
Abstract
Annually 1–2 in every 1000 adults will develop a deep venous thrombosis of the lower extremity. A third to half of these patients will develop the post-thrombotic syndrome (PTS). However, predicting which patients will develop the PTS remains elusive. Ipsilateral thrombosis recurrence seems to be the most important risk factor. Moreover, residual venous occlusion and valvular reflux seem to predict PTS incidence to some degree. Laboratory parameters, including
Introduction

NR, not reported; FU, follow-up; ECS, elastic compression stockings; Abstract only, only the abstract of the paper was available to the authors; PTS, post-thrombotic syndrome; DVT, deep venous thrombosis
Pathophysiology
CEAP Classification, adapted from Eklöf et al. 97
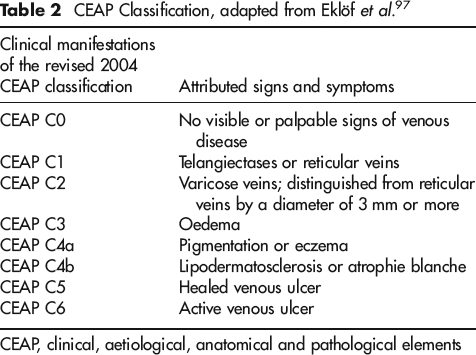
CEAP, clinical, aetiological, anatomical and pathological elements
Villalta score, adapted from Kahn et al. 98
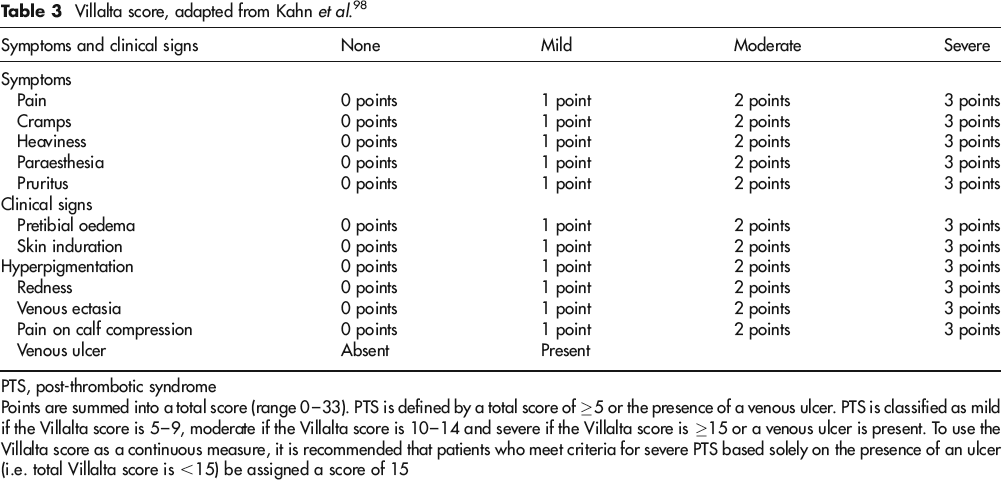
PTS, post-thrombotic syndrome
Points are summed into a total score (range 0–33). PTS is defined by a total score of ≥5 or the presence of a venous ulcer. PTS is classified as mild if the Villalta score is 5–9, moderate if the Villalta score is 10–14 and severe if the Villalta score is ≥15 or a venous ulcer is present. To use the Villalta score as a continuous measure, it is recommended that patients who meet criteria for severe PTS based solely on the presence of an ulcer (i.e. total Villalta score is <15) be assigned a score of 15
Current treatment options
The cornerstone of PTS prevention remains the use of elastic compression stockings (ECS) after a symptomatic DVT event. Studies on long-term use of ECS after a proximal DVT have shown a highly significant reduction in both mild/moderate PTS and severe PTS. 45 Therefore, it is generally recommended to prescribe below-knee ECS with a pressure gradient of 30–40 mmHg to patients with symptomatic proximal DVT. 46 Use of lower-pressure gradient stockings might increase patient satisfaction and therapy compliance; however, evidence on the lowest amount of pressure needed to prevent PTS is currently unavailable. Also, ECS treatment duration is controversial. Current guidelines advocate the use of ECS for two years or longer after an initial thrombotic event; however, Aschwanden et al. 3 recently showed no added effect of prolonging ECS treatment after six months for prevention of skin changes and PTS symptoms, suggesting that a decrease in treatment duration is feasible. Moreover, Roumen-Klappe et al. 28 suggest multilayer compression bandaging in the acute phase of DVT to have no effect on the development of the PTS compared with delayed compression therapy with stockings. Starting treatment solely with elastic stockings within two weeks post-DVT thus seems feasible.
