
Abstract
Objective
Chronic venous disease (CVD) is a common problem in developing and developed countries.
Methods
A cross-sectional study, conducted in two major towns in Serbia, comprised 3225 subjects over 18 years old, enrolled in the survey consecutively by general practitioners (GPs) within their normal framework. Diagnosis of CVD was made by GPs on the basis of symptoms and visual examination. Data on potential risk factors were collected by the use of a questionnaire.
Results
The prevalence of CVD was significantly higher in women (73.7%) than in men (70.1%), although severe forms of CVD were significantly more frequent in men. Risk factors for CVD were age, body mass index ≥25.00 kg/m2, family history of CVD, history of blood clots in veins and ever-smoking in both sexes, and menopause, increased number of child births and physical inactivity in women.
Conclusion
The results obtained suggest the possibility of CVD prevention by modification of some behavioural risk factors.
Introduction
Chronic venous disease (CVD) is a common problem in the Western world and ranges in severity from minor asymptomatic incompetence of venous valves to chronic leg ulceration.1,2 The cause of the disease is probably multifactorial. Genetic predisposition, older age, female sex, obesity, number of pregnancies, oral contraceptive use, hormonal replacement therapy, prolonged standing or sitting, low level of physical activity, smoking, prior episodes of blood clots, leg trauma, flat feet, hernia surgery, history of cardiovascular disease, diet, bowel habits and some others were investigated as possible risk factors for CVD.2–11 However, the results of these investigations were not consistent.
The present investigation is a part of the Vein Consult Program (‘Observational, multicentric, descriptive survey of chronic venous disease – Step 1’), which was organized and sponsored by the Servier Company and performed in co-operation with the International Union of Phlebology. Step 1 of the survey comprised screening of CVD patients by general practitioners (GPs), assessment of their quality of life by the use of a short chronic venous disease quality-of-life questionnaire (CIVIQ-14) and testing of the hypotheses that some of the above-mentioned factors were related to signs and symptoms of CVD. Step 2 is planned to be the following up of patients who after GP opinion have to refer to a venous specialist. In this paper we present the results concerning risk factors for CVD.
Material and methods
The survey was conducted in Belgrade and Nis, two major towns in Serbia. It was performed by 78 GPs (∼15% of all GPs in these two cities) who participated in continuous education concerning CVD. Continuous education comprised theoretic and practical education on phlebology, the aim of which was to improve their knowledge of diagnostics and therapy for CVD, and CVD definition according to the clinical, aetiological, anatomical and pathophysiological (CEAP) clinical (C) classification for chronic venous disorders. All men and women aged >18 years consecutively coming to see the GP for any reason, with the exception of those who came for an emergency, were asked to participate in the study, fully or partly (the patient can agree to take part in Step 1 but decline Step 2). Written consent was obtained from all participants.
For each patient included in the study the GP had to fill out a questionnaire (consultation records form). The following data were collected: demographic characteristics (age, sex); anthropometric and lifestyle characteristics (weight, height, smoking, physical activity); family history of venous leg problems; personal history of blood clots in veins of legs; hours spent standing and hours spent sitting per day; number of child births, current pregnancy, oral contraceptives and hormonal replacement therapy use; symptoms of CVD (heavy legs, pain in the legs, sensation of swelling, sensation of burning, night cramps, itching, sensation of ‘pins and needles’ in the legs); present and previous therapy for CVD, as well as the results of clinical examination of legs. Diagnosis of CVD was made by GPs on the basis of CVD symptoms and visual examination of the lower extremities. The CEAP C classification for chronic venous disorders 12 was used. Diagnosis of CVD in patients who were CEAP C0s was made by a GP after exclusion of other possible causes of existing symptoms. For the purpose of the study, patients with CVD were classified in three hierarchical categories: C0s–C1, C2–C3 and C4–C6.
Statistical analysis
Continuous variables were described as means± standard deviation (SD) or median and categorical variables were presented by counts and/or percentages. The chi-square test was used to compare differences in CVD frequency between men and women. Univariate and multivariate logistic regression analyses were used for estimating the association between risk factors and CVD. All variables, which were according to univariate analysis associated with CVD at a level of P ≤ 0.10, were included in the multivariate analysis. All P values are based on two-tailed tests, and P < 0.05 was considered as significant. Data were analysed using SPSS package version 19.
The study was reviewed and given ethical approval by the Ethics Committee at the Faculty of Medicine in Belgrade.
Results
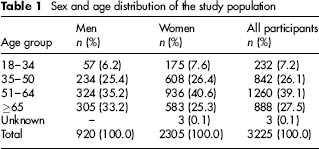
Included in the study were 3225 subjects, 920 (28.5%) men and 2305 (71.5%) women. Only 7% of participants were 18–34 years old, and the greatest number of participants was in the age group 51–64 year (Table 1).
