
Abstract
Introduction
The ESCHAR trial showed that superficial venous surgery and compression in chronic venous ulceration achieved a 24-week healing rate of 65% and 12-month recurrence rate of 12%. Foam sclerotherapy treatment is an alternative to surgery. The aim of this study is to assess the effect of foam sclerotherapy on ulcer healing and recurrence in chronic venous leg ulcers.
Methods
Chronic venous leg ulcers (CEAP [clinical, aetiological, anatomical and pathological elements] 5 and CEAP 6) with superficial venous reflux were treated between March 2006 and June 2011 with ultrasound-guided foam sclerotherapy and compression. Venous duplex was performed on all legs before and after treatment. Twenty-four-week ulcer healing and one- and four-year ulcer recurrence rates were calculated using Kaplan–Meier survival analysis.
Results
Two hundred legs (186 patients) with chronic venous ulcers (CEAP 5: n = 163 and CEAP 6: n = 37) were treated with foam sclerotherapy. Complete occlusion was achieved in 185/200 (92.5%) limbs, short segment occlusion in 14/200 (7%) limbs and one leg segment failed to occlude. One patient suffered an asymptomatic non-occlusive deep vein thrombosis (DVT) diagnosed on duplex scan at one week and one presented with an occlusive DVT three weeks following a normal scan at one week. One patient developed an asymptomatic occlusive DVT at two weeks following a non-occlusive DVT diagnosed on initial one-week scan. Eighteen patients were lost to follow-up (3 moved away and 15 died of unrelated causes). The 24-week healing rate was 71.1% and one- and four-year recurrence rates were 4.7% and 28.1%, respectively.
Conclusion
Foam sclerotherapy is effective in abolition of superficial venous reflux and may contribute to similar ulcer healing and long-term recurrence rates to superficial venous surgery. Foam sclerotherapy is an attractive alternative to surgery in this group of patients.
Introduction
If left untreated, persistent venous hypertension as a result of superficial venous reflux may lead to venous leg ulceration. 1 This condition can affect any age group but it is particularly common in the elderly population, causing considerable morbidity, pain and distress. 2 Subsequent treatment places a significant economic burden on the National Health Service (NHS). 3
The ESCHAR trial published in 2003 by Barwell et al. 4 showed that superficial venous surgery led to significant reduction in venous ulcer recurrence rates at one year (12% in the surgery plus compression group against 28% in the compression alone group). The long-term follow-up of this work reported by Gohel et al. 5 confirmed that at four-year follow-up, the ulcer recurrence rate was reduced from 56% for the compression group alone to 31% in the surgery plus compression group. However, surgery may not be an attractive treatment option for all patients suffering from venous leg ulceration, with the ESCHAR trial reporting that 41% of patients eligible for superficial venous surgery refused surgery.
With the global revolution over the last decade in endovascular techniques of varicose vein management, 6 it would be logical to consider their role in the treatment of superficial reflux in limbs with chronic leg ulceration. Ultrasound-guided foam sclerotherapy (UGFS) has been used in the treatment of varicose veins in the last decade with considerable success. 7 Recently, its efficacy in the management of recently healed or open venous leg ulcers (CEAP [clinical, aetiological, anatomical and pathological elements] classification 5 and 6) has been a matter of discussion with ulcer healing and early recurrence rates following UGFS being shown to be comparable to superficial venous surgery.8–11
The aim of this study was to determine the safety and efficacy of UGFS on ulcer healing and long-term recurrence in legs with open and recently healed venous ulceration.