Prevention of PTS is now the major focus of trials researching catheter-directed thrombolysis to treat proximal DVT (e.g. the Scandinavian CAVENT trial, the American ATTRACT trial and the Dutch CAVA trial). 47 49 Thrombolysis in the acute phase of DVT has been proposed to reduce long-term venous occlusion. Furthermore, rapid recanalization of venous tracts may reduce valve damage and avert deep venous insufficiency. Short-term studies have shown the safety and feasibility of this treatment modality; however, the long-term effects on PTS development are currently unknown. 50 53
During the last two decades a number of invasive treatments have been proposed to treat both deep venous insufficiency and persistent occlusion after a thrombotic event. A number of surgical procedures to treat venous valve insufficiency currently exist: internal and external valvuloplasty, 54 external banding, 55 the Maleti neovalve 56 and axial vein transfer. 57 Valvuloplasty is preferred by most authors. However, in a great number of patients valvuloplasty is not a viable option, due to destruction of the valve leaflets during the recanalization process in post-thrombotic legs. Persistent post-DVT occlusions are now being recognized as being of importance and treated in a number of specialized centres by angioplasty and stenting. Mid- and long-term follow-up show good results with primary patency rates of approximately 80% two years post-stenting and a clinically significant decrease in PTS symptoms; 58 60 however, randomized controlled trials of these treatments are lacking. In general, interventional treatment is only offered at select centres with expertise in these techniques to patients with severe persistent symptoms after the initial DVT.
In light of the limitations of the current treatment options, identification of risk factors for the development of PTS remains of greatest importance. Likewise, identification of high-risk patients will be needed in selecting patients for treatment with catheter-directed thrombolysis in the future.
Risk factors
Age
Differences between young and old patients might underlie differences in PTS incidence, though no clear mechanism has been postulated yet. Changes in the vein wall, hormonal factors, innate thrombus lysis, inflammatory response to thrombosis and mobility/calf muscle pump function might all differ by age. Advancing age has been clearly shown to be a risk factor for DVT, with incidence being very low in children (ranging from 34 to 58 cases of venous thromboembolism per 10,000 hospital admissions in children of <18 years of age) and increasing steadily to 3.1 per 1000 by the age of 85–89 years.61,62 However, the relation between age and incidence of PTS remains controversial. Conflicting reports in the literature have been put forward; some authors have described a positive correlation,17,30,31,63-65 some reported no correlation 17 and some even a lower incidence of PTS in older patients. 33 An increase of 0.3 points in the Villalta score per 10-year age increase was found by Kahn et al., 65 whereas Stain et al. 31 reported an odds ratio (OR) for PTS development of 1.2 for every 10-year age increase. Moreover, Schulman et al. 30 showed age above 60 years to be associated with a higher proportion of proximal DVT (58% versus 42%, P = 0.001) and a higher DVT recurrence rate (31% versus 25%, P = 0.049), compared with younger patients, both of which are independent risk factors for the development of PTS. A relationship between severity of PTS and age, however, has not been noted. 17
Obesity
Increased body weight has been proposed to lead to poor calf muscle function via lack of physical exercise, increased venous pressure and promotion of venous reflux. Obesity has indeed been associated with an increased risk of PTS.5,17,31,33,64,66 A 1.5-fold increase in PTS incidence in patients with a body mass index (BMI) ≥30 kg/m 2 has been described. 33 An increase in Villalta score of 0.14 and 0.16 per 1 kg/m 2 increase in BMI has been described by Kahn et al.17,65 in two studies. Furthermore, a higher BMI has been associated with less favourable QoL scores in PTS patients. 18
Gender
Summary of risk factors for PTS

PTS, post-thrombotic syndrome; DVT, deep venous thrombosis Risk factor's relation with PTS incidence: + + strong correlation, + moderate correlation, ± mostly unclear or no correlation
Unprovoked vs. provoked DVT
While surgery and trauma are associated with a high incidence of provoked DVT (ORs as high as 21.7 and 12.7, respectively 67 ), unprovoked DVT on the other hand might be an indication of an underlying hypercoagulable state that could lead to a higher incidence of recurrent thromboembolic events and PTS. However, a difference in the incidence of PTS after unprovoked versus provoked DVT has not been noted.5,11,31,68,69
