorly understood, with few cases reported in the literature. 1 Studies have shown no genetic abnormalities within the underlying connective tissue. However, venous aneurysms have been associated with deep venous thrombosis (DVT) and pulmonary embolus (PE). 2 Venous aneurysms have been reported to be widespread, with the majority occurring in either the neck or extremities with PE usually the first sign of their existence. 1 To our knowledge, there exists only one other report describing PE due to a primary tibial vein aneurysm (TVA). In that case there were multiple bilateral PEs initially treated with anticoagulation alone with recurrent PEs three months later prompting duplex ultrasound, which identified the TVA. 1 We report the case of a primary posterior TVA resulting in PE, successfully treated with open surgical repair.
Case report
A 36-year-old man was evaluated at an outside hospital for a three-day history of left calf pain and acute shortness of breath with syncope. Initial evaluation included computerized tomography (CT) angiography of the chest, which demonstrated an acute PE. Venous duplex demonstrated left posterior TVA with mural thrombus. The patient was placed on elastic compression stockings and lifelong anticoagulation with warfarin with a goal of 2–3 international normalized ratio (INR).
He presented to us 18 months later for evaluation and management of continued left calf pain. Repeat venous duplex imaging demonstrated aneurysmal dilation of the left posterior tibial vein segment in the proximal and mid-calf. The aneurysm measured 1.7 × 2.2 × 9 cm with mural thrombus and preserved flow with distal augmentation (Figures 1 and 2). In addition, he had visible medial upper calf varicose tributaries and an incompetent perforating vein. There were no pigmentary changes or oedema. His INR was 2.1 with a negative hypercoagulability work-up.
Duplex ultrasonography imaging showing left popliteal vein with flow augmentation Duplex ultrasonography imaging showing cross-section of left posterior tibial vein segment confirming posterior tibial vein aneurysm with mural thrombus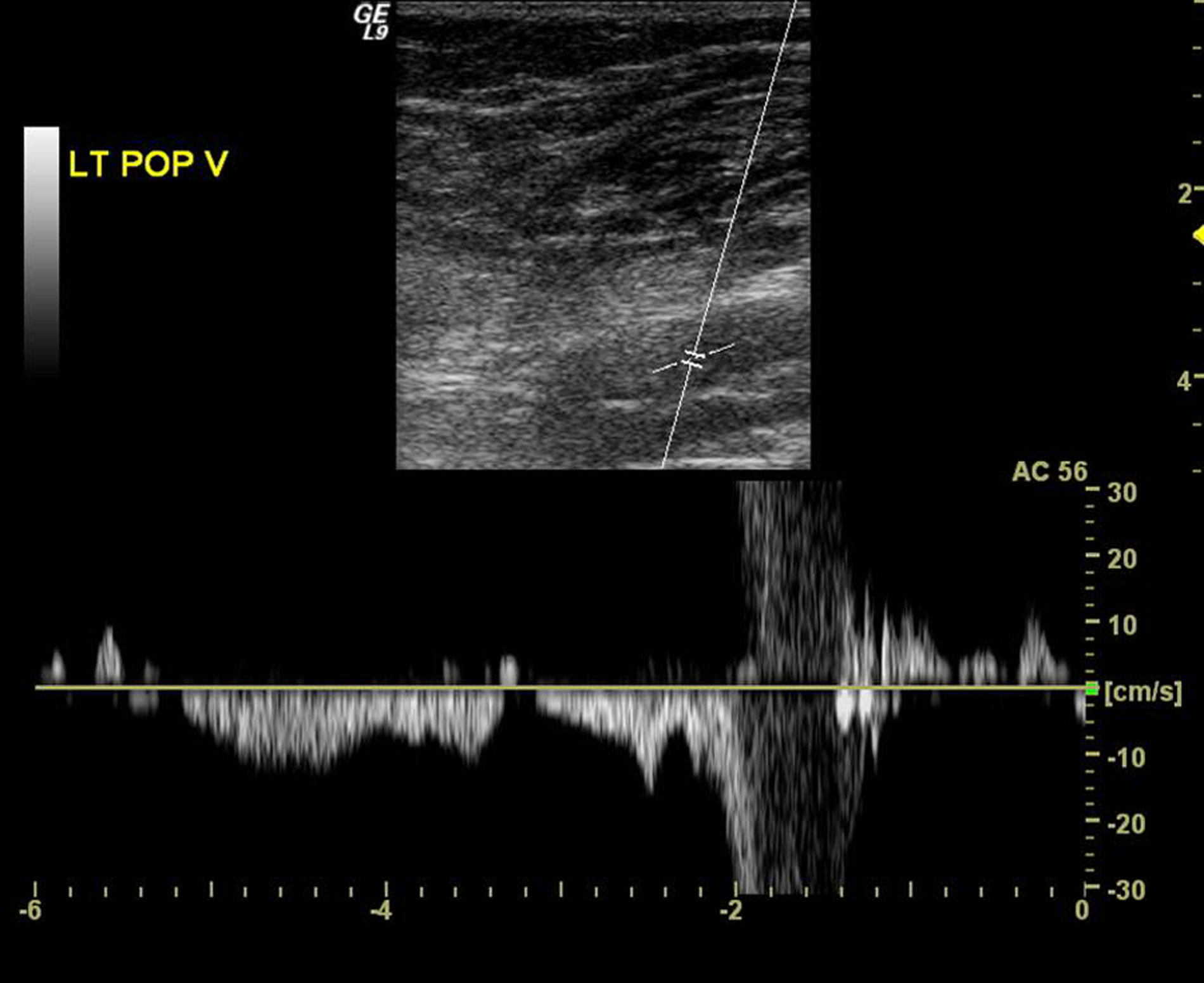

Given the patient's continued calf pain, negative hypercoagulable screen, duplex finding of thrombus within the posterior TVA and history of a symptomatic PE, it was probable that the posterior TVA was the source of the PE during the initial event. His management with warfarin had been well-tolerated with no clinically evident PE. However, the presence of thrombus in the venous aneurysm presented a clear and ongoing risk for future embolic events. Although lifelong anticoagulation therapy was an option, given his young age, the isolated nature of the aneurysm, and the uncertain efficacy of long-term anticoagulation for this entity, surgery was recommended.
