
Abstract
Intra-arterial injections represent the most feared complication of sclerotherapy for varicose veins. We present a case of an inadvertent intra-arterial injection of polidocanol at the left medial calf in a 59-year-old woman with subsequent arterial occlusions of the posterior tibial artery and foot arteries. Despite several therapeutic interventions, lower-limb amputation could not be prevented. We conducted a PubMed search for articles reporting arterial complications related to sclerotherapy, in order to evaluate aetiology, clinical presentation, therapeutic management and outcome of sclerotherapy-associated intra-arterial injections during the past 50 years. Intra-arterial injection of a sclerosing solution was reported in 63 cases, mostly after injection near the ankle region or the distal medial calf. Clinical presentation was frequently characterized by immediate pain during injection and distal ischaemia with subsequent tissue loss. Despite several treatment approaches, amputation could not be prevented in 31 cases (52.5%). The pathophysiology of arterial complications related to intra-arterial injection and advisable therapeutic interventions are discussed. Inadvertent intra-arterial injection represents a limb-threatening complication of sclerotherapy. Target-oriented and prompt therapy seems inevitable in order to reduce the risk of permanent tissue loss and amputation.
Introduction
Sclerotherapy has been effectively used for decades in the management of varicose vein disease. Previous studies have proven the efficacy of the method and reported potential side-effects.1–3 Intra-arterial injections represent the most feared complication of varicose vein sclerotherapy, as an intra-arterial injection of the sclerosing solution might lead to skin damage and subsequent tissue loss in affected extremities. Ultrasound guidance has revolutionized the method, but could not prevent subsequent arterial complications. There is still no effective strategy for prevention or for treatment of critical limb ischaemia related to intra-arterial injection of the sclerosant. As prevention is still the best ‘therapeutic’ option, we want to remind of this potential complication, present one case of critical limb ischaemia related to inadvertent intra-arterial injection of a sclerotherapy foam solution and review the current literature dealing with this rare but serious complication.
Case report
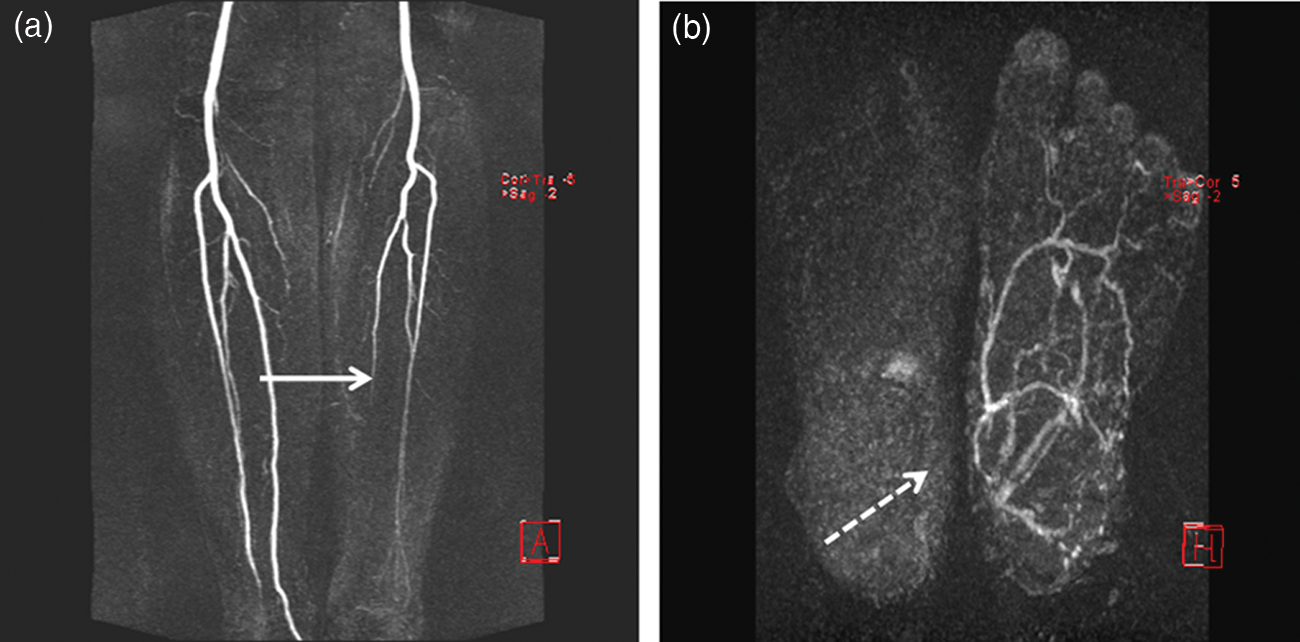
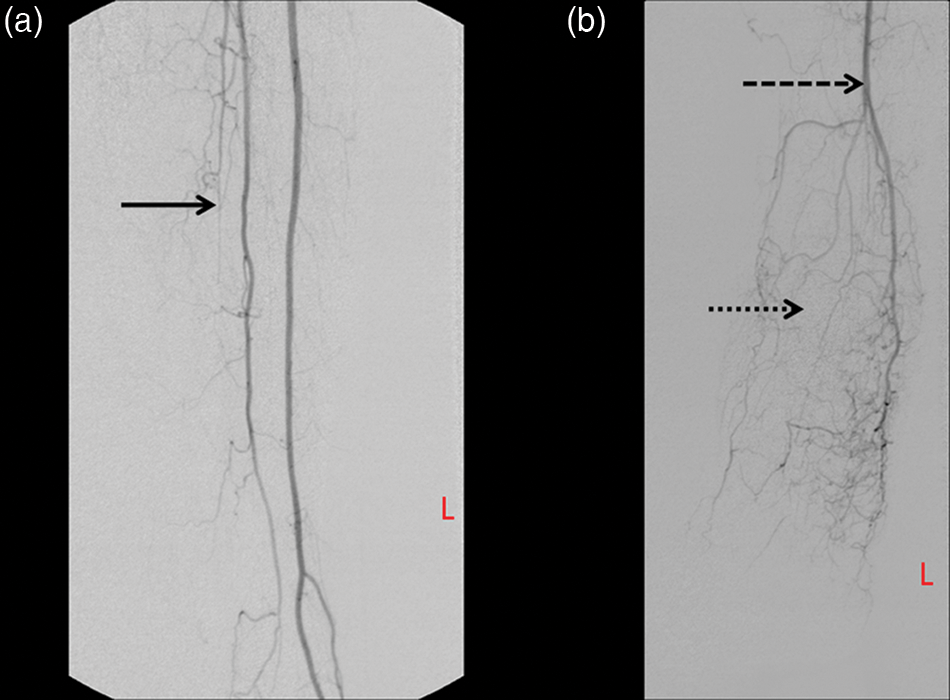
