
Abstract
Aims
To review the results and cost of a rolling ultrasound-guided foam sclerotherapy (UGFS) treatment programme for patients with chronic superficial venous insufficiency.
Method
A prospective study of a rolling treatment programme where patients were offered unlimited follow-up at intervals of 6–8 weeks and further (top up) UGFS when necessary, until occlusion criteria were met.
Results
A total of 213 lower limbs with complete follow-up were included in the study. Median (range) age was 57 (16–94) years, maximum diameter of varicose vein was 10 (3–18) mm, C of CEAP (clinical, aetiological, anatomical and pathological elements) was 4 (2–6), number of treatment sessions was one (1–4) and follow-up was three (1.5–33) months. Satisfactory occlusion could not be achieved in nine (4%) limbs. The ratio of odds (95% CI) for requiring more than one treatment session was 3.58 (1.46–8.77), P = 0.002 for great saphenous varicosity and 2.11 (1.13–3.94), P = 0.015 for age 50 or more.
There were 20 (9.3%) immediate and 63 (29.5%) delayed adverse effects. All were minor except for one cutaneous nerve injury, one pulmonary embolism and one infected haematoma. The ratio for odds (95% CI) for post-treatment skin discolouration was 2.59 (1.14–5.87), P = 0.017 for women and 1.32 (1.02–1.71), P = 0.032 for increasing sclerosant volume used. Service line costing per completed treatment episode was £115.22 (€130.07, $188.60).
Conclusion
UGFS in a rolling treatment programme is safe and can achieve high occlusion rates at a low cost. Patients above the age of 50 with great saphenous varicosity are likely to require more than one treatment session.
Introduction
Ultrasound-guided foam sclerotherapy (UGFS) has been shown to be effective in treating primary and recurrent varicose veins giving comparable results to other endovenous treatments and surgery.1–3 It has also been used successfully in the treatment of complicated varicose veins with signs of chronic venous insufficiency including ulceration.4,5 In a study by O'Hare and Earnshaw, 6 25% of UK vascular surgeons use UGFS to treat varicose veins. This is despite the fact that most of the data available in support of this practice come from observational non-randomized studies with wide variations in reporting standards.
Advocates of UGFS would agree that one of its key advantages is its low cost. To the authors’ knowledge, no detailed costing of this procedure exists in the literature.
This paper presents the experience of a single centre in the use of UGFS within a rolling varicose veins treatment programme. Detailed costing analysis as per service line reporting costing method 7 is also included.
Materials and method
Lower limbs treated with UGFS between November 2006 and February 2010 by a single surgeon in a district general hospital were included in this study.
Inclusion criteria for treatment of varicose veins with UGFS included: clinical CEAP (clinical, aetiological, anatomical and pathological elements) score of ≥4 or clinical CEAP score of <4, if accompanied by above-knee thrombophlebitis or bleeding from varicose veins. These restrictions were placed by the primary care trust due to limitations on funding. Patients who did not qualify for intervention were discharged with advice regarding compression hosiery. All patients meeting the inclusion criteria were offered UGFS as the only primary treatment. Exclusion criteria for this cohort were recent deep vein thrombosis (DVT) and contraindications for the use of compression hosiery. Patients were incorporated in a rolling treatment programme where they were offered unlimited follow-up at intervals of 6–8 weeks. Further UGFS injections were given until successful treatment was achieved. Figure 1 shows the treatment flow chart.
Ultrasound-guided foam sclerotherapy treatment protocol
The anatomies of the varicose veins were determined with duplex scanning prior to treatment. The classification of great saphenous vein (GSV) or small saphenous vein (SSV) trunk varicosity was still valid if the main point of reflux was through an incompetent perforator along the course of the trunk vein as opposed to the saphenofemoral junction (SFJ) or saphenopopliteal junction (SPJ). For the purpose of this study, the GSV/SSV trunk varicosity definition included the main trunk and any associated extrafascial branches. Other varicose veins included aberrant and non-specific varicose veins that were not in relation to the main saphenous trunks.