Sex and age distribution of the study population
CVD was present in 70.1% of men and 73.7% of women. The difference was statistically significant (P < 0.05). In comparison with men, women had more frequently CVD CEAP C0s–C1 (P < 0.001), but less frequently CVD CEAP C4–C6 (P < 0.001). Men and women did not differ in the frequency of CVD CEAP C2–C3 (Table 2).
Frequency of chronic venous disease (CVD), by sex
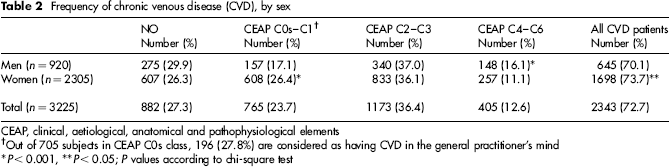
CEAP, clinical, aetiological, anatomical and pathophysiological elements
Out of 705 subjects in CEAP C0s class, 196 (27.8%) are considered as having CVD in the general practitioner's mind
P < 0.001,
P < 0.05;
P values according to chi-square test
Tables 3 and 4 present the distribution of postulated risk factors in men and women with and without CVD. Differences between cases and controls were tested by the use of univariate logistic regression analysis. As in both men and women subjects with CVD and controls significantly differ in their age, univariate analysis of all other risk factors was age-adjusted. The number of women currently pregnant was too small (14 women) to be included in the analysis.
Distribution of postulated risk factors in men with and without chronic venous disease (CVD)
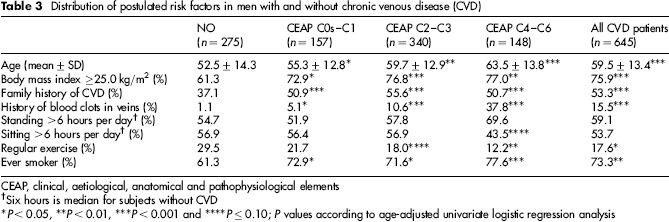
CEAP, clinical, aetiological, anatomical and pathophysiological elements
Six hours is median for subjects without CVD
P < 0.05,
P < 0.01,
P < 0.001 and
P ≤ 0.10;
P values according to age-adjusted univariate logistic regression analysis
Distribution of postulated risk factors in women with and without chronic venous disease (CVD)

CEAP, clinical, aetiological, anatomical and pathophysiological elements
Six hours is median for subjects without CVD
P < 0.001,
P < 0.01 and
P < 0.05;
P values according to age-adjusted univariate logistic regression analysis
Factors that were according to univariate logistic regression analysis associated with CVD at a significance level of P ≤ 0.10 were included in multivariate logistic regression analysis, the results of which are presented in Tables 5 and 6.
Risk factors for chronic venous disease (CVD) in men according to multivariate logistic regression analysis
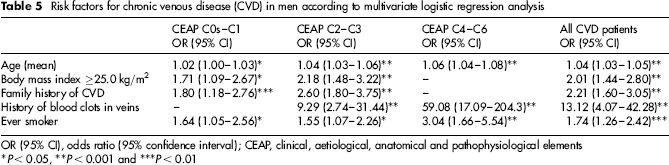
OR (95% CI), odds ratio (95% confidence interval); CEAP, clinical, aetiological, anatomical and pathophysiological elements
P < 0.05,
P < 0.001 and
P < 0.01
Risk factors for chronic venous disease (CVD) in women according to multivariate logistic regression analysis

OR (95% CI), odds ratio (95% confidence interval); CEAP, clinical, aetiological, anatomical and pathophysiological elements
Six hours is median for subjects without chronic venous disease
P < 0.01,
P < 0.001 and
P < 0.05
According to the results of multivariate analysis (Table 5), age, body mass index (BMI) ≥25.0 kg/m2, family history on CVD, history of blood clots in veins and ever-smoking were significantly related to CVD in men. There were some differences in risk factors between CVD categories. A history of blood clots in veins was not related to CVD CEAP C0s–C1 category, but it appeared to be the strongest risk factor for CVD CEAP C4–C6 category. BMI ≥25.0 kg/m2 and family history of CVD were not related to CVD CEAP C4–C6 category. However, in patients with CVD CEAP C4–C6 who had no history of blood clots in the veins, family history of CVD was also an independent risk factor (odds ratio 1.76; 95% confidence intervals 1.03–3.01).