Methods
Patients and setting
The target population consisted of patients presenting to a specialist leg ulcer service with venous leg ulceration between March 2006 and June 2011. Patients included had recently healed (i.e. within 6 months) leg ulceration or open leg ulceration of more than four weeks’ duration; superficial venous reflux confirmed on venous duplex scan and an ankle brachial pressure index greater than 0.85. Patients were assessed in specialist nurse-led assessment clinics for suitability for UGFS following colour venous duplex imaging, and venous reflux was identified as purely superficial, mixed superficial plus segmental deep and mixed superficial plus total deep reflux. Patients with total deep reflux were not offered treatment as this group of patients failed to show any benefit from abolition of superficial venous reflux in the ESCHAR trial.4,5
Ultrasound-guided foam sclerotherapy
UGFS was performed in an outpatient setting using local or no anaesthetic. Immediately prior to the treatment the refluxing saphenous trunk or varicosities were identified on duplex, patients were then placed in a reverse Trendelenburg position for cannulation with 18–22 g cannula for truncal veins and 18 g butterfly for superficial varicosities placed where necessary under direct ultrasound guidance. Sclerosant foam was prepared by mixing 3% sodium tetradecyl sulphate (Fibrovein, STD Pharmaceuticals Ltd, Hereford, UK) and air (1:4) by using a 5 and 2 mL syringe connected by a three-way tap as described by Tessari. 12 Once cannulation was established, the patients were placed in the Trendelenburg position and foam was injected under duplex guidance into the great saphenous vein (GSV) aiming to reach within 2 cm of the saphenofemoral junction (SFJ) or into the short saphenous vein (SSV) to within 2 cm of the saphenopopliteal junction (SPJ) or directly into the refluxing varicosity. On completion of the injection, the patients were asked to dorsi and plantar-flex their ankle for a short period to help clear any foam that may have entered the deep venous system. Postprocedure: patients with active leg ulceration were placed in multilayer below-knee compression bandaging with extension of the Coban compression layer above the knee (Profore, Smith & Nephew, Hull, UK) and a full-length class II elastic stocking (Duomed, Medi, Hereford, UK) for two weeks being changed at one week; this was converted to a below-knee multilayer compression bandage at two weeks and a below-knee class II elastic stocking on healing. In patients with healed ulceration, a Coban compression bandage and a full-length class II elastic stocking were applied for two days, a full-length stocking alone for two weeks and thereafter a below-knee compression class II stocking. Immediately following the procedure, patients were asked to take a 15 minute walk if their mobility allowed.
Follow-up duplex imaging
Patients underwent colour duplex venous imaging (Sonos 2000™; Hewlett Packard, Palo Alto, CA, USA) one week postsclerotherapy to assess early treatment efficacy. This was performed by an independent specialist vascular scientist. Superficial venous segments (i.e. SFJ, above- and below-knee long saphenous vein, thigh perforator veins, SPJ, SSV and calf perforating veins) and deep venous segments (i.e. common and superficial femoral vein, above- and below-knee popliteal vein) were routinely assessed. Complete occlusion of the treated superficial veins was defined as 85% or more closure of the treated saphenous trunk or tributary with abolition of reflux. 13 Anything less than that was termed ‘short segment occlusion’. Incomplete occlusion was defined as a persistently patent vein lumen postsclerotherapy. A detailed assessment of the deep venous segments was performed to assess the degree of thrombosis; this was defined as endovenous foam-induced thrombosis (EFIT). Using a modification of the endovenous heat-induced thrombosis (EHIT) classification described previously following endothermal ablation, 14 EFIT in this study was classified as:
Type 1: thrombus lining the lumen of the deep vein <25%;
Type 2: thrombus extending into the lumen of the deep vein 25–50%;
Type 3: thrombus extending into the lumen of the deep vein 50–99%;
Type 4: complete occlusion of the deep vein.
Post-treatment assessment of the ulcerated limb
Patients with active ulceration were reviewed in a specialist nurse-led leg ulcer clinic at least once a month until the ulcer was healed and at one, three, six and 12 months thereafter. After the first 12-month follow-up, patients were seen annually in a well leg clinic. Data for ulcer healing and recurrence were collected in a prospectively maintained database.
Statistical analysis
The results were analysed in consultation with a medical statistician using the Statistical Package for Social Sciences (SPSS for Windows, version 17.0, Chicago, IL, USA). Twenty-four-week ulcer healing rates were measured for active ulcers from treatment to ulcer healing using Kaplan–Meier survival analysis. Similarly, survival analysis was used to calculate one- and four-year ulcer recurrence for healed ulcers from the time of treatment to recurrence and for active ulcers from the healing date.
