
Abstract
Pelvic congestion syndrome (PCS) is frequent and underestimated as both symptoms and signs are not specific. Furthermore, patients consult general practitioners as well as specialist gynaecologists, urologists, vascular surgeons and phlebologists who are frequently unaware of this condition. Investigation protocol must first eliminate other diseases with similar clinical disorders and then identify which veins are responsible for PCS related to compression or reflux. Selective venography is the more informative investigation but transvaginal ultrasound examination is a valuable screening test. Outcome analyses after endovenous treatment have been reported in several articles, but no randomized controlled trial is available for comparing various operative treatments knowing that most of them were undertaken after failure of medical treatment. In our experience, about two-thirds of patients were symptom-free after vein compression, stenting, or embolization at middle-term assessment.
Keywords
Introduction
Pelvic congestion syndrome (PCS) is a common condition and reports indicate that more than 30% of women complain about pain in the lower abdomen at some time in their life. By no means are all pelvic symptoms attributable to PCS, so careful diagnostic procedures are required to identify those who may benefit from treatment of ovarian and pelvic vein syndromes. In PCS pain should be associated with other symptoms such as pelvic heaviness, dyspareunia, dysmenorrhoea, lumbar pain, urinary frequency and signs of vulvar and lower-limb varices, and haemorrhoids. It is admitted that symptoms should have been present for at least six months before considering PCS as a possible diagnosis.
Investigation of PCS
Many protocols are used to identify the presence of PCS and no comparative trial has been published to evaluate the currently used criteria. Nevertheless, there is consensus for agreeing that selective venography is the best investigation for identifying the anatomical and pathophysiological anomalies of PCS. Since selective venography is an invasive investigation, it is recommended that investigations start with non-invasive duplex ultrasonography that will demonstrate findings suggestive of PCS. In our daily practice we use an investigation diagram when female patients consult us for signs and symptoms described above (Figure 1).
Investigation algorithm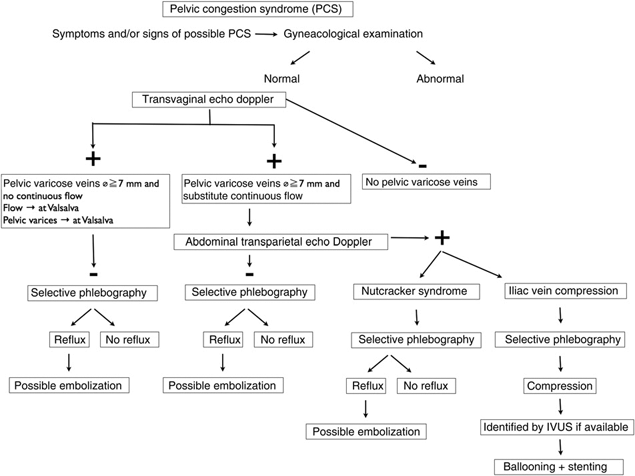
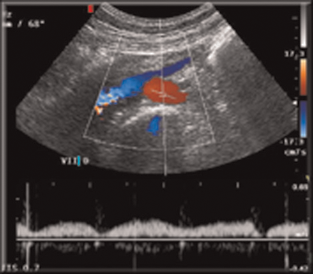
The first step is to eliminate a gynaecological disease which is the most likely source of pelvic symptoms. In those suspected of suffering from PCS, investigations start with transvaginal echo Doppler (TED). This investigation provides both anatomical and haemodynamic information. When pelvic varices are seen, which show continuous flow on Doppler imaging and this is not modified by a Valsalva manoeuvre, we undertake abdominal transparietal echo Doppler (ATED) in search of a vein compression syndrome (Figure 2). ATED can identify either left renal vein compression (Figure 3) or more frequently iliac vein compression (Figures 4 and 5).