A 59-year-old female Caucasian presented at our outpatient clinic for vascular disorders because of massive pain and pallor in the left forefoot subsequent to a foam sclerotherapy procedure for varicose veins the day before. The foam sclerotherapy using 2% polidocanol (Aethoxysklerol) was performed by a resident surgeon to treat a chronic venous valvular insufficiency (CEAP [clinical, aetiological, anatomical and pathological elements] classification grade C2) of a saphenous side branch vein on the left medial calf without considering a preceding duplex evaluation of the veins. The first and second volumes, each about 1.5 mL of 2% polidocanol, were injected 7–10 cm above the medial ankle on the left side. Immediately after the second injection the patient complained about a burning pain at the site of injection; subsequently the sclerotherapy procedure was stopped and a short-stretch bandage was wrapped over the lower leg. Fifteen minutes after the last injection, the patient complained about a burning pain and numbness of the left forefoot and inability to move the toes of the affected extremity. Compression therapy was discontinued after two hours during the home visit of the resident surgeon. As symptoms persisted overnight, the patient was finally referred to the outpatient clinic of vascular diseases 14 hours after the sclerotherapy procedure. A sharply demarcated cyanotic pallor and beginnings of oedema of the foot were prominent during the first clinical examination at the outpatient clinic (Figure 1). The duplex scan of the lower limb arteries during this examination revealed an occlusion of the left posterior tibial artery. In order to evaluate the length of occlusion and collateral vessels, we performed a magnetic resonance angiography (MRA) of the lower limb arteries 19 hours after sclerotherapy. MRA confirmed occlusions of the left posterior tibial artery, the dorsalis pedis artery and the plantar arch (Figure 2). Sufficient collateral vessels or potential anastomoses for pedal bypass surgery could not be confirmed by MRA or by digital subtraction angiography (DSA) of the left leg (Figure 3). The results of these imaging procedures did not allow endovascular revascularization or a pedal bypass surgery to treat the critical limb ischaemia in this case. We decided on an intra-arterial application of Alprostadil (10 μg daily) and activated partial thromboplastin time-adjusted continuous intravenous infusion of unfractionated heparin (UFH) for seven days. Hence steal mechanisms of prostanoid therapy led to a further reduction of left forefoot perfusion; Alprostadil therapy had to be withdrawn after three days. In order to induce a potential collateralization, we treated the patient for 10 weeks with a low-molecular-weight heparin in therapeutic dosage (dalteparin, 12,500 units daily subcutaneously), 100 mg of acetylic salicylic acid (ASA) orally, fluid substitution and analgesics according to the World Health Organisation (WHO) recommendations. The patient