
Abstract
Objectives
This study aims to describe a technique for catheter-directed foam sclerotherapy (CDS) of great saphenous vein (GSV) insufficiency and report occlusion rate and patient satisfaction after a single treatment.
Methods
About 100 patients were included. The GSV was accessed at knee level. With the method of Tessari 10 mL sclerosant foam was made (2 mL 3% polidocanol and 8 mL air) and delivered along the GSV while the catheter was withdrawn. At two weeks and at one year after treatment the patients were evaluated.
Results
CDS was successfully performed in 94 of the 100 patients. After one year, 84% of the patients were satisfied. Seventy percent of the GSV were completely occluded, 14% were partly occluded and 15% were recanalized. No serious side-effects occurred.
Conclusions
CDS is safe. Patient satisfaction is very satisfying and the occlusion rate is promising after a single treatment. Repeated treatments and technical development may achieve higher occlusion rates.
Keywords
Introduction
Varicose veins and associated venous insufficiency is a common disorder, affecting 20–40% of the Western population. 1 Chronic venous insufficiency has a high impact on patients’ health-related quality of life comparable with other chronic diseases such as diabetes and cardiovascular disease. 2
Incompetence of the great saphenous vein (GSV) has traditionally been treated with saphenofemoral high ligation and stripping of the thigh GSV. However, the need for an operating theatre, complications,3,4 unsatisfactory recurrence rate5,6 as well as poor cosmetic outcome after surgery have led to the development of minimally invasive techniques during the last decade. These modern endovascular techniques challenge surgery as the gold standard for treatment of venous insufficiency.7,8
Many studies have described ultrasound-guided foam sclerotherapy (UGFS), which is attractive due to its safety profile, simplicity and cost-effectiveness.9–11 The heterogeneity between the studies is substantial, a variation of UGFS technique is used and many report results after repeated UGFS, which limits comparisons.
This is an observational study of the first 100 GSVs treated with a catheter-directed foam sclerosation technique (CDS). The aim of the study was to present the results of occlusion rate and patient satisfaction at two weeks and at one year after a single treatment.
Materials and methods
Patients
All patients with varicose veins referred to the Surgical Department of Halmstad, Sweden, were clinically evaluated by a vascular surgeon and an ultrasound (US) examination was performed by a vascular nurse trained in sonography. The US is performed in a 60° upright position to assess the diameter and reflux of the great saphenous vein at knee level and at the terminal valve at the saphenofemoral junction (SFJ). The examination includes the small saphenous vein and the deep venous system with the femoral and popliteal vein. Veins with duration of reflux ≥0.5 seconds were classified as insufficient.
Between November 2007 and October 2008, 100 consecutive symptomatic patients with verified axial reflux in the GSV were offered CDS. All patients (n = 100) accepted and informed consent was obtained. Exclusion criteria were allergy to polidocanol, a very tortuous vein (which could make the catheters impossible to advance) or a GSV diameter exceeding 10 mm at the terminal valve. Anticoagulants, history of thrombosis or recurrent varicose veins were not contraindicated. In case of bilateral insufficiency, the GSVs were treated separately. The study was approved by the Ethical Committee of the University of Lund, Sweden.
Technique
The treatment was performed in the outpatient clinic by a team consisting of two vascular surgeons and two nurses. The patient was placed on the examination table in a slightly upright position to distend the vein. An US machine (LOGIQ e, General Electric, Jiangsu, China) with a 10-MHz linear transducer was used to identify the vein, preferably immediately above the knee. The skin was infiltrated with local anaesthesia (1 mL of Mepivakain/Carbocain® 1%, AstraZeneca, Södertälje, Sweden), and the leg antisepticized and draped.
