
Abstract
Objective:
Immunohistochemical techniques have revealed the presence of vascular endothelial growth factor (VEGF) in the epidermis of patients with chronic venous disease (CVD). Our objective was to perform a quantitative analysis of the VEGF gene transcription in tissues that are potential sources of this factor (skin, varicose veins [VV] and great saphenous vein [GSV]) in patients with CVD.
Methods:
In all, 212 skin and venous tissue samples were collected from patients diagnosed with CVD and controls. The VEGF gene expression was analysed using quantitative realtime polymerase chain reaction (PCR).
Results:
The skin VEGF expression was lower in the CVD group than in the control group (P = 0.04). There were no significant differences between the insufficient GSV of the CVD group and the control healthy vein (P = 0.22). There was a greater expression of VEGF in the VV of the CVD group than in the control healthy vein (P = 0.03). Comparison of the VEGF expression between the different tissue types in the CVD group revealed significant differences between the skin and GSV (P = 0.02) and between the skin and the VV (P = 0.004), and between the VV and the GSV (P = 0.02).
Conclusions:
The results of the present study show an over-expression of VEGF gene in the VV tissue of patients with CVD. Based on the data in patients with C2 disease, the VVs appear to be the source of increased VEGF expression.
Introduction
Chronic venous disease (CVD) is a process affecting the venous system of lower limbs and causing deep, superficial and perforating vein incompetence. This process results in venous hypertension and produces the typical symptoms and signs of the disease, such as pain, swelling, heaviness, skin changes and ulceration.
The physiopathology of primary varicose disease is complex and considered a multifactorial process with numerous described genetic, hormonal and mechanical risk factors.1,2
There is currently strong evidence indicating that CVD is an inflammatory disease, but the mechanism triggering the inflammatory cascade is yet to be determined.3,4 The onset of this disease is a loss of control over venous homeostasis, irrespective of the trigger mechanism.
Vascular endothelial growth factor (VEGF) has an important role in maintaining vascular integrity and reactivity. 5 In primary varicose disease, the capillaries in the skin are dilated and tortuous, and may acquire a glomerular appearance with capillary endothelium proliferation. 6 VEGF could explain this proliferation. 7 It has also been shown that it produces a large increase in microvascular permeability. 8 This increased permeability could trigger the inflammatory cascade and, in turn, VEGF induces the expression of adhesion molecules such as intercellular adhesion molecule-1, vascular cell adhesion molecule-1 and E-selectin. 9
Immunohistochemical techniques have revealed the presence of VEGF in the epidermis of patients with CVD, 10 as well as elevated plasma levels which increase with disease severity.11,12 The tissue/s where this VEGF is over-transcribed and produced still remains unknown in the primary varicose disease. This information could allow us to gain a better understanding of the molecular causes of varicogenesis, in order to conduct new studies and design better treatment strategies.
Our objective was to perform a quantitative analysis of the VEGF gene transcription in tissues that are potential sources of this factor (skin, varicose veins [VVs] and great saphenous vein [GSV]) in patients with CVD.
Methods
Overall, 212 skin and venous tissue samples were collected from patients diagnosed with CVD and controls. The samples were obtained from different areas: skin with telangiectasias, VVs and GSV from patients with CVD, and GSV and healthy skin from control subjects.
The study included 84 subjects, 44 with CVD and 40 controls. All included subjects signed an informed consent form. The study was approved by the Ethics Committee of Getafe University Hospital.
The 44 patients with primary varicose disease, all over 18 years of age (mean age of 47.2 ± 9.9), were recruited from the Vascular Surgery Outpatient Department. All of them presented symptomatic C2 grade CEAP (clinical, aetiological, anatomical and pathological elements) classification CVD. 13 The other inclusion criteria were: no previous vein surgery and no evidence of deep vein thrombosis event. The patients were only included if they had telangiectasias, VVs and GSV insufficiency, verified by colour flow duplex ultrasound, and all were candidates for undergoing elective crossectomy with stripping of the GSV.