Transvaginal duplex ultrasound. Pelvic varices with continuous flow Abdominal transparietal duplex ultrasound. Compression of left renal vein (Nutcracker syndrome)

When compression is identified by ATDE, more detailed information on the anatomy of the pelvic vein is sought by undertaking venography. We search for:
Left renal vein compression and possible associated ovarian reflux (Figures 6-8);
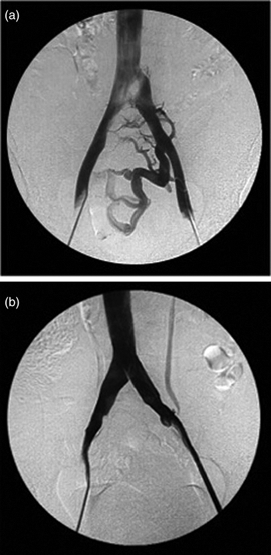
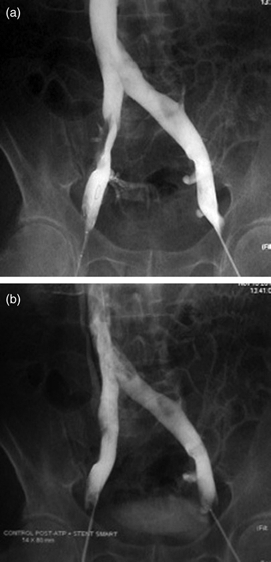
Iliac vein compression and possible reflux in internal iliac vein tributaries. (Figures 9a, b, 10a and b).
Conversely, when pelvic varices without continuous flow are found, but do show flow augmentation and dilation of pelvic varices induced by a Valsalva manoeuvre during TED investigation (Figures 11a and b), selective venography is considered to be the next step, as a vein compression syndrome is unlikely.
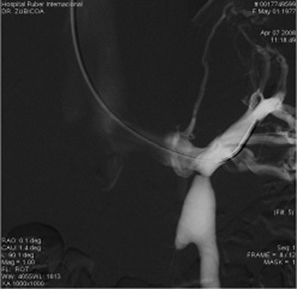
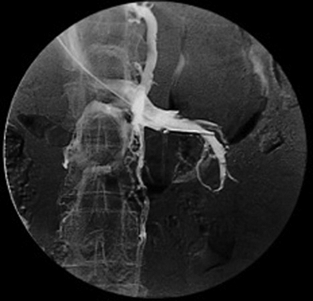
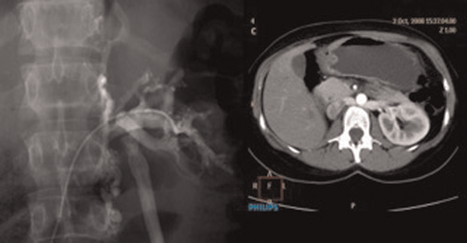
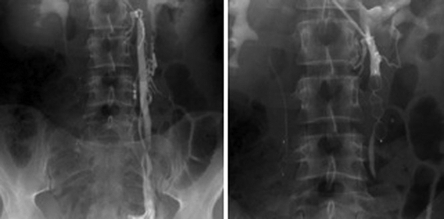
We use brachial access to undertake the venography since this allows confirmation of the absence of left renal vein and iliac vein compression. Reflux is investigated by selective venography and is frequently identified in ovarian veins (Figures 12a, b, 13-17) or iliac vein tributaries (Figure 18).
Abdominal transparietal duplex ultrasound. Compression of common left iliac vein (May-Thurner Syndrome) Abdominal transparietal duplex ultrasound (iliac vein compression syndrome). Compression of common right iliac vein Venography using brachial access. Left renal vein compression associated with left ovarian vein reflux Venography using brachial access. Left renal vein compression associated without left ovarian vein reflux Right venography using femoral access: left: retroaortic left renal compression with left ovarian vein reflux; right: computed tomography scan of same patient Venography using femoral access: (a) left common iliac vein compression and reflux in left internal iliac vein tributary, and (b) same patient after stenting. Reflux is no longer identified Venography using femoral access: (a) common right iliac vein compression, and (b) same patient after stenting. Reflux is no longer identified Transvaginal duplex ultrasound: (a) pelvic varices without continuous flow, and (b) same patient. Both venous flow and diameters of pelvic varices increase during a Valsalva manoeuvre (a) Venography using brachial access and selective ovarian vein catheterization. Valsalva manoeuvre: Unilateral ovarian vein reflux filling pelvic varices through a round ligament vein as well as lower-limb varicose veins, (b) Same patient during (left) and after (right) embolization. No more reflux into the ovarian vein and consequently no more pelvic and lower-limb varices are visible during a Valsalva manoeuvre Venography using brachial access and bilateral ovarian vein catheterization for assessing reflux. Right ovarian vein competent and incompetent. Left ovarian vein competent and incompetent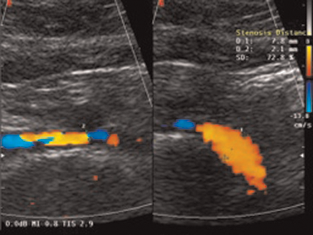



To summarize, the suggested diagram allows us to investigate a suspected PCS step-by-step to identify precisely which anomaly is present and likely to be responsible for the PCS.