Results
Patient demographics and clinical characteristics for 200 legs
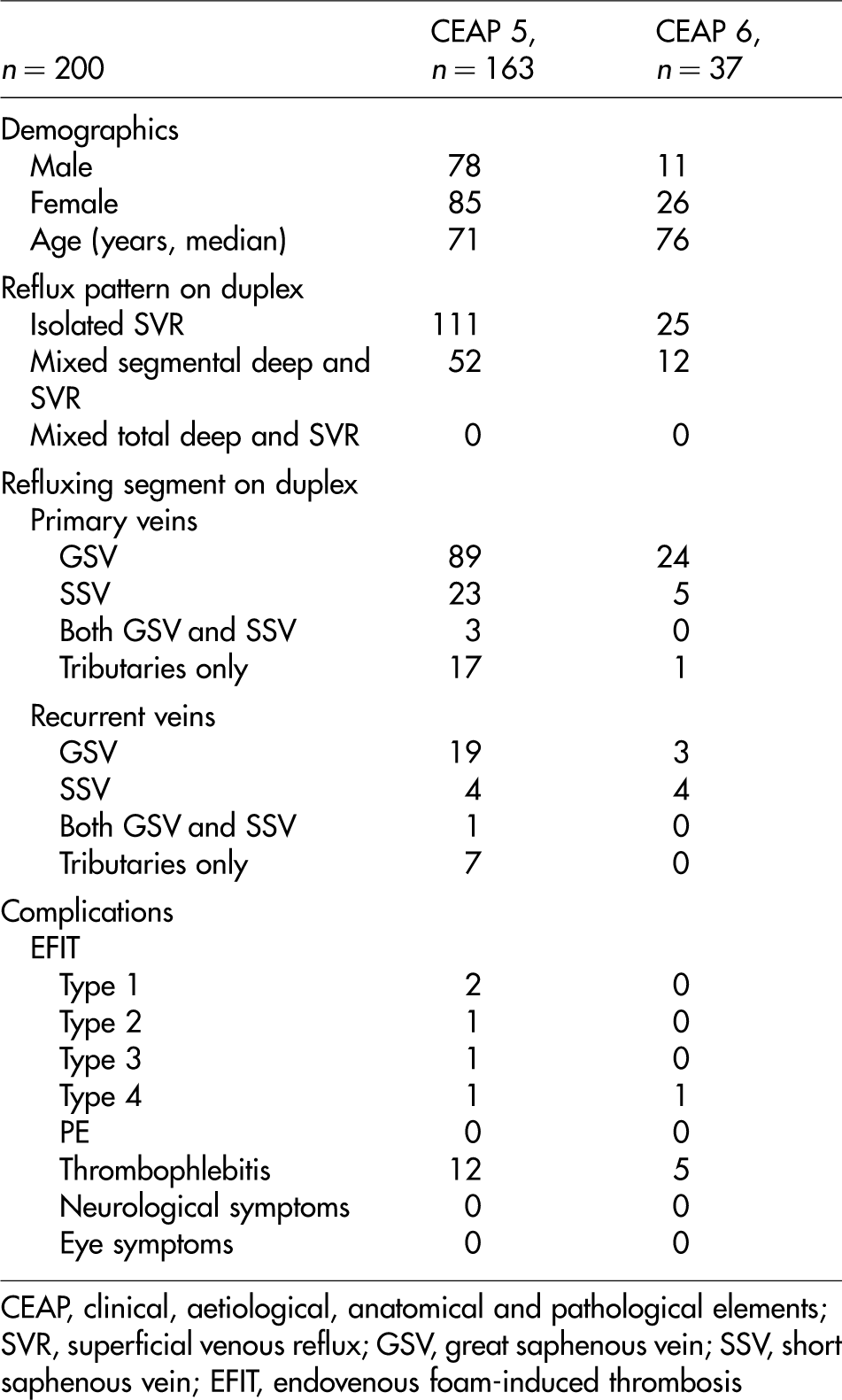
CEAP, clinical, aetiological, anatomical and pathological elements; SVR, superficial venous reflux; GSV, great saphenous vein; SSV, short saphenous vein; EFIT, endovenous foam-induced thrombosis
Effect of UGFS on truncal veins
GSV
Of the 135 legs treated for GSV reflux, overall complete occlusion was seen in 123 legs (91%) after a maximum of two sessions and short segment occlusion was seen in 11 legs (8%). In one leg the treated GSV trunk remained patent after one session with the patient refusing further treatment.
SSV
Complete occlusion was seen in 35/36 (97%) legs treated for SSV reflux after one session of treatment and short segment occlusion was seen in one leg.
GSV and SSV
Four patients had treatment for SSV reflux following initial successful treatment for GSV reflux. All four SSV trunks had complete occlusion after one session.
Tributaries only
Of the 25 legs treated for median calf, anterior thigh, medial and lateral thigh tributaries only in an otherwise normal or previously operated GSV and SSV trunks, 23 had complete occlusion after one session (92%) and two had short segment occlusion.