Using colour flow duplex imaging in the longitudinal view, the saphenous valvular function was evaluated in all subjects included at the femoral junction, thigh and calf levels. Flow direction was noted during the Valsalva manoeuvre and proximal and distal muscular compressions. Reflux was quantified based on maximum reverse velocity and/or valve closure time from the Doppler spectral tracings obtained in the longitudinal section. Reflux was considered significant if a peak velocity greater than 30 cm/second or a valve closure time greater than 0.5 seconds was detected.14,15
During the surgical intervention, samples were collected from skin areas with visible telangiectasia, GSV in the saphenofemoral junction (SFJ), and VVs in the patients included in the CVD group.
The study design was based on the hypothesis that the epidermis could be the source of the angiogenic stimulus in CVD. It is just in the skin areas with telangiectasias where VEGF should be over-expressed and more highly transcribed than in others skin areas without telangiectasias in patients with CVD. Thus, it exclusively included patients with GSV reflux and VVs that showed telangiectasia, and, thus, skin samples from areas with telangiectasia were collected in these CVD group patients in order to determine a potential over-expression of VEGF in these skin areas.
We obtained the samples of GSV from the SFJ portion in all the cases in order to control possible bias. It has been proved by Hollingsworth et al. 16 that when the SFJ is competent and functional, transcription of the VEGF gene is not affected by the position from which the vein segment is taken. On the other hand, in the sections from GSV in which the SFJ is incompetent, the levels of transcription of VEGF are elevated overall in all the portions (proximal, mid- or distal portion).
The controls were 40 patients (mean age of 65.7 ± 9.4) who underwent autologous vein graft bypass for chronic lower-limb ischaemia, without signs or symptoms of CVD and without GSV insufficiency evidenced by colour flow duplex ultrasound showing that the vessel was disease-free and without valvular incompetence in any segment. Samples were obtained from the GSV in the SFJ portion after it was removed for the graft, and from healthy skin.
Overall, 212 tissue samples were collected and immediately introduced into RNA-later solution (Sigma, St Louis, MO, USA), stored for 24 hours at +4°C and then frozen to - 80°C until processing. The samples were later thawed and homogenized using a MagNA Lyser electric homogeniser (Roche, Basel, Switzerland). The RNA was obtained using the commercial RNAeasy Fibrous Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer's instructions.
The amount of purified RNA was determined using spectrophotometry at 260 nm in a Nanodrop analyser (ND-100; Nanodrop Technologies, Wilmington, DE, USA). The purity was verified according to the ratio of 260/280 nm measurements, such that values between 1.8 and 2.1 indicated that the quality of the RNA obtained was optimal and suitable for the quantitative realtime polymerase chain reaction (qRT PCR).
The VEGF gene expression was analysed using qRT PCR (Real Time PCR 7500 Fast, Version 2.0, Applied Biosystems, Carlsbad, CA, USA). For the qRT PCR study, 1 μ;g of total RNA was reverse transcribed to complementary DNA (cDNA) using the commercial High Capacity cDNA Reverse Transcription Kit (Applied Biosystems). Afterwards, 30 ng of cDNA was used as a mould for the realtime PCR in a final volume of 12 μL, which contained TaqMan Master Mix Universal Fast (2x) (Applied Biosystems, Foster City CA, USA) plus the specific TaqMan (20 x) test for the gene studied. Amplification was for 35 cycles of 94°C for 45 seconds, 58°C for 45 seconds and 72°C for 60 seconds. The gene studied was VEGF (Hs009055_ml) using the following primers: forward 5′-TCAAGGACAGAA GAGACTATAAAATTTGC-3′ and reverse 5′-ACTCCAAACTCCTTCCCCACAT-3′. The 18S gene of ribosomal RNA (Hs99999901ml) with the following primers: forward 5′- GTAACCC GTTGAACCCCATT-3′ and reverse 5′- CCATCC AATCGGTAGTAGCG- 3′ and the house-keeping ciclofilin gene with primers: forward 5′-AATGC TGGACCAAACACAAA-3′ and reverse 5′-CCTTC TTTCACCTTCCCAAA-3′, were used as an endogenous control.