The vein was accessed by a micropuncture introducer set (MPIS; COOK, Bloomington, IN, USA) and a 0.35 Fr guidewire (Fixed Core Wire Guide Straight; COOK) was advanced proximally under US surveillance and positioned at the SFJ. A catheter (Beacon Tip Royal Flush Plus high-flow catheter; COOK) was introduced over the guidewire and positioned approximately 2 cm distal to the SFJ and the guidewire was removed. The table was slightly tilted to elevate the leg to empty the GSV. Saline was injected to visualize the tip of the catheter and confirm a position distally to the SFJ. Using a modified method of Tessari, 10 mL sclerosing foam (SF) was made by mixing 2 mL chilled 3% polidocanol (Aethoxysklerol®; Inverdia, Wiesbaden, Germany) and 8 mL air using two syringes (10 mL Becton-Dickinson, Canaan, NH, USA) and a three-way connector. 12 The GSV was compressed with the US probe proximal to the catheter, to inhibit inflow from the GSV to the common femoral vein. The foam was then delivered along the GSV while the catheter was steadily withdrawn. Approximately 9.2 mL of foam was delivered since 0.8 mL was left within the catheter. The SFJ and site of puncture was compressed for five minutes and the thigh massaged to fill superficial varicosites with foam. No additional local injection of foam was given.
Immediately after the procedure the patient was mobilized. All patients wore two-layer short stretch compression bandages (Coban2, 3 M, Neuss, Germany) for one to five days after treatment. The bandages were self-adhesive and remained until removed by the patients.
Follow-up
Evaluation with US was performed at two weeks and at one year after treatment. All patients were seen and re-examined by the same nurses who made the first US. The GSV was examined from knee to SFJ and classified as recanalized, occluded or partly occluded. If a segment of the vein of more than 2 cm was circulated it was classified as partly occluded. The femoral vein was examined to exclude thrombosis (deep vein thrombosis, DVT) or deep venous insufficiency. At the two-week follow-up, the patients were asked for complications and how they experienced symptoms compared with before treatment. At the one-year follow-up, the patients were registered as satisfied or not.
Results
Median age was 52.5 years (range 18–92), 28 men and 72 women. All patients had visible varicose veins. CEAP (clinical, aetiological, anatomical and pathological elements) classifications were C2 (n = 11), C3 (n = 58), C4 (n = 19), C5 (n = 8) and C6 (n = 4). No patient had insufficiency in the deep venous system or the small saphenous vein. Twenty-three had recurrent varicose veins.
Foam delivery along the GSV was technically successful in 94 of the 100 patients. Puncture of the GSV failed in four cases due to vascular spasm and in two patients the guidewire could not be advanced to the SFJ.
In 87 patients the GSV was punctured just above the knee, in one patient below the knee and in three at the ankle. In three patients, access to GSV was achieved by an antegrade puncture in the groin. Site of catheterization was altered after initial attempt at knee level failed due to vascular spasm. The median time for the procedure was 22 (8–90) minutes. The complete treatment exceeded 30 minutes in 20 patients, but only in two patients following the 50th patient.
At the US control two weeks after treatment, the GSV was completely occluded in 92 of the 94 successfully treated patients. In the remaining two patients the GSV was partly occluded. The patients’ experience of the treatment was registered as: ‘great improvement’ (n = 45), ‘improvement’ (n = 41), ‘no difference’ (n = 7) and ‘worse’ (n = 1).