Preoperatively warfarin was transitioned to low-molecular-weight heparin (LMWH). Full-dose anticoagulation and a pneumatic tourniquet at the thigh level were utilized intraoperatively for prevention of thrombus embolization. The use of an Esmarch bandage was avoided to further reduce the risk of embolization. The aneurysm was approached through a medial calf incision exposing the posterior tibial neurovascular bundle while ligating varicose tributaries and perforating veins. Two normal-appearing posterior tibial veins and a normal-appearing posterior tibial artery were identified. These vessels were displaced by the very large posterior TVA which was adjacent and deep to the normal vessels. The normal contiguous veins proximal and distal to the aneurysm were ligated. The venous aneurysm was opened longitudinally and several back wall tributaries were suture ligated. The lumen was highly trabeculated with no evidence of thrombus (Figure 3). The vein was trimmed and the venotomy was closed. The patient's postoperative course was uneventful with no evidence of a PE. He had no neurological compromise and his leg pain and edema quickly resolved postoperatively. Follow-up duplex imaging demonstrated patent paired posterior tibial veins with no evidence of DVT. Anticoagulation was discontinued one month postoperatively.
Intraoperative image of lateral venorrhaphy of left posterior tibial vein with visualization of intraluminal complex web and scar formation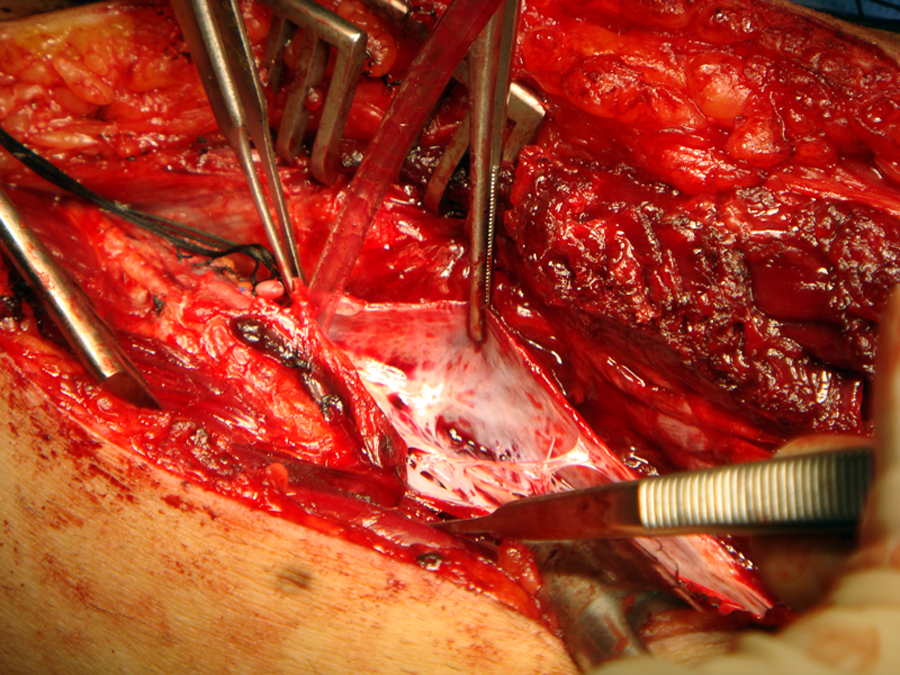
Discussion
Venous aneurysms are defined as segmental venous dilations 1.5–2 times the normal vein diameter and may occur in both the superficial and deep venous systems. The most common symptoms are a painful mass with localized swelling. The diagnosis is typically made using non-invasive imaging such as duplex ultrasonography or axial imaging with CT or magnetic resonance imaging. Phlebography has a more limited role but may be helpful in clarifying complex venous anatomy. Multiple theories have postulated the influence of inflammatory changes, infection, congenital vein wall weakness, mechanical trauma, haemodynamic abnormalities and localized degenerative changes in the formation of TVA. 3
Venous stasis and luminal irregularities associated with venous aneurysms result in a high risk for PE, which can develop in up to 71% of patients. 4 PE may be the initial presenting sign of a venous aneurysm. Even when venous aneurysms are discovered in isolation, predicting the future development of emboli is imprecise since there is no correlation between the presence of intraluminal thrombus and the formation of PE. 5 Furthermore, the long-term efficacy of anticoagulation therapy for the prevention of PE related to venous aneurysms remains to be established. Lower extremity venous aneurysms are prone to embolization since the thrombus within the aneurysm may be forcefully expelled during calf muscle contraction.