The relative quantification of the VEGF gene expression was performed using the delta delta CT (ΔΔCT) comparative method. 17 The results were standardized to the content in the endogenous control. The program calculates the delta CT (ΔCT) and the ΔΔCT with the formulas below:

The Kolmogorov-Smirnov one-sample test was used to study the normality of the distribution of the variables. Comparisons of the VEGF expression in the different tissues were made between the two groups of patients using the Mann-Whitney U test for independent variables, and between the three types of tissues in the CVD group with the Wilcoxon test for paired variables with Bonferroni's correction. All calculations were performed using the SPSS programme version 15.0. The results were expressed as mean ± standard deviation, and a P value <0.05 in two-tailed analysis was considered statistically significant.
Results
Figure 1 shows the data for the VEGF gene expression in the different study groups obtained using the ΔΔCT method after qRT PCR reaction analysis. This method doubly normalizes quantitative results of the analysis of gene expression by the control genes (18S and ciclofilin) and the tissue was having lower expression of VEGF (resulting skin with telangiectasia from CVD patients).
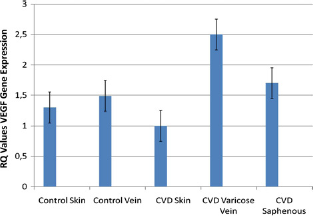
Data for relative VEGF gene expression (RQ values) in the different study tissues obtained using the ΔΔCT method after realtime PCR reaction analysis, doubly normalized by the analysis of gene expression by the control gene (18S) and the tissue having a lower expression of VEGF (resulting skin with telangiectasia from CVD patients) for statistical comparisons. VEGF, vascular endothelial growth factor; RQ, relative quantification; PCR, polymerase chain reaction; CVD, chronic venous disease
It was shown that the VEGF gene was absolutely over-expressed in skin with telangiectasia in patients with CVD compared with ciclofilin gene expression. Ciclofilin is a Ciclosporine A cytosolic receptor, which is ubiquitously expressed and constantly in the cytosol of all eukariotic cells and tissues, in which it was used as house-keeping gene positive control to demonstrate the relative quantification expression of VEGF in the assessed tissues.
An analysis of the relative quantification (RQ) values using the ΔΔCT approach was made for each tissue between the CVD group and the control group (Figure 2). The results revealed a significant difference in the skin VEGF expression between the two groups. It was lower in the CVD group than in the control group (1 versus 1.3 ± 0.1, P = 0.04). There were no significant differences between the insufficient GSV of the CVD group and the control healthy vein (1.7 ± 0.2 versus 1.5 ± 0.1, P = 0.22). In contrast, the comparison between the VV of the CVD group and the control vein showed a significant difference with a greater expression in the former (2.58 ± 0.3 versus 1.5 ± 0.1, P = 0.03).

Comparison of the relative quantification (RQ) values of the VEGF gene expression for each tissue between the CVD group and the control group. *P significant. VEGF, vascular endothelial growth factor; CVD, chronic venous disease
Comparison of the RQ values of the VEGF expression between the three different tissue types in the CVD group revealed significant differences between the skin and GSV (1 versus 1.7 ± 0.2, P = 0.02) and between the skin and the VV (1 versus 2.5 ± 0.3, P = 0.004), and also between the VV and the saphenous vein (2.58 ± 0.3 versus 1.7 ± 0.2, P = 0.02).
Discussion
Although the onset mechanism of CVD is yet to be clarified, a series of events such as the presence of dilated veins and capillaries, proliferation of dermal capillaries, 6 increased microvascular permeability. 18 and the activation of inflammatory mechanisms3,4 have all been demonstrated. These processes begin to act prior to venous hyperpressure and leukocyte trapping. 19
VEGF plays a role in all these processes by promoting vasodilation through increased NO production and increasing capillary permeability, promoting endothelial cell proliferation and inducing the expression of adhesion molecules. 9
There has been demonstrated an increase in serum VEGF levels and in trophic skin alterations inpatients with CVD, both of which enhance with the clinical grade of the disease.11,12 Howlader et al., 12 found a trend to increased serum VEGF levels among patients with healed ulcers (C5 grade CEAP). This may reflect the fact that VEGF is induced in patients with CVD to repair tissue damage caused by the disease. Otherwise, the present study showed that VV tissue over-expresses the VEGF gene compared with skin and GSV in patients with CVD. These data were obtained from C2 grade CEAP patients; thus, consistently, we could not establish an association between VEGF tissue expression and different CEAP grade classification.