Foam was made up of 3% sodium tetradecyl sulphate (STS, Fibrovein, CP Pharmaceuticals, Wexham, UK) and air in a ratio of 1:4 using the standard Tessari Technique. 8 The patient was positioned in a reverse Trendelenburg position (10° tilt), supine for the GSV and prone for the SSV. The vein was canulated under ultrasound guidance using a size 19 Gauge butterfly syringe. If cannulation was unsuccessful due to depth of the vein, a longer 21 Gauge (40 mm) hypodermic needle was used instead. A test injection was verified with the ultrasound probe prior to administration of the full amount of foam to fill the varicose vein. On average, this corresponded to 5 mL for SSV and 8–10 mL for GSV. A maximum of 12 mL of foam was used in any one session. Pressure was applied to the terminal valve of the vein, at the time of injection, to prevent efflux of foam into the deep veins. The number of punctures varied according to the target vein: one puncture for SSV and two for GSV (1 above knee and 1 below knee).
Immediately after treatment, the lower limb was wrapped with a short stretch bandage (Coban™, 3M, St Pauls, MN, USA) for 24 hours, following which patients were asked to wear the provided above-knee grade 2 compression hosiery for four weeks. Patients with ulceration were advised to continue with standard four layer compression bandaging.
Outcome measures
Patients were reviewed six to eight weeks after each treatment session by the same surgeon. They were assessed clinically and underwent duplex scanning of the treated limb at each visit. Successful treatment was recognized as complete occlusion of the saphenous trunk or other varicosity from the level of incompetence between the superficial and deep system. At this point the patient would be discharged. If complete occlusion was not achieved, further UGFS injections were given and the treatment cycle repeated. Treatment was reserved only for truncal varicose veins and associated main branches and not for superficial telangiectasia. Patients were asked for any possible early or late adverse effects at every visit.
Data pertaining to patient demographics, duplex findings, treatment details, session time and outcomes were recorded in a comprehensive prospective database. Data were analysed using SPSS software (version 12.0; SPSS Inc., Chicago, IL, USA).
Costing method
Cost analysis was performed as per service line reporting. 7 The following variables were recorded for the 213 treated lower limbs: total number of sessions required to treat all of these limbs, total time recorded for all treatment sessions, total volume of foam used and other consumables for all treatment sessions. The total cost of consumables and staffing were generated for treating 213 lower limbs and a mean average of cost was calculated for treating one lower limb from this value.
Results