Since lower extremity venous aneurysms in general, including posterior TVA, are localized and surgically accessible, we believe that surgical intervention should be pursued in the majority of these cases. Although endovascular therapies are technically feasible using endografts, coils, plugs or endothermal ablation, we contend that for accessible veins such as the tibials, such catheter-based therapies are not ideal. Such potentially less invasive options could be technically challenging given the relatively small size of the posterior tibial veins (PTVs) which would need to be traversed and could pose risks of device embolization (coils), extension of thrombosis (endothermal ablation), injury to access vessels, unintended thrombosis (endografts), failure or recurrence. In considering the technical aspects for surgical repair, one must address whether special precautions are necessary and whether the aneurysmal venous segment can be excluded or repaired. While PE has been identified as the primary risk necessitating surgical treatment, we are not aware of any such intraoperative complications during surgical repair. The risk of PE is real, however, supporting an aggressive surgical approach. Pharmacological prophylaxis is prudent and in our case we provided therapeutic dosing of unfractionated heparin intraoperatively and LMWH in the perioperative period. Gabrielli et al. 1 reported using a retrievable inferior vena cava (IVC) filter for this purpose. While this approach is commonly employed where the risk of embolization seems high based on history, duplex findings including clot burden, location, or morphology (i.e. free-floating iliac vein thrombus), we have not found significant support for this practice in the literature. Neither the PREPIC study nor the ACCP Guidelines support the use of IVC filters in patients without contraindications to anticoagulation.6,7 Considering the manipulation inherent in the muscle retraction required for surgical exposure of the posterior tibial vessels, the expulsion of clot from an aneurysm is certainly a concern. To minimize this risk we utilized a pneumatic tourniquet on the thigh without exsanguinating the leg. Additional manoeuvers including thrombectomy, lysis, femoral vein exposure or IVC filter placement could have been instituted for any intraoperative concerns of thrombus extension.
Options for operative repair include venous aneurysmorrhaphy, exclusion or excision with ligation of tributaries with or without bypass. While popliteal or femoral venous aneurysms should be reconstructed whenever possible to maintain deep venous continuity, TVA can safely be ligated due to the presence of reliable redundant anatomy. 8 After surgical repair we recommend short-term anticoagulation with warfarin to prevent thrombosis. Patients with underlying hypercoagulability or other thrombotic risk factors may benefit from long-term anticoagulation.
Conclusion
We have presented a case of a PE likely resulting from a posterior TVA. Open surgical repair of the venous aneurysm resulted in relief of symptoms and mitigation of the embolic risk of this lesion. For venous aneurysms of the lower extremity, surgical repair is recommended with the choice of technique dictated by the anatomy of the lesion. The use of a pneumatic tourniquet and chemical prophylaxis should be considered for intraoperative thromboembolism prophylaxis.