subsequently developed gangrene in the left forefoot and distal plantar foot; when compared with the initial clinical presentation, the demarcation line descended during the 10-week therapy distal towards the metacarpo-phalangeal joints (Figure 4). Consecutively, an amputation of the left forefoot and necrectomy of the distal plantar foot and subsequent soft tissue reconstruction with a latissimus dorsi flap was inevitable. Because of persisting plantar pain already at rest and progressive calcaneal osteomyelitis, the patient unfortunately underwent lower limb amputation two months later.
Clinical picture on the day of admission: cyanotic pallor of the left forefoot with a sharp demarcation line Magnetic resonance angiography of the lower legs (a) and feet (b). Full line arrow marks the beginning of the posterior tibial artery-occlusion; the broken line arrow shows the absence of the left plantar arch Digital subtraction angiography of the left lower leg arteries (a) and foot arteries (b). Full line arrow marks the proximal end of posterior tibial artery occlusion. Large broken arrow marks the left fibular artery which is the solitary main artery on the left foot. The small broken arrow marks the site of the occluded dorsal pedis artery. Sparse arterial collateralization to the medial forefoot and toes Clinical picture of the left forefoot after 10 weeks. Sharply demarcated gangrene of all toes, the demarcation line shifted within the 10-week therapy distal towards the metacarpo-phalangeal joints

Methods
A PubMed search of articles was conducted using the keywords ‘sclerotherapy’ and ‘artery’, ‘arterial’ or ‘intra-arterial’, or ‘complication’, excluding reports of esophageal varicoses. All abstracts published between 1 January 1961 and 1 November 2011 were evaluated for reports of intra-arterial injections subsequent to sclerotherapy of varicose veins. The literature research was restricted to English, French and German languages. We retrieved a full printed manuscript from the library of the Medical University of Graz of all abstracts with reported arterial complications, intra- or periarterial injections, as well as all manuscripts with missing abstracts and those manuscripts which were not detected by the PubMed search, but cited in one of the manuscripts retrieved. Abstracts of conference reports were excluded in this review.
Age and gender of the patients, site of injection, type and concentration of the sclerosant, onset and type of symptoms, diagnostic procedures, vessels involved, subsequent treatment and need for amputation were recorded from all reports identified. The case reported above was added to the review. Descriptive statistics were performed using the Statistical Package for Social Sciences Version 18.0.