Effect of UGFS on ulcer healing
Of the 37 active ulcers at the time of treatment (size: median 1.9 cm2, interquartile range 0.9–7.3 cm2), 28 healed at 10 weeks (median, range 2–124). Five ulcers were not healed at the time of analysis (median follow-up 1 month), three patients were lost to follow-up following moving away and one died of unrelated cause. Using Kaplan–Meier survival analysis 71.1% of ulcers healed at 24 weeks and 91.2% at one year (Figure 1).
Kaplan–Meier analysis for 24-week and one-year ulcer healing rates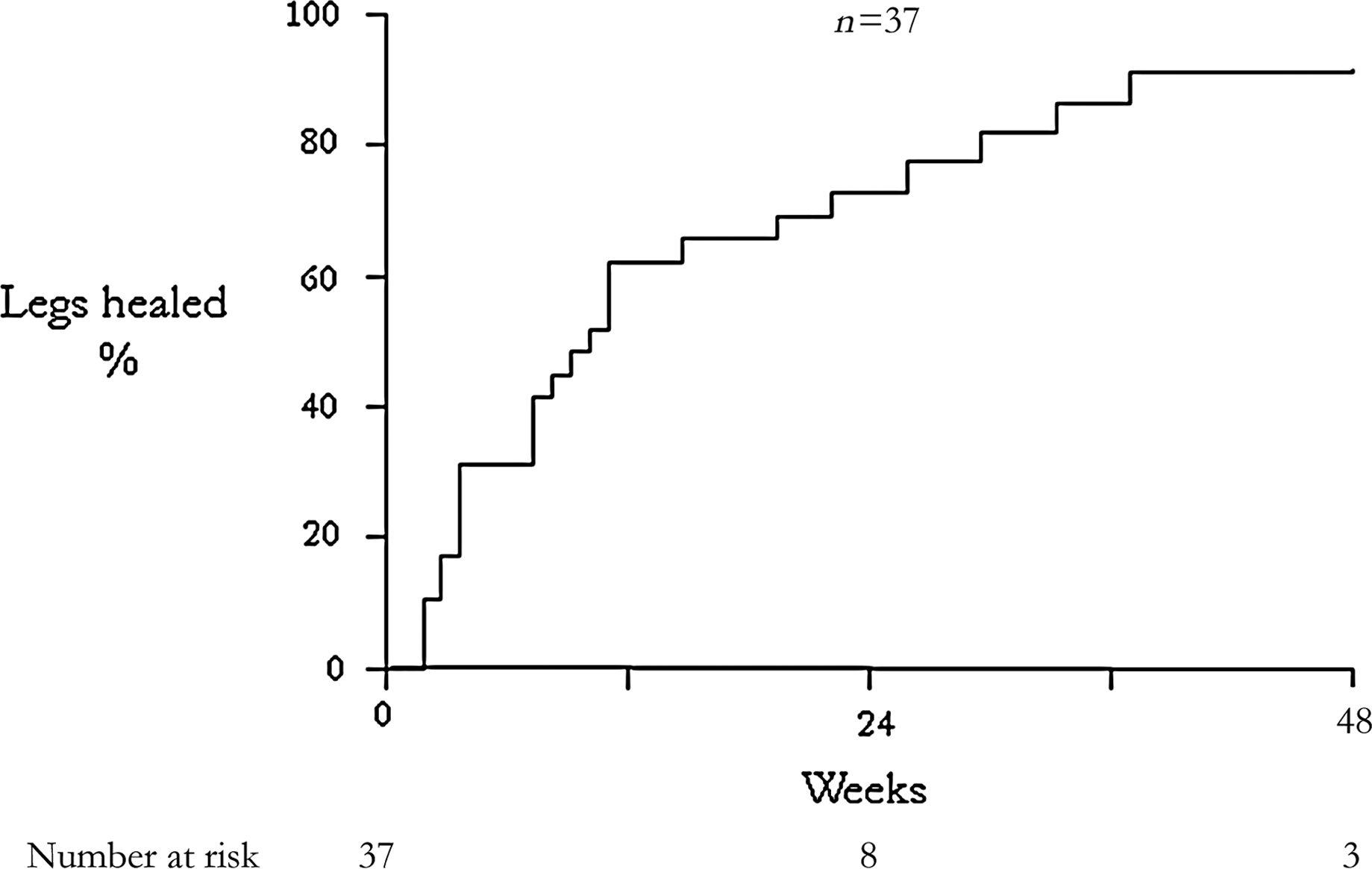
Effect of UGFS on ulcer recurrence
Ulcer recurrence was analysed on 191 legs (163 legs with recently healed ulcers and 28 ulcers that healed after treatment) with median follow-up of 26 months (range 1–60). Recurrence was seen in 28/191 (14.6%) legs at 20 months (median, range 1–50). Nine recurrent ulcers were treated for CEAP 6 (24%) and 19 for CEAP 5 disease (12%). Using Kaplan–Meier survival analysis one- and four-year recurrence rates were 4.7% and 28.1%, respectively (Figure 2).