Moreover, immunohistochemical techniques have also revealed an increase in the amount of VEGF in the skin of patients with primary VVs. 10 Nevertheless, this does not really clarify where this VEGF is produced.
Oppositely, our results showed a significant difference in the VEGF expression in the ‘diseased’ skin of CVD patients compared with the healthy skin in the control group, there being a lower expression in the CVD group. This could be explained by a down-regulation of the epidermal transcription of VEGF due to the saturation of epidermal receptors by VEGF produced in the VVs. 20
Comparison of the GSV of CVD patients with the control vein revealed that VEGF transcription tends to be greater in the CVD group, although the difference was not significant. These results do not agree with those of the Hollingsworth group, who found elevated VEGF transcription in insufficient saphenous veins compared with control veins, although they did not show differences in insufficient GSV with ostial competence. 16 However, our study did find a significant difference in the VEGF expression for VVs in the CVD group being higher in comparison with control veins.
When the VEGF transcription between the three types of tissues were compared (insufficient saphenous vein, VV and skin with telangiectasias), the CVD group showed significant differences between the skin and the saphenous vein, and between the skin and the VV. There was a difference towards greater VEGF gene expression in the VV than in the insufficient saphenous vein.
These findings, along with the non-existence of differences between the saphenous vein of the CVD group and the control vein, but significant differences between the VV and the control vein, mainly indicate that the origin of the increase in VEGF is localized in the wall of the VV (either in the endothelium or the smooth muscle cells of the medial wall), which could already be altered in early stages of the VV disease even without saphenous insufficiency, which will require the valvular destruction of this.
In our hypothesis, this VEGF would be produced in the venular plexus and the ‘diseased’ veins, which eventually become VVs in response to stimuli such as hypoxia and hyperpressure, or by altered base regulation of the disease, and it would be released into the dermis where it would perform its action by bonding to epidermal epithelial cell receptors.
The pathophysiology of primary CVD is complex. A causative mechanism is yet to be elucidated. Current evidence suggests that the disease starts as the result of a mechanical problem such as descending valvular incompetence 21 or because of the presence of endothelial dysfunction. 22 Nevertheless, our study shows that the origin of the VEGF over-expression in CVD is the VV itself and not the epidermis or the insufficient GSV, thus moving the whole causal process of the disease to the venous tissue.
Our data support the hypothesis of a potential genetic cause involved in the origin of CVD and show endothelial or smooth muscle cells to be clear candidates for holding the early or initial processes.
In our hypothesis, the basis for CVD might be seen initially in the loss of maintenance or regulation of VV homeostasis.
This may explain why CVD occurs in many patients where the SFJ is competent, so the importance of the failure of the SFJ valve as an initiating mechanism remains to be clarified.
The important implication of VEGF in the etiopathogenesis of the disease makes it a target for new therapeutic strategies. In fact, a previous study has shown that micronized purified flavonoid fraction, a drug widely used in all stages of symptomatic CVD, and with effects on the improvement of venous tone, capillary permeability and an anti-inflammatory effect, reduces plasma VEGF levels in CVD patients with skin involvement. 23
The field of antiangiogenic therapies could be a line of research for the future treatment of the causes of primary varicose disease. VEGF receptor inhibitors, including antireceptor-specific antibodies and other molecules, as well as VEGF-A neutralizing antibodies24,25 could be alternatives in the treatment strategies approach.
In conclusion, our results show that VV tissue over-expresses the VEGF gene, which may justify the source of the increased VEGF levels in skin and serum in patients with CVD demonstrated in previous studies, focusing on the casual process of the disease to the venous tissue.