Results
We identified 277 manuscripts fulfilling the mentioned PubMed search criteria, and of those 29 manuscripts with potential reports of complications during sclerotherapy of varicose veins were retrieved. Another 12 manuscripts not identified by PubMed search, but cited in 29 manuscripts, were included. Finally, 19 manuscripts with reports of inadvertent intra-arterial injections of a sclerosant during sclerotherapy of varicose leg veins were included in this review.4–22
Based on these 19 reports and the case report presented above, 63 cases of intra-arterial injections subsequent to sclerotherapy were analysed. Thirty-one of the 63 cases were published in French literature,4,7,9,11–13,15,16,18 five cases in German5,14 and the remaining 27 cases were retrieved from English literature.6,8,10,17,19–22 The mean age of the patients was 44.3 ± 12.9 years. Of the 32 cases with gender specification, 21 (66%) patients were women and 11 (34%) were men.
Sclerosing agent
Data regarding the sclerosant used could be retrieved in 37 cases. Sodium tetradecyl was the most frequent sclerosant, leading to arterial complication in 24 cases (64.9%). Especially, recent reports describe the usage of polidocanol in seven cases (11.1%), whereas polyiodinated iodine was used in four cases (6.3%) of published intra-arterial injections. There exist only single case reports of intra-arterial injections of hypertonic saline and Ethanolamine oleate, one case (1.6%) reported for each of these sclerosants. The more concentrated 3% solutions of sodium tetradecyl or 3% polidocanol were used in 20 (87%) and five (71%) cases of intra-arterial injections, respectively.
Site of injection
All reports included in this review commented on the site of injection leading to arterial complication. However, there is only sparse information regarding the quantity of preceding therapies and number of injections during the sclerosing session. Most arterial complications were reported after injections at the ankle region5,6,9,11,14,15,20 or the medial calf up to 10 cm above the ankle corresponding to ‘Cocketts’ perforating veins,8,16,19 with a frequency of 10 (15.9%) and 26 (41.3%) cases, respectively. Only one report describes an arterial complication after sclerotherapy near Sherman's perforating vein at the medial calf, 8 whereas intra-arterial injection during sclerotherapy at the cross-section of the small saphenous vein occured in 10 (15.9%) cases.4,7,12,17,18,20 Complications during sclerotherapy at the thigh were less frequent with eight reported cases (12.7%) after injection near the cross-section of the great saphenous vein10,12,13,17 and three reports (4.8%) of peripheral ischaemia after injection of the sclerosant at the medial thigh.10,21 Multiple injections were reported in two cases;20,21 one case describes arterial complication after sclerotherapy of an incomplete gastrocnemius vein. 20 Endovascular catheter-assisted sclerotherapy of the great saphenous vein lead to intra-arterial injection in one single case reported by Grommes. 22
Onset and signs of intra-arterial injection
In 57 cases, information about the onset of symptoms could be retrieved. Immediate pain during and directly after sclerotherapy was described in 48 reports (84.2%). In six cases (10.5%) onset of symptoms occurred within minutes, whereas a delayed onset of signs within 48 hours appeared in only three cases (5.3%) related to intra-arterial injection.
The signs can be categorized as local effects at the site of injection and secondary failures related to ischaemia of the tissue affected by impaired arterial perfusion. The pain at the site of injection appeared consistently immediately after or during the injection of the sclerosant. Several reports describe a cascade of immediate pain, which subsequently radiated distal along the arterial path. Peripheral ischaemic symptoms like discolouration of the foot, subsequent foot oedema, violent distal pain and paraesthesias were reported with a latency period up to 12 hours. Although local pain at the injection site is frequent, some reports describe solitary distal ischaemia.