Kaplan–Meier analysis for 12-month and four-year ulcer recurrence rates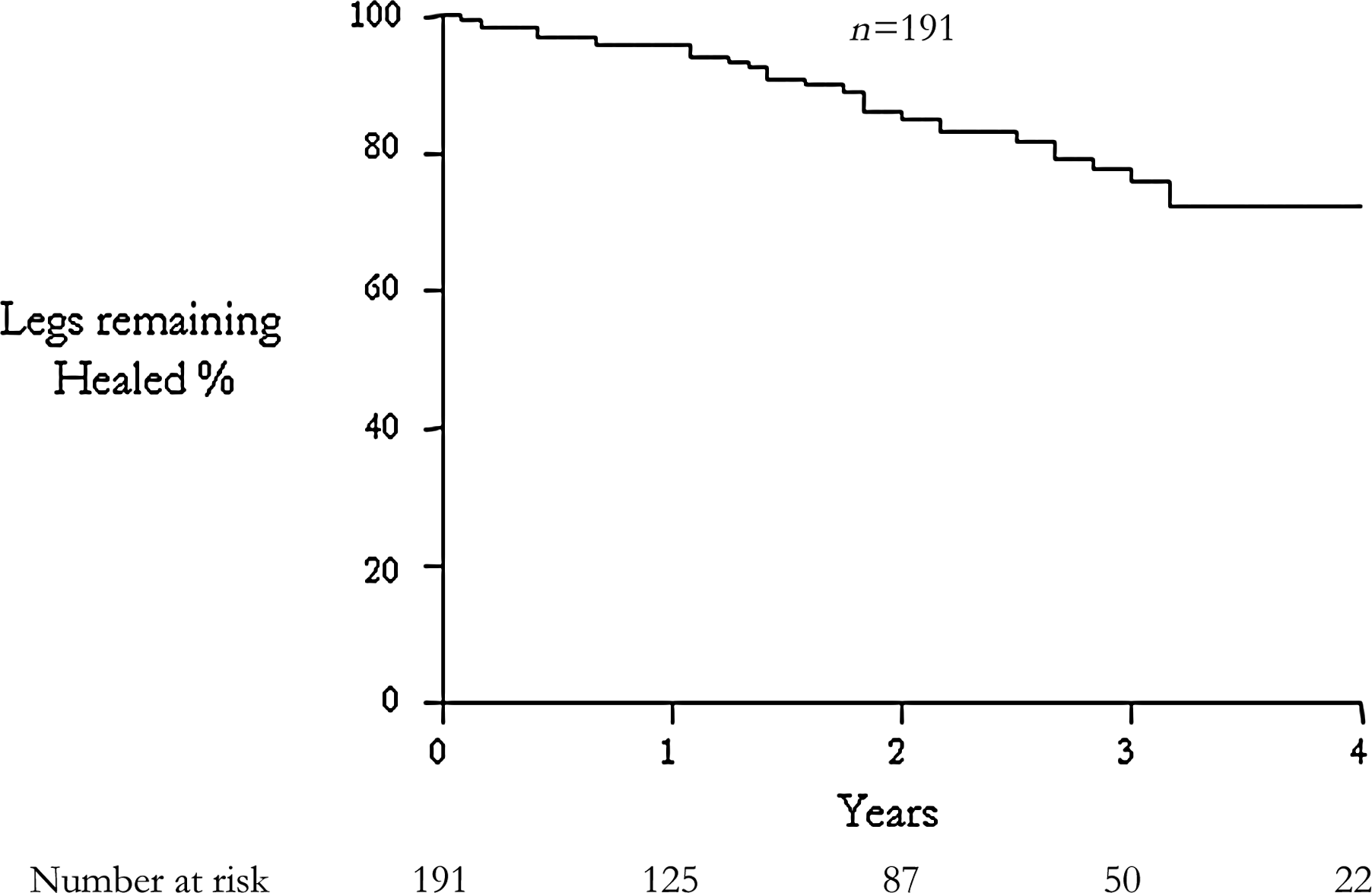
Complications
Eighteen patients were lost to follow-up, with three moving away immediately after treatment, and 15 died of unrelated causes. Following treatment, thrombophlebitis was seen in 17 patients who resolved with compression hosiery and non-steroidal anti-inflammatory medications.