Outcome after endovenous treatment according to published literature
Few articles have been published summarizing the outcome of treatment for PCS. We have included only articles reporting the outcome in more than 10 patients. The total number of patients summarized in Table 1 is 387.
1
8
Venography using brachial access. Incompetent right ovarian vein before and after embolization (Amplatzer) Venography using brachial access. Incompetent left ovarian vein before and after embolization (Amplatzer) Venography using brachial and femoral access. Simultaneous selective bilateral venography of incompetent ovarian veins filling pelvic and vulvar varices Venography using brachial access for catheterization of incompetent left ovarian vein filling through the pudendal vein pelvic and lower-limb varices. Same patient after embolization Clinical series reporting the outcome of embolization of pelvic and ovarian veins to treat PCS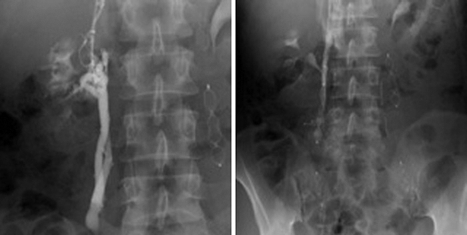



Some remarks can be drawn from the data: in these studies the aetiology of the syndrome was not identified. Symptoms and signs are frequently not clearly described and outcome criteria are different or vague making it difficult to compare results. There are therefore several aspects of the studies that are unsatisfactory. Nevertheless, it appears that the outcome is better when bilateral embolization is used.
Another bias should be pointed out. In most of these series, femoral access was used for selective venography. Catheterization of the internal iliac vein as well as right ovarian vein may be technically difficult from femoral access. Consequently, some sources of reflux may not have been identified. We recommend access via either the jugular vein or in preference the brachial vein which is more comfortable both for the patient and for the physician.
It is worthy to note that no randomized controlled trial comparing open surgery or laparoscopic procedures to endovenous surgery are available. Nevertheless, nowadays there is a large consensus for using the latter.
Venography using brachial access and internal iliac vein tributary vein catheterization. Reflux filling both pelvic varices and lower-limb varicose veins is identified after injection into internal pudendal vein and Valsalva manoeuvre. Same patient after embolization. No more reflux into internal iliac vein tributary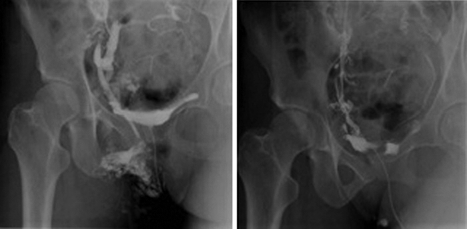
Personal series
Cause of PCS among patients after detailed investigations
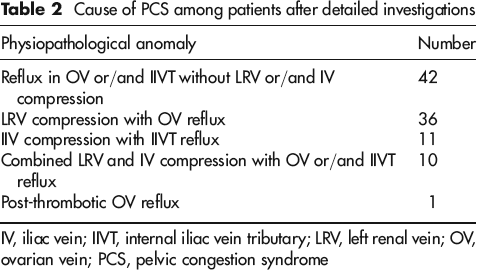
IV, iliac vein; IIVT, internal iliac vein tributary; LRV, left renal vein; OV ovarian vein; PCS, pelvic congestion syndrome
Reasons for seeking consultation among patients from the authors’ clinical series

LL, lower limb; CVD, chronic venous disease; PCS, pelvic congestion syndrome; Sy, symptom; Si, sign
The mean follow-up in this series is 14 months (12–18), age mean 42 (range 21–64).
The outcome of treatment has been assessed on the extent of postoperative pain. Sixty-four percent of patients had no more pain, 29% were improved and 7% unchanged.
Conclusion
Drugs can sometimes achieve temporary improvement in a proportion of patients with PCS. Hysterectomy is an obsolete treatment, and data on outcome after sclerotherapy are not conclusive. Open and laparoscopic surgery are more invasive than endovenous treatment and published outcome data are no better than those reported after endovenous treatment. At present, grade 1C recommendation for PCS endovenous treatment can be justified. To attribute a stronger recommendation we need long-term follow-up of clinical series as currently only one has reported a five-year follow-up. 7
Advances in endovascular treatments regularly provide new techniques for treating pelvic varices, and so long-term follow-up of any one system may be difficult. In addition, the experience and skill of radiologists and surgeons performing these treatments almost certainly have a major influence on the outcome. Comparison of different treatments, unless carried out in the same centre, will have little meaning.