Discolouration or cyanosis occurred within several hours. Ischaemia of the skin was characterized by a sharply demarcated border which presumably corresponds to the area of distribution of affected arteries. Skin discoloration was not limited to the foot; especially injections at the site of perforating veins of the medial calf and the cross-section of the lesser saphenous vein lead to local demarcated areas at the site of injection.
Neurological symptoms like numbness of the foot and dysaesthesias up to paresis of the foot accompanied distal ischaemia. These symptoms were transient in some cases, but persisted more often until demarcation of gangrene.
Affected arteries
Only 40 reports (63.5%) comment on affected arteries in cases of inadvertent intra-arterial injection during sclerotherapy.5,6,8–15,17–22 Commonly, arterial injection of the sclerosing agent leads to an occlusion of the affected artery and its branches. In 20 cases (50%) intra-arterial injection occurred at the posterior tibial artery, whereas only single case reports describe this complication at the anterior tibial artery 11 or peroneal artery. 18 Two cases report occlusions of isolated foot and toe arteries,9,21 whereas six reports (15%) comment on the injection of the sclerosing agent into the superficial femoral artery,10,12,17,21,22 mostly after injection near the cross-section of the great saphenous vein. In 10 cases, intra-arterial injection affected smaller arteries like branches of the popliteal artery, 13 the superficial external pudendal artery 17 and the median superficial sural artery. 17 Peripheral pulses were mostly absent after injection at the femoral artery and the lower leg arteries. However, despite documented arterial involvement, the pulse of the affected artery was still present in four cases.11,13,17,20
Immediate therapy
In the absence of consistent guidelines, several treatment approaches tend to establish reperfusion of occluded arteries and to ameliorate peripheral perfusion, in the hope that subsequent amputation can be prevented. In 40 cases, information regarding therapeutic management could be retrieved. Heparin use was documented in 27 (42.9%) of those cases. In 10 cases (15.9%), intra-arterial infiltration of procaine or lidocaine was considered as immediate therapy. Vasodilating agents, such as nitrates and prostanoids, were applied in 12 cases (19%) and intravenous dextrane was used in 10 cases (15.9%) of arterial complications subsequent to sclerotherapy. Although occlusions of the affected arteries occurred frequently, subsequent attempts at catheter-directed thrombolysis or mechanical thrombectomy were undertaken in just four (6.3%) and two (3.5%) cases, respectively.
Outcome
Amputation is still the most feared complication of intra-arterial injection during sclerotherapy. In 59 cases, the authors comment on the rate of amputations. Unfortunately, amputation was unavoidable in 31 (52.5%) of these cases,8–12,14,16,20–22 with a need for major amputation in 10 cases (32.3%). Minor amputations, i.e. amputations of the forefoot or toes, were performed in 21 patients (67.7%). With respect to the site of injection, amputations were not reported after injection near the cross-section of the lesser saphenous vein and, when compared with other regions, less frequent at the ankle area with three (30%) reported amputations among the 10 cases.9,11,20 Arterial complication after injection at the groin necessitated amputation in three (37.5%) of the eight cases reported,10,12 but these amputations had to be performed above the knee. In contrast to these data, intra-arterial injection at the distal medial calf, corresponding to the area of ‘Cockett's’ perforating veins, led to subsequent amputation in 19 (73.1%) of the 26 cases,8,14,16,21 with a necessary major amputation in four cases.
In 59 cases, authors commented on outcome and persistent damage. If all cases of amputations, persisting pain or persisting neuropathic and myopathic damages were combined, persisting damage can be recorded in 50 (79.4%) of those cases. The authors described a full recovery within several weeks in only nine reports.8,9,12,14,17,20 Treatment approaches did not differ between these nine cases and 50 reports of persisting damage.
Discussion
Endovenous foam sclerotherapy has proven its safety with an overall complication rate of 0.58% reported in a multicenter registry of 12,173 sessions. 3 Most complications are benign and can often be related to lack of experience of the performing specialist. More frequent side-effects are superficial thrombophlebitis or residual pigmentation.23,24 Intra-arterial injections of the sclerosing agent are seldom, but as they bear the risk of critical limb ischaemia with frequently needed amputation, they represent nearly the most feared complication of the method.