GSV appearance at ultrasound in relation to patients’ satisfaction at follow-up

GSV, great saphenous vein; US, ultrasound
Three patients were not available for US evaluation at one year
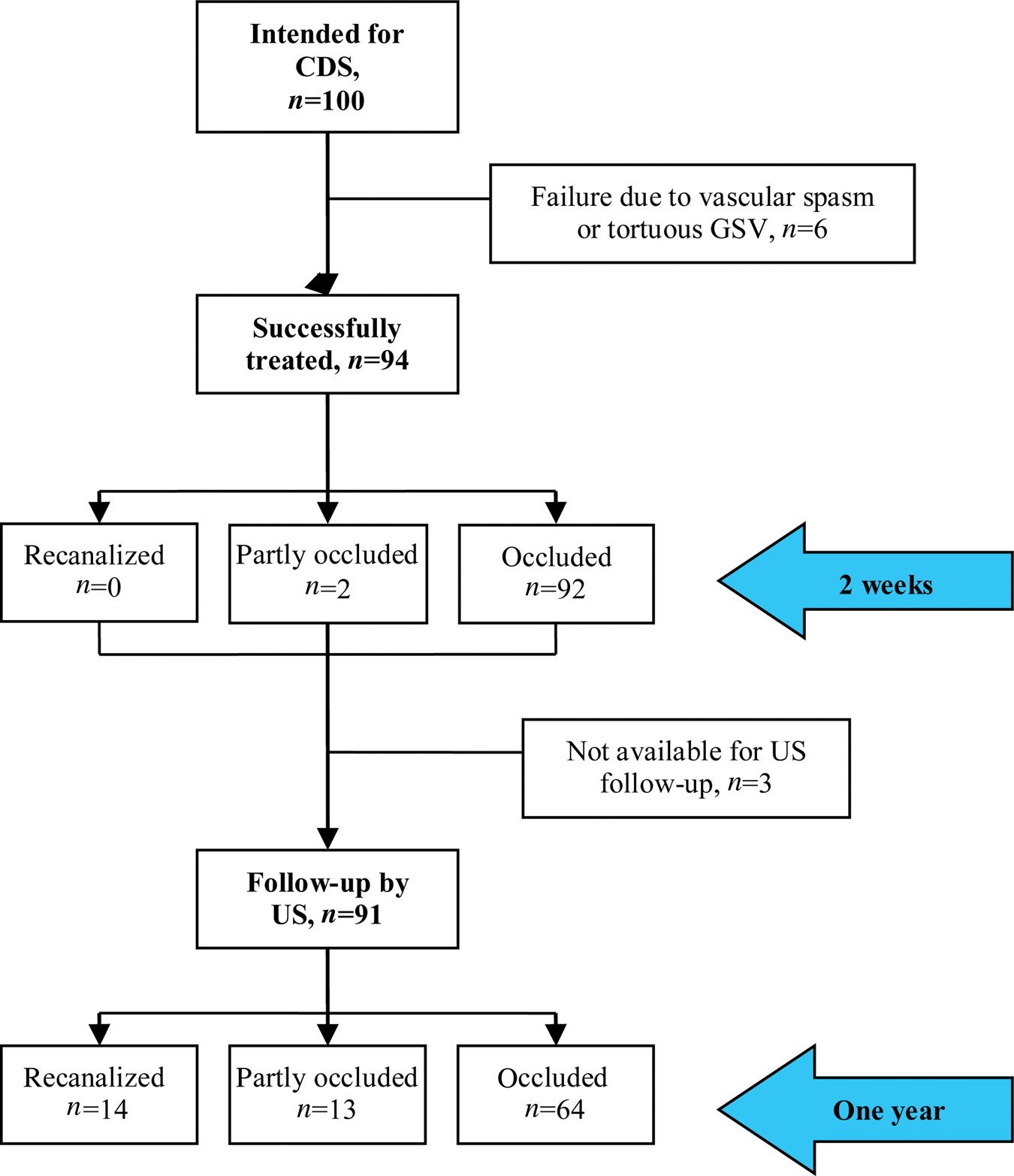
Study flow diagram
All four patients with venous ulcers were healed and satisfied.
No major complications occurred such as visual disturbance, pulmonary embolism, DVT or infection. Two patients were diagnosed with superficial thrombophlebitis. About 28% (26 patients) used prescription-free analgesia during the first week. No patient had sick leave. At the one-year follow-up 26 patients had pigmentations to some extent, with six of them displeased with the cosmetic result, but only one patient regretted the treatment.
Discussion
In this study the results of catheter-directed foam sclerotheraphy (CDS), a simplified technique for sclerosing of the GSV, is presented.
UGFS has become a well-recognized treatment of venous insufficiency since first described in the 1990s. 13 The method is attractive due to its safety profile, simplicity and cost-effectiveness.9–11
The technique has been modified over the years, since foam injection techniques and foam preparation have been shown to influence outcome.14–17 Many studies of foam sclerosation have been published but the techniques vary substantially, which limits comparisons.
UGFS has reported lower occlusion rates compared with radiofrequency ablation and endovenous laser ablation.9,18 The technique widely used to deposit foam in the GSV is by direct cannulation and injection of foam at different sites.