At the one-week duplex scan, three asymptomatic patients had developed limited thrombus protruding into the deep vein at the junction of the main treated trunk (EFIT 1 = 2; volume of foam 4 and 10 mL and EFIT 2 = 1; volume of foam 2 mL). One received compression alone, one was treated with aspirin and compression for three months (EFIT 1) and the third was treated with warfarin and compression for two months (EFIT 2). All three legs showed full recovery with no residual reflux on subsequent duplex scans. One patient developed a non-occlusive asymptomatic deep vein thrombosis (DVT) (EFIT 3; volume of foam 5 mL) diagnosed on duplex scan at one week and was treated with warfarin and compression with complete resolution and no reflux at follow-up scan four weeks later. One patient presented with an occlusive DVT (EFIT 4; volume of foam 5 mL) at three weeks following a normal scan at one week. This patient was treated with warfarin and compression resulting in recanalization of the common femoral vein with no residual reflux. One patient developed an asymptomatic occlusive common femoral DVT (EFIT 4; volume of foam 10 mL) at two weeks following a non-occlusive DVT diagnosed on initial one-week scan. Treatment with warfarin and compression was started after the first scan resulting in partial resolution of thrombus.
None of the patients suffered pulmonary embolism and no one experienced neurological or eye symptoms.
Discussion
This study is the largest to date looking at the effect of UGFS on ulcer healing and long-term recurrence up to four years. In the last decade, minimally invasive endovenous procedures to ablate refluxing superficial veins have become more popular in the management of varicose veins and potentially have advantages over surgery in patients with venous leg ulcers. The present study demonstrated that UGFS was effective in the abolition of superficial venous reflux with favourable ulcer healing and long-term recurrence rates with a low complication rate.
The healing and recurrence rates in the present study were similar to the surgery group of the ESCHAR trial and compared well with the compression alone group of the ESCHAR trial and other published studies using compression alone.15–17 UGFS produced a 24-week ulcer healing rate of 71% when compared with 64% in the surgical arm of the ESCHAR trial. The early ulcer recurrence rate at one year for UGFS in this study was 4.7%, which appears lower than 12% at the same stage in the surgical arm of the ESCHAR trial. The long-term ulcer recurrence rate at four years was similar in both studies: 28% in this study compared with 31% in the surgical arm of the ESCHAR trial. While this present study was not conducted within the confines of a randomized controlled trial both sets of data were obtained prospectively from consecutive cases attending a similar clinic base using Kaplan–Meier analysis. Any direct comparison between these two study groups has to be considered with caution, as a number of variables are present between the two cohorts including exclusion of ulcerated legs with co-existent total deep venous reflux in this current study.
Promising results for both ulcer healing and recurrence rates following UGFS have been reported by others. In a retrospective study reported in 2004, Cabrera et al. 8 demonstrated excellent ulcer healing rates of 84% at a median follow-up of 2.7 months and favourable ulcer recurrence rates. The authors advocated a technique of abolishing virtually all the superficial venous reflux, which resulted in carrying out a mean of 3.6 treatment sessions per patient. In 2006, Bergan et al. 9 showed impressive healing rates with all 28 limbs healed following UGFS treatment. This group performed direct injection of perforating veins in four legs and in others the foam was guided in a distal direction to fill the network of venous microcirculatory vessels beneath the ulcer bed; the source of venous hypertension underneath the ulcer. This would explain improvement in venous refill time and venous function following UGFS as previously reported by Kulkarni et al. 18 In 2010, Bush 19 described a new technique of terminal interruption of the reflux source (TIRS) by injecting foam into venous branches in proximity to the ulcer bed and showed excellent results in a small cohort of 14 chronic venous ulcers.