Aetiology
Intra-arterial injections occurred most frequently at the malleolar area and the site of perforating veins above the medial ankle. However, arterial complications subsequent to inadvertent intra-arterial injection are not restricted to the malleolar region; other areas predisposed are the groin and cross-section of the lesser saphenous vein. It has to be pointed out that any injected area bears the risk of intra-arterial injection. Ultrasound guidance during sclerotherapy conceivably reduces inadvertent intra-arterial injections, but cannot prevent this complication, as the reported cases of tissue necrosis subsequent to the ultrasound-guided injection showed.17,20
Most authors assume that arterial occlusions occur directly after injection of the sclerosing agent into the artery. Another explanation was first raised by de Takats 25 in 1959, who illustrated connections between arterioles and venoles at the precapillary junction. Despite intravenous injection, a crossing of the sclerosing agent towards the arteriolar precapillary system may occur through these junctions. Reviewing the presented cases of arterial complications, this theory may only be applicable to a minority of these reports, because the frequent concomitant phenomenon of tissue necrosis around the injection site and distal ischaemia of the forefoot cannot be explained by arterio-venous shunts at the precapillary junction.
Pathophysiology
Usually, in sclerotherapy of varicose veins, the therapeutic agent, or so-called sclerosant, is being injected into the lumen of the vein, aiming to create venous wall damage and subsequent occlusion. Endothelial damage is dependent on the dose and the time of contact between the agent and the intimal layer; 26 in vitro studies demonstrated death of endothelial cells 15 minutes after exposure to 0.3% polidocanol or 0.1% sodium tetradecyl sulfate (STD). Subsequent adherence and aggregation of platelet cells initiate the intrinsic coagulation pathway by activating factor XII.
In a canine and rabbit animal model, arterial injection of a sclerosing solution caused the development of an embolus. 27 This study indicated that in particular STD had little effect on the major arteries, not evoking any spasm, but STD led to sludge in smaller vessels by denaturation of blood cells with subsequent obstructed microcirculation. Secondary arterial thrombosis occurred due to stagnation of the blood flow. In 1967, Fegan discussed whether STD would lead to intimal irritation and subsequent damage of this inner layer of the arteries. In contrast to the documented endothelial damage after sclerotherapy of varicose veins, no intimal damage or irritation of the vessel wall could be observed within the first three weeks after intra-arterial injection of the sclerosing solution in the canine animal model. Of interest, the sludge of denaturized blood observed did not contain any cellular particles and no fibrin was formed. Contrary to the observations in the canine model, intra-arterial injection of sclerosing agents caused severe lesions of the arterial wall and embolization of terminal vessels with documented dispersal of cell debris into peripheral microcirculation in a rat animal model. 28
The toxicity of sclerosing agents to granulocytes and red blood cells has been proven by in vitro studies at dilutions of up to 1:1000. 29 In addition to these effects, polidocanol and STD, the most frequently used sclerosants, both exhibit procoagulant activity through stimulation of platelet lysis and release of procoagulant platelet-derived microparticles. 30 In contrast to STD, polidocanol activates the intrinsic pathway of coagulation with a proven impact on clotting factors VIII, IX, XI and XII.30,31 The impact on blood coagulation seems to be dose- and time-dependent. Furthermore, Parsi reported that the impact on the coagulation system is not limited to platelets and procoagulant clotting factors. Polidocanol and STD reduced the concentrations of anticoagulant factors protein S and protein C. 32 A combination of distinct toxic endothelial damage, cellular degradation of blood cells and activation of the blood coagulation can be presumed as the pathophysiological pathway of arterial occlusion related to sclerosing agents.