Two hundred and twenty lower limbs were treated between November 2006 and February 2010. Seven lower limbs were lost to follow-up before being discharged and were not included in the analysis.
Demographic, clinical and treatment data for 213 limbs (complete follow-up) with varicose veins treated by UGFS
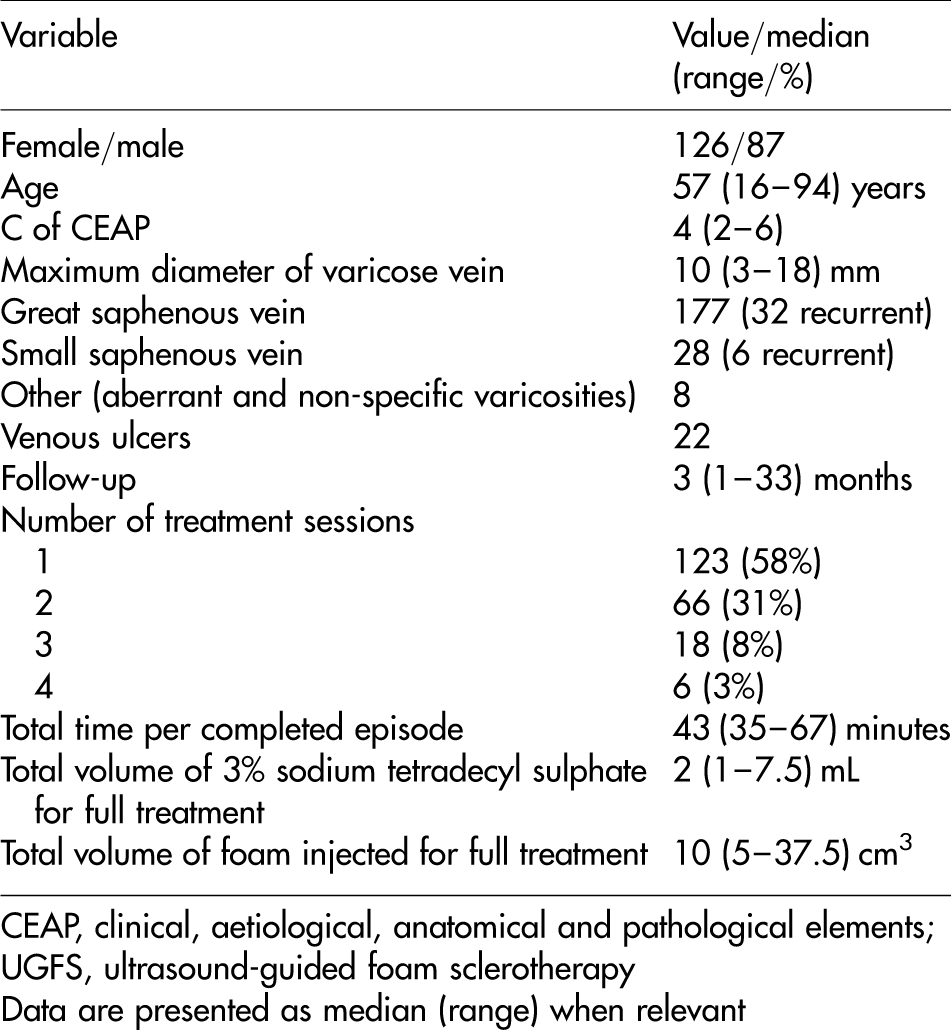
CEAP, clinical, aetiological, anatomical and pathological elements; UGFS, ultrasound-guided foam sclerotherapy
Data are presented as median (range) when relevant
Details of nine limbs with incomplete or abandoned UGFS treatment

UGFS, ultrasound-guided foam sclerotherapy
Details of immediate and delayed adverse effects in 213 UGFS treated limbs
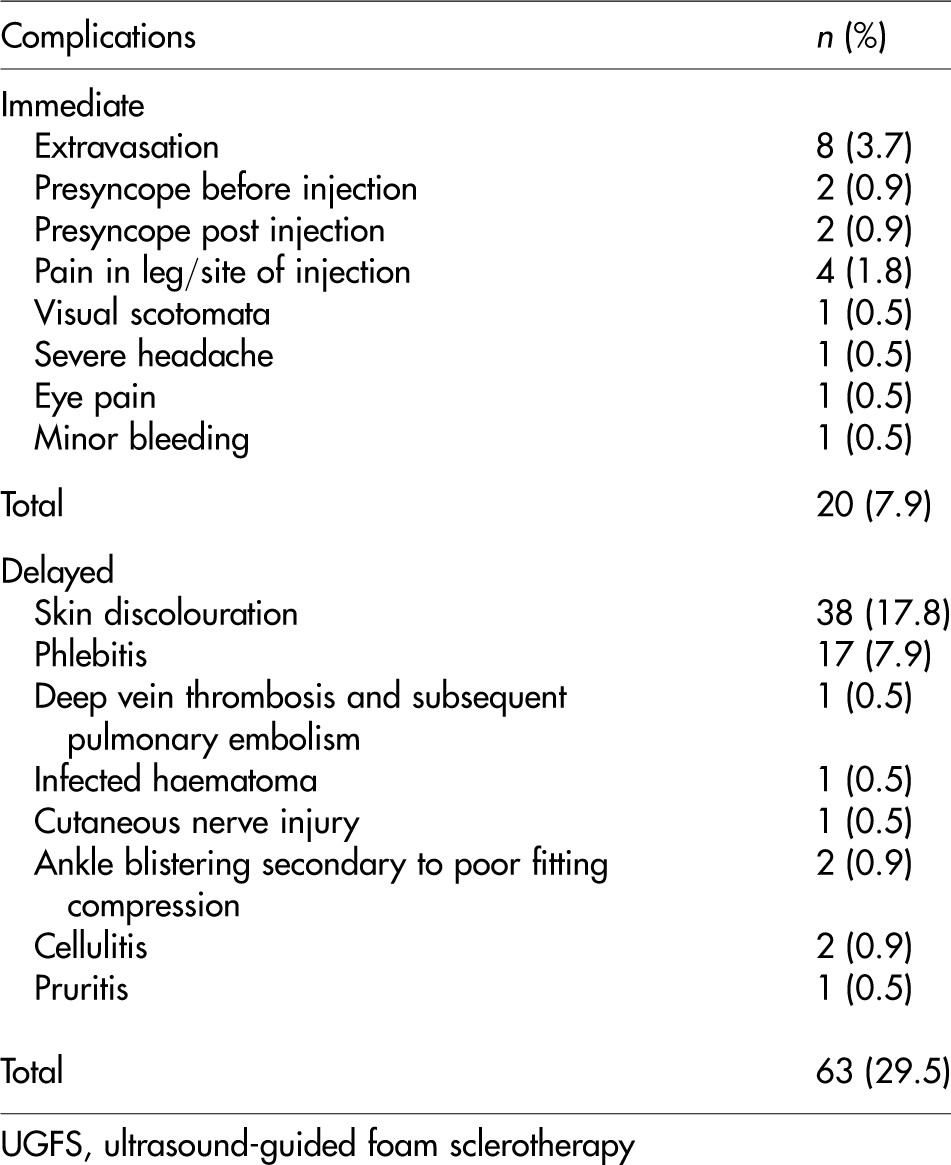
UGFS, ultrasound-guided foam sclerotherapy
Skin discolouration accounted for the majority of delayed adverse effects (17.8% of all treated limbs). There was one reported complication of pulmonary embolization secondary to post-treatment DVT. The male patient presented 10 days after receiving 10 mL of foam (2 mL 3% STS and 8 mL air) for a great saphenous varicosity.
Twenty-two treated limbs had venous ulceration. Median (range) age for this group was 69 (50–94) years. Seventeen (77%) had complete healing of their ulcers within three months. The remainder showed variable degrees of improvement.
Odds ratios for requiring more than one treatment session and for the development of skin discolouration in 213 UGFS treated limbs