The foam is then distributed along the GSV by the blood flow, massaged with the US probe or by altering the position of the leg. With this procedure, the distribution of foam is affected by vasospasm and dilution with blood and may therefore be less predictable. CDS delivers the foam during a short period of time directly to the intended site, along the length of the GSV, with less impact from surrounding factors. The catheter induces a vasospasm which might further enhance drug interaction with the vein wall. This technique is simple and has shown very good short-term results suggesting that CDS may enhance occlusion rates.15,19,20
In this study, foam delivery was technically successful in 94%, which suggests that many patients with axial reflux in the GSV are suitable for CDS. Patient satisfaction of 91% (86 of the 94 patients reported ‘great improvement’ and ‘improvement’ of symptoms) at two-week follow-up indicates that CDS is well tolerated by the patients.
The complete occlusion rate was 70% at one year but 84% of the patients were satisfied with the treatment. A possible explanation could be that patients with an open or partly occluded GSV experience relief of symptoms due to a reduction of the axial reflux. The five satisfied patients with an open GSV indicated an experienced improvement of symptoms despite recanalization. Reflux and diameters of the recanalized GSVs were not measured to support this theory but it has been shown by Chapman-Smith et al. 21 in a prospective five-year study of UGFS.
A meta-analysis of 69 UGFS studies has reported an occlusion rate of 87% (60.0–98.2%). 10 The heterogeneity between the studies is substantial as many report results after repeated UGFS. The lower occlusion rate of 70% in this study reflects the outcome after a single CDS session and exclusively patients with GSV insufficiency. Additional CDS after one year have been successfully performed in 10 patients, suggesting that the technique is repeatable. Myers et al. 17 reported higher occlusion rates after a second UGFS, which indicates a possible better outcome with repeated CDS.
In this study air foam of cold polidocanol was used. Chilled polidocanol has been described in a study by Kölbel et al. 20 and in our experience foam prepared with cold polidocanol is more sustainable than a non-chilled solution, but there is no evidence for any influence on the outcome. Foam sclerosant with air or with carbon dioxide (CO2) are equally effective but CO2 foam has shown less systemic adverse effects, though clinically relevant side-effects are very rare.14,16,22 In this study, air foam was used and no severe side-effects have been observed, and no reported visual disturbances. Despite a limited sterility with this technique of CDS, no infections occurred.
The median time for CDS was 22 minutes (8–90). The range mainly reflects the learning curve. The complete treatment lasted for more than 30 minutes in 20 patients, but in just two patients after the 50th session. Time for the complete procedure after initial training was approximately 20 minutes. The very first patients were included in this presentation to support the opinion that CDS is a simple procedure to learn. After the initial cannulation, which is the most difficult part, the procedure is straightforward. The results presented here may be biased by the first cases and the occlusion rates after one year have the potential to increase by experience. Occlusion rates can most likely be improved by repeated CDS. Efforts in increasing foam contact with the vessel wall by emptying the vein before delivery and the use of higher volumes of foam in large veins may also improve the results. However, the risk of complications might increase with higher volumes of foam and not more than 10 mL per session is recommended. 11 The use of compression bandages or stockings for a longer time after CDS can possibly enhance long-term occlusion rates. Different views exist, though, on whether compression bandages should follow UGFS.11,23
The cost for the drugs and the single-use medical material was calculated to be 106 EUR. The procedure can be performed by one doctor and two nurses at an outpatient clinic. No extended analysis of the cost has been done but this indicates that CDS is far less expensive than other methods.
One shortcoming of this study is that no validated quality-of-life questionnaire was used and this study was not designed to analyse which aspects influence patient satisfaction. However, the patients reported their experience to the nurses before the US examination and were therefore not influenced by the US result.
Conclusion
It can be concluded from this study that CDS is safe, cheap and easy to perform. The one-year result regarding occlusion rates after a single CDS is less than expected, but the patient satisfaction is high.
Footnotes
Conflicts of interest and funding:
None.
Acknowledgements:
A special thanks to Linda Rapp and Ulrika Johansson for registration of patient data.