Despite occlusion of the microcirculation, proximal arterial thrombosis was a frequently observed complication, ancillary deteriorating peripheral blood inflow. Proximal thrombosis of affected arteries can be explained by a major impact of all three components of Virchow's triad. 33 In particular, this applies to the abnormalities in blood composition, the vessel wall itself and blood flow. However, the pathophysiology in developing arterial and venous thrombosis appears to be more complicated; especially the crosstalk between these components seems to determine the subsequent thrombus formation. 34 Arterial complications during sclerotherapy and the mentioned animal studies have proven broad endothelial damage, stasis related to distal occlusion of the microcirculation and finally degradation of blood components and activation of the coagulation cascade. This broad impact on all components of Virchow's triad might explain the frequent arterial thrombotic manifestation after inadvertent arterial injection of a sclerosing agent.
Arterial occlusion may lead to the development of a compartmental syndrome with neurological deficits up to paralysis, 35 caused by elevated intra-compartmental pressure. In case of persisting compartmental syndrome, leg atrophy follows muscle necrosis. Unless large arteries of the calf are occluded, peripheral arterial pulses may be still palpable and feign intact perfusion. Early and effective diagnosis remains as a clinical challenge because currently there is no established role for imaging in acute compartment syndromes. 36
Signs and outcome of intra-arterial injection
The signs of intra-arterial injections are variable. In most cases, inadvertent intra-arterial injection of the sclerosing agent leads to an immediate burning pain at the site of injection; as a consequence of peripheral ischaemia, the pain subsequently propagates distal along the corresponding tissue of the involved artery. A common sign is a sharply demarcated cyanotic pallor or erythematous colour change of the affected area. Subsequent tissue necrosis was observed around the injection site independently from the site of injection and distal, mostly localized at the forefoot. The immediate pain during injection and intense burning pain in the distribution of the artery with subsequent tissue necrosis are similar to complications of drug abuse following intra-arterial injection. 37 Similar to inadvertent injection of the sclerosing agent, vascular complications during drug abuse show a picture of diffuse tissue ischaemia and patchy muscle necrosis, which may be exacerbated by the development of a compartment syndrome. 38 Despite obvious tissue necrosis, peripheral pulses may remain palpable in both. Two other conditions are characterized by a similar pattern of necrosis and ulceration: warfarin necrosis and calciphylaxis. As reduced levels of antithrombotic clotting factors, protein C and protein S are common in all of these diseases, a key role of reduced antithrombotic factors leading to microcirculatory obstructions can be presumed.39,40
As an inevitable consequence of tissue necrosis, amputations were performed in almost every second case of inadvertent arterial injection. One-third of these applied to major amputations, performed above the ankle. The extent of necrosis with unrecoverable tissue damage and chronic pain necessitated most of the reported amputations; single cases of amputations were performed with the intent to control infection and osteomyelitis.
Therapeutic strategies
Ischaemia related to intra-arterial injection of a sclerosing solution: pathophysiology, therapy and its effectiveness

ASA, acetylic salicylic acid; i.a., intra-arterial
When intra-arterial injection is recognized by the physician, the needle should be left in position in order to aspirate blood and the remaining sclerosing solution back into the syringe. 41 Whenever possible, attempts should be made to aspirate the remaining sclerosing solution from the affected artery. The authors recommend replacing the syringe and slowly injecting 10,000 IU of the unfractionated heparin into the affected artery. Several authors argue for the consequent use of heparins, either by intra-arterial, intravenous or subcutaneous application as subsequent anticoagulation;6,8,9,12,14,15,17,20–22 despite this consensus concerning heparin therapy following intra-arterial injections of sclerosing agents, its efficacy in this situation is just as little proven as all other potentially beneficial therapies. However, heparin inhibits the coagulation cascade as one of the three components of Virchow's triad and therefore heparin presumably reduces the liability of thrombus formation. Hence platelet activation, platelet membrane damage and microparticle release further propagate thrombus formation, platelet inhibition may be recommended. Immediate intravenous application of acetylic salicylic acid, at a dosage similar to coronary events with 500 mg ASA injected, might be beneficial.