UGFS, ultrasound-guided foam sclerotherapy; CEAP, clinical, aetiological, anatomical and pathological elements
*Incremental increase by one unit
Service line costing of 213 completed episodes of UGFS
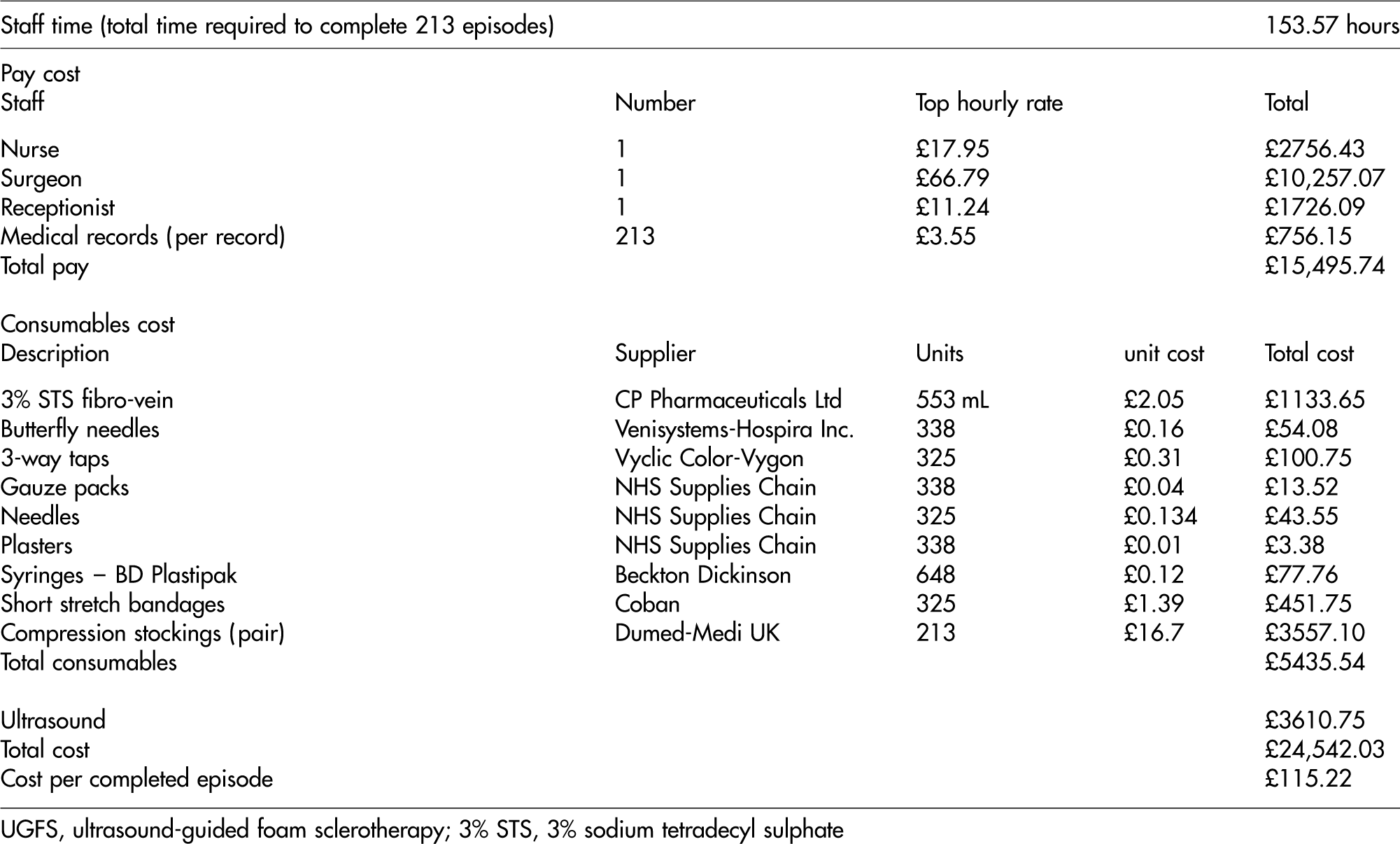
UGFS, ultrasound-guided foam sclerotherapy; 3% STS, 3% sodium tetradecyl sulphate
Discussion
This paper reports the experience of a single centre in treating 213 lower limbs with varicose veins through a rolling programme of UGFS. In all, 96% of this cohort had complete occlusion at a median follow-up period of three months.
UGFS is a minimally invasive office-based treatment for superficial venous insufficiency. Unlike other endovenous and surgical methods, UGFS success as measured occlusion/exclusion of the target vessel is not immediately apparent.
Early follow-up to quantify treatment success by duplex scanning is therefore desirable for this method. In addition, the facility to offer completion UGFS to those with incomplete occlusion should also be available as part of a comprehensive UGFS service. With these criteria in mind, a rolling treatment/follow-up/treatment programme appears to offer the ideal set-up for a UGFS service. In this cohort, all patients were offered an unlimited number of follow-up/treatment sessions until they either fulfilled the discharge criteria or were deemed unlikely to benefit from further treatment attempts.