In a larger well-designed study, Pang et al. 10 reported an 82% ulcer healing rate at a median of one month in 82 legs with active ulceration following UGFS and a 5% two-year ulcer recurrence rate in 116 legs with healed ulcers. In 2009, Darvall et al. 11 from the same unit reported their preliminary results of UGFS on 28 patients with active venous ulceration. Remarkably, 96% of the ulcers healed in three months following UGFS and only two ulcers recurred at 12 months. In their experience, patients rarely chose surgery as an option and the majority chose UGFS. Patients in our unit and other units have experienced a similar aversion to surgery, with nearly half of the patients refusing to undergo surgery. 4 A major weakness in this present study was the failure to prospectively monitor the number of patients who refused UGFS, but as this procedure was performed as an outpatient procedure, taking less than 20 minutes to perform, it is likely that only a very few declined.
Long-term data from consecutively collected prospective studies or randomized controlled trials of chronic venous leg ulcer studies are more accurately reported using Kaplan–Meier analysis and is accordingly scarce. Using this method of data analysis, the four-year recurrence rate of 28% obtained by UGFS in this study compared well with the 27% and 24% recurrence rates obtained by surgery in legs with superficial reflux and superficial/segmental deep reflux, respectively, from the ESCHAR trial. 5 One shortcoming of this present study was that the patients did not have surveillance duplex scans at one year following treatment. It is likely that some legs developed recanalization of truncal veins leading to further venous hypertension and ulceration. The development of further venous reflux in patients with leg ulceration should be anticipated and duplex surveillance as now performed in our unit to identify and counter this may lead to further reduction in ulcer recurrence by identifying legs that need further treatment.
In a recent randomized controlled trial of varicose vein treatments, Rasmussen et al. 20 showed a higher rate of recanalization of the treated saphenous trunks at one year following UGFS (16.3%) compared with radiofrequency ablation (4.8%), endovenous laser ablation (5.8%) and surgery (4.8%). While UGFS may be cheaper and repeatable, endothermal ablation appears to be a more durable method for ablating refluxing saphenous trunks. This begs the question whether some younger ulcer patients with superficial venous insufficiency who could tolerate endovenous thermal ablation under local anaesthetic would be best served by offering a hybrid treatment of thermoablation to eliminate truncal reflux and UGFS to ablate the subulcer venous plexus/terminal reflux source. This option of using a combination of endovenous treatment would be guided by availability, finance and patient suitability.
Complications in this present study were minor apart from two clinically significant DVTs. Seventeen legs showed signs of superficial thrombophlebitis, which has been frequently reported following UGFS in the past, and although unpleasant for patients does not usually present a major clinical problem.21,22 Limited extension of thrombus from the target truncal vein into the deep vein was seen in four patients diagnosed one week following sclerotherapy at the routine follow-up duplex scan with two patients having substantial DVTs, one symptomatic and one asymptomatic. Thrombus extension into the common femoral vein lumen following endovenous laser ablation and radio frequency ablation has been reported before and has been termed EHIT.14,23 This EFIT may be classified in a similar way to EHIT but is effectively a type of DVT which may require treatment. Post foam sclerotherapy scanning was performed by an independent vascular scientist in the department and not in the outpatient settings using a portable scanner. Furthermore, the scans were performed remote from the operator who had carried out the initial treatment and avoided any operator bias. We believe that this robust method of assessment provided a sensitive technique for accurate assessment that has not been described in other studies. DVT is a recognized complication and therefore early duplex scanning is recommended for detection of thrombus extension into deep veins in order to prevent progression to an occlusive DVT and potential long-term problems with the post-thrombotic syndrome.
In the current economic climate in the NHS, consideration has been given to reduce the cost of treatment in general. UGFS has been shown not only to be the least expensive, but also to be the least durable procedure in the treatment of varicose veins compared with surgery and other endovenous procedures.20,24 The favourable ulcer healing and recurrence rates described in this present study and by others makes UGFS an attractive short-term option in the management of patients with chronic venous leg ulcers and may be especially advantageous in the elderly and frail patients who find a surgical option unacceptable. However, while this procedure is relatively safe, it is not devoid of risks and perhaps each endovenous ablative technique should be considered for individual patients with an aim to reduce venous hypertension in order to improve management of chronic venous leg ulcers.
Footnotes
Acknowledgements
The authors would like to thank G Woolfrey, J Waldron, N Kenny, A Cooper and J Dyer (Gloucestershire Leg Ulcer Service); C Wakely, J Minor, L Harrison and J Howard (Vascular Scientists); and C Foy (Medical Statistician, Gloucestershire Research and Development Unit) for their contribution and support.