Intra-arterial infiltration with procaine (1–3%) was presumed to form a complex with sclerosing solutions and inactivate its toxicity. 42 Therefore, procaine and lidocaine were used in several cases of inadvertent intra-arterial injection of a sclerosant.4,7,8,12–15,18,20 However, in vitro studies with procaine, lignocaine and protamine did not confirm the suspected potential protective benefits of these drugs. 43 In contrast, these drugs additionally slightly increased the haemolytic activity of STD. The authors commented that the haemolytic activity of polidocanol and STD were not inhibited by procaine, lignocaine or protamine, but bovine serum albumin turned out to neutralize the haemolytic activity of these sclerosants. Hence albumin is one of the major components of blood plasma, and patient's blood might dilute and inactivate the toxicity of polidocanol and STD. They assume that 1 mL of blood would contain enough plasma to neutralize 0.2 mL of STD or 0.4 mL of polidocanol at 3% concentration.
Blood has been proven to be the most effective agent neutralizing the toxicity of sclerosants, by diluting its concentration and albumin-dependent reduction of cellular lysis. 43 The lytic activity of the sclerosants is dose- and time-dependent. Therefore, all attempts should be made in order to achieve immediate revascularization. This raises the question how to re-establish arterial perfusion, especially regarding the obstructed microcirculation. Catheter-directed aspiration is effective to treat obstructions related to arterial embolization of larger arteries, 44 but this therapy is ineffective when the obstruction is localized in the microcirculatory vascular bed. Thrombolysis was used in four cases of inadvertent arterial injection.14,20,21 In only one case complete recovery was reported, whereas amputation could not be prevented in two of these cases. As these results do not differ from the other cases not considering thrombolytic therapy, it is debatable whether catheter-directed thrombolysis can be recommended as a therapeutic regimen for inadvertent intra-arterial injection of the sclerosing agent. In cases where cellular lysis has already taken place and microcirculatory obstruction is caused by sludge of cellular degradation without fibrin, thrombolysis presumably might be ineffective. However, proximal thrombosis of the arteries has been documented and thrombolysis might improve peripheral perfusion by restoring the capacity of arteries occluded by thrombosis. Kobayashi 26 reported sclerosant-related endothelial damage within 15 minutes of contact; therefore, thrombolytic therapy should be considered especially in the very early phase after recognition of the arterial complication.
Several authors recommend the administration of intravenous dextran, a composition of long-chain carbohydrate polymers.6,8,17,19,41 In vivo studies suggested that dextran lowers blood viscosity and increases peripheral blood flow. 45 Furthermore dextran seems to inhibit clotting factor VIII, increase clot lysability and decrease platelet aggregation.46,47 Data regarding the effect of dextran on the short-term patency of grafts after bypass surgery are conflicting, especially the largest of these studies, which reported negative results regarding its efficacy. 48 The authors conclude that there may be subsets of patients who might benefit from dextran administrations; this applies to patients with veins of poor quality or those with poor outflow. If this suggestion can be applied regarding arterial complications of sclerotherapy, these patients would probably benefit from dextran administration.
Therapeutic approach to complications related to intra-arterial injection of a sclerosing solution

ASA, acetylic salicylic acid; i.a., intra-arterial; p.o., per os; i.v., intravenous
Conclusion
Although intra-arterial injection of a sclerosant might lead to critical limb ischaemia and subsequent need for amputation, this rare complication does not question the proven safety of the method. However, each physician performing sclerotherapy should be aware of this rare but serious complication. High personal experience and careful ultrasound-guided technique may reduce the risk of such events. As endothelial damage occurs within the very first minutes after injection of the sclerosant, prompt realization of the arterial complication and immediate therapy seems essential to reduce the risk for subsequent amputation.