Few reports have outlined the outcome of UGFS in varicose veins with high clinical CEAP scores. In this cohort, the median C score was 4 (119 limbs). In all, 42% of the whole cohort required more than one treatment session. Neither the incremental rise in clinical severity nor the incremental rise in varicose vein size appeared to predict the need for more than one treatment session. This finding is similar to that by O'Hare et al., 4 who could not establish a relationship between occlusion rates and two groups of clinical severity (C ≥ 4 vs. C < 4) and two groups of varicose veins size (<7 mm vs. ≥7 mm). The evidence that neither varicose vein size nor clinical severity influence the response to UGFS is further supported by the findings of Coleridge Smith. 9
While clinical severity and vein size do not appear to correlate with the response to UGFS, the length of the treated varicosity (great saphenous vs. small saphenous) and advancing age were factors associated with increased odds for repeated injections in this study. This is of particular relevance to the treatment of small saphenous varicosity. In a review by Perrin and Gillet 10 it was suggested that unless a grossly incompetent SPJ stump is present, UGFS is the most appropriate treatment. The experience from this study and from others 11 suggests that one UGFS treatment session is usually adequate to treat any degree of small saphenous insufficiency. However, long-term follow-up is required to detect rates of recurrence.
Out of the 22 limbs with venous ulcers treated in this cohort, 17 had complete healing within three months. The patients with complete healing had failed treatment with standard four-layer compression bandaging alone, prior to additional treatment with UGFS. With longer follow-up, Darvall et al. 5 achieved 96% healing of venous ulcers in 28 lower limbs undergoing UGFS Our findings support the effectiveness of UGFS in treating venous ulcer disease in the short term. Further follow-up is required for this series in order to assess long-term outcomes and recurrence of ulceration.
The safety of UGFS remains subject to debate. This is mainly due to a number of reported cerebrovascular and venous thromboembolic (VTE) events related to this procedure.12,13 A controlled multicentre prospective study including 1025 patients studied the side-effects of UGFS. Eleven thromboembolic complications occurred; including 10 DVTs and one pulmonary embolism (PE). One transient ischaemic attack with complete resolution in 30 minutes was also diagnosed. 9 In this series, one transient visual scotoma was diagnosed with no subsequent long-lasting complications. One patient was diagnosed with a DVT and subsequent PE after treatment with UGFS. Further investigations revealed the underlying myeloproliferative disorder. Since this condition significantly increases the risk of VTE, in hindsight, we would not have offered him this procedure.
Immediate adverse effects were more likely in men; however, the wide spectrum of these events makes it difficult to draw any conclusions from this correlation. The most common adverse effect in this cohort was the development of skin discolouration (17.8%). This incidence is in keeping with other reports.12,13 Female gender and incremental increase in 3% STS volume used were the only factors associated with skin discolouration in this study. While the use of less concentrated sclerosant might reduce the incidence of skin discolouration, most of these skin changes resolve completely by one year. 2
In this cohort, the cost for a completed episode of UGFS was £115.22 (€130.07, $188.60). The actual cost is also influenced by the treatment of any complications, treatment of disease recurrence and any hospital infrastructure costs which are not accounted for in this evaluation. Furthermore, different units may have different practices (use of an ultrasonographer, use of a different sclerosant, follow-up frequency, etc.). However, such differences are unlikely to change the overall cost significantly. This low cost allows clinical freedom in offering patients more follow-up and treatment opportunities.
In conclusion, a rolling treatment programme for lower-limb venous insufficiency using UGFS is safe, achieves high occlusion rates at three months and is of low cost. Neither venous trunk size nor the degree of clinical severity should be considered as contraindications to treatment by this method. Although most patients within such a programme will require only one treatment session, patients over the age of 50 with great saphenous varicosity are more likely to require additional sessions.
Footnotes
Acknowledgements
No further contributions that need acknowledgement.
No sources of financial or material support.
No conflicts of interest.