In women (Table 6), age, BMI ≥25.0 kg/m2, family history of CVD, history of blood clots in the veins, ever-smoking and menopause were significantly positively related to CVD. A negative relationship was found with standing more than six hours per day. There were some differences in risk factors between CVD categories. BMI ≥25.0 kg/m2, family history of CVD, ever-smoking and menopause were risk factors in all CVD categories. Age, history of blood clots in the veins and increased number of child births were risk factors for CVD CEAP C2–C3 and CEAP C4–C6 categories, and physical inactivity was a risk factor for CVD CEAP C4–C6 category. Standing more than six hours per day was a negatively related to CVD CEAP C0s–C1 and CEAP C4–C6 categories.
Discussion
In the present study the prevalence of CVD was high (72.7%), significantly higher in women than in men, although severe forms of CVD (CEAP C4–C6) were significantly more frequent in men. Age, BMI ≥25.0 kg/m2, family history of CVD, history of blood clots in the veins and ever-smoking were found to be risk factors for CVD in both sexes, and menopause, increased number of child births and physical inactivity were risk factors for CVD in women.
CVD is not restricted to the elderly, but its prevalence, especially the prevalence of leg ulcers, increases with age.5,9,13–15 In Fiebig et al.'s study 10 age also appeared as a factor of severity of CVD. In the present study, age was an independent risk factor for all CVD CEAP C categories and patients with CVD CEAP C4–C6 were the oldest.
Most studies have shown that CVD is more frequent in women.8,15 –19 Sex-related and lifestyle risk factors, such as genetic factors, obstetric history, work and oral contraceptive use, could be considered at least partly responsible for the higher frequency of CVD in women. Since the first symptoms of CVD appeared in women at a younger age than in men, Fiebig et al. 10 postulated that the higher proportion of female CVD patients may be partially explained by different timings in disease in the two sexes. In some studies, the difference between sexes was small or not statistically significant.5,14,20 In the Edinburgh Vein Study1,21 the prevalence of varicose veins and chronic venous insufficiency was higher in men. Chronic venous insufficiency was also more frequent in men than in women in Scott et al.'s study. 22 In the present study, CVD CEAP C4–C6 category was significantly more frequent in men. The significantly higher frequency of total CVD in women was on account of the CVD CEAP C0s–C1 category.
The role of hormonal factors in the development of CVD has been suggested by several investigations. Hormones and/or other systemic factors may be of importance in the development of postpartum varicose veins. The increasing number of pregnancies7,9,18,23 and child births4,17 was related to increasing CVD prevalence, although in several studies this association disappeared after age adjustment. 2 It seems that alteration in the sex hormone balance have a role in the pathogenesis of CVD even in menopausal women. 24 In the present study, average number of births was significantly higher in women with CVD CEAP C2–C3 and CEAP C4–C6 in comparison with those without the disease. The higher number of births was a risk factor for CVD independent of other observed factors, including age. Menopause was also independently related to all CVD CEAP C categories, especially with the CEAP C4–C6.
The association of CVD with oral contraceptive (OC) use and hormonal replacement therapy is not clear. Fowkes et al. 3 first described the association between OC and reduced prevalence of superficial venous reflux and postulated that sexual hormones influenced venous wall components. Scott et al. 22 and Gourgou et al. 7 did not find a relation between CVD and current OC use. In the study of Górski et al., 25 OC use was inversely related to the prevalence of varicose veins and chronic venous insufficiency. The relationship was not adjusted to parity which was mentioned by the authors as the possible source of bias. In the present study there was no relationship between CVD and either OC use or hormonal replacement therapy. The number of women who used OC and hormonal replacement therapy was very small (9.1% and 5.2%, respectively) to discover any relationship unless it was very strong.
Many studies have found an association between family history and CVD4,7–9,14,26 suggesting a genetic predisposition. Ahti et al. 27 showed that the effect of family history on the risk of varicose veins was affected by differential misclassification. However, Cornu-Thenard et al.'s study, 28 in which the parents of cases (30–40-year-old patients with varicose veins and without history of deep vein thrombosis) and the parents of controls (patients’ spouses) were examined for CVD, demonstrated the prominent role of heredity in the development of varicose veins. According to Hotoleanu and Jurj, 29 gene polymorphisms associated with biochemical and coagulation system abnormalities and genetic factors involved in venous thrombosis leading to secondary chronic venous insufficiency represents the genetic background of CVD. After analysis of CVD patients (2701 subjects) and their families (self-reported disease status in the first-degree relatives – parents and siblings), Fiebig et al. 10 found that the additive genetic component of CVD was approximately 17%. In the present study family history of CVD was significantly more frequently reported by CVD patients. A high proportion of controls, especially women, also reported family history of venous disease.
Smoking was found to be a risk factor for varicose veins in the Framingham study, 16 but only in men, not in women. In a case-control study conducted by Gourgou et al., 7 the lower limb venous insufficiency was significantly associated with tobacco smoking in both men and women, independent of other risk factors. The results of the same study suggested that the risk of venous insufficiency increased with an increasing number of cigarettes smoked per day (dose–effect relation). In Criqui et al.'s study, 4 current smoking was associated with increased rates of severe CVD (CEAP C4–C6 classes) but only in men. In a recent study from Finland, 30 the five-year incidence of varicose veins was in both sexes higher in smokers compared with non-smokers, but the difference was not significant. In the present study ever-smoking was significantly related to all categories of CVD; in both sexes, the association was the strongest in patients from the CEAP C4–C6 category. The mechanisms responsible for the harmful effects of smoking on the venous system are not completely understood. There are several hypotheses based on the knowledge that smoking is a major factor in oxidative stress hypoxia and endothelial damage. 7
A number of studies have found an association between obesity and CVD2,5–7,14 especially in patients with severe skin changes. 31 However, Benigni et al. 32 did not find any relationship between the CEAP C class and obesity in male patients and concluded that obesity was probably a simple reflection of ageing. Many authors considered BMI to be more important in women than in men,2,6,14,33 but there are studies2,34 in which this relationship was found in both sexes. Criqui et al. 4 found increased waist circumference in both sexes with severe CVD (CEAP C4–C6). In the present study BMI ≥25.0 kg/m2 was in both sexes independently significantly associated with all CVD categories, with the exception of a severe form of CVD in men. Fowkes et al. 3 postulated that in obese people intra-abdominal pressure is increased, reducing blood flow in the pelvic veins.
According to Scott et al. 22 and Mohr et al., 35 venous thromboembolism (VTE) is the most important secondary cause of CVD. Heit et al. 36 and Carpentier et al. 37 estimated that as many as 20% of CVD cases developed as a consequence of prior deep VTE, and Kahn et al. 38 found that disease severity was worse in CVD patients with prior VTE. In Clark et al.'s study 5 self-reported deep venous thrombosis was a significant risk factor for varicose veins (OR = 3.19). In the present study, history of blood clots in the veins was the most important independent risk factor for CVD. Odds ratios were 2.61 in women and 13.12 in men for all CVD patients and 7.83 and 59.08, respectively, for the severe form of the disease. Kahn and Ginsberg 11 consider that VTE leads to CVD via the development of venous hypertension as a result of persistent venous outflow obstruction and/or venous valvular incompetence.
Data about prolonged standing as risk factors for CVD have been inconsistent. Laurikka et al., 17 Tüchsen et al. 39 and Gourgou et al. 7 found prolonged standing at work to be an independent risk factor for CVD. In Criqui et al.'s study, 4 standing was a strong risk factor for severe venous disease in women, but not in Maffei et al.'s study. 40 Both Fowkes et al. 3 and Criqui et al. 4 found that sitting was associated with a lower rate of venous insufficiency for women but not for men. However, according to Robertson et al. 6 and Fowkes et al., 2 results of all these studies should be interpreted with caution because of the difficulty in measuring levels of posture. In the present study, prolonged standing and sitting were not related to CVD in men. In women, an inverse relationship was found between CVD and standing for more than six hours per day (median value for control group). This finding seems to be more a consequence of the disease than a cause of disease. There was no association when hours of standing and sitting were analysed as continuous variables or categorical variables (<5, 5–10 and >10 hours).
A low level of physical activity was found to be a risk factor for varicose veins in Brand et al., Framingham's study 16 and Gourgou et al.'s study. 7 In the present investigation physical inactivity was independently positively related to the CVD CEAP C4–C6 category but only in women. Again, it is not clear whether physical inactivity was a cause or a consequence of the severe form of the disease.
The present study has several limitations: cross-sectional design, which makes it difficult to judge the causal relationship; diagnosis of CVD made by GP and not confirmed by specialist; diagnosis of CVD made on the basis of symptoms and clinical, visible changes, and not on functional ones; data on postulated risk factors were self-reported and consequently the possibility of recall bias cannot be excluded; and data on positional factors, such as standing and sitting, were not detailed enough for evaluation of their importance as risk factors.
Although some risk factors for CVD are unchangeable, the results obtained suggest the possibility of CVD prevention by modification of behavioural risk factors such as obesity, smoking and physical inactivity.
Footnotes
Acknowledgement
This work was supported by the Ministry of Science and Technological Development, Republic of Serbia, through contract no. III41002 (2011–2014).