Ipsilateral DVT recurrence
Ipsilateral recurrent thrombosis is common in DVT patients (Table 1). Two or more thrombotic events in the same extremity have been shown to increase the incidence of PTS,4,12,25,26,31,35,63 and previous ipsilateral thrombosis was associated with a 1.78-point increase in Villalta score.18,65 Conversely, presence of PTS was associated with a 6- to 11-fold increased incidence of recurrent DVT in patients treated with anticoagulants. 12 This might be explained by the findings of Young et al. 70 who showed an increased risk (hazard ratio 2.2) of DVT recurrence in limbs with residual thrombosis, as residual thrombus is also a known predictor of PTS. The mechanism by which DVT recurrence increases PTS incidence and/or severity most likely relates to aggravation of local venous damage and worsening of venous reflux via valvular destruction and extension of residual occlusion of affected vein segments. Kahn et al. 65 showed a 9.9% incidence of recurrent thrombosis during two years after treatment of DVT with anticoagulants; predictors of recurrence were cancer-associated venous thrombosis, unprovoked venous thrombosis, proximal (versus distal) thrombosis, symptomatic pulmonary embolism at study enrolment and male gender. Higher incidences of recurrence in patients with proximal DVT and in males have also been noted after longer patient follow-up.26,30,65 Increased contralateral recurrence has also been noted in a number of studies, probably via systemic vein wall defects, blood hypercoagulability or body habitus.12,35 A lower incidence of recurrence was seen after DVT provoked by surgery or trauma, conceivably because no underlying systemic venous aberrations were present. 26
Thrombus location
In many studies, proximal thrombi in the deep venous system (popliteal, femoral, common femoral and iliac veins) have been associated with a worse clinical and haemodynamic outcome and lower QoL scores than distal thrombi (peroneal, tibial, gastrocnemial, and soleus veins).9,15,18,23,31,33,65,71,72 Controversy remains, however, as some studies did not find this correlation.25,63 Kahn et al. found a PTS incidence of 52% in patients with proximal DVT versus 41 % in distal DVT, and a 2.23-point increase in Villalta score with proximal versus distal DVT.18,65 Similar findings were shown by Holmström et al. 15 QoL scores were also lower in patients with proximal versus distal DVT. 18 Van Ramshorst et al. 73 showed thrombus extent to correlate well with the number of refluxing vein segments at follow-up, but no association was shown for clinical severity. Eichlisberger et al. 7 showed a greatly increased incidence of PTS in patients with four-level thrombosis compared with those with popliteal vein thrombosis only (55% versus 4%, respectively) at 13 years after the initial DVT, and Tick et al. showed a 1.3-fold increase in PTS incidence with iliofemoral as compared with popliteal thrombosis. 33
Residual occlusion
Incomplete recanalization of thrombosed venous tracts is thought to impair the outflow of post-DVT extremities, thereby promoting venous hypertension. Johnson et al. 16 showed residual occlusion to be present in 80% of post-thrombotic limbs and reflux to be present in 83% (in 65% of limbs both occlusion and reflux were present). It takes a mean of 3.4 + 5.9 months to achieve 50% recanalization after DVT. 72 Prandoni et al. 74 found a relative risk for PTS development of 1.56 with the presence of residual vein thrombosis, and 1.69 if both residual vein thrombosis and popliteal vein reflux were present. In another study, they found a hazard ratio of 2.4 for recurrent thromboembolism in patients with residual thrombosis compared with those with complete recanalization. 75 This was confirmed in another study that showed the risk of DVT recurrence and mortality was increased in patients with residual occlusion after DVT (hazard ratios 2.2 and 3.9, respectively). 70 However, controversy remains as Haenen et al. 13 found no relation between non-compressibility or the combination of reflux and non-compressibility and PTS. Kahn et al. 17 found comparable results. Furthermore, the proportion of venous occlusion was reported to be the same in patients with CEAP scores of C0–3 and C4–6. 76
Residual reflux
Loss of venous valve function due to thrombosis has been proposed as one of the main pathological pathways by which PTS develops. Indeed, it has long been shown that reflux in the deep veins of the affected limb correlates well with incidence and severity of PTS.13,76,77 Yamaki et al. 76 showed peak reflux velocity in the popliteal and femoral vein on duplex to correlate highly (OR 60.32 for popliteal vein and 25.77 for femoral vein) with severity of chronic venous insufficiency. Haenen et al. 13 showed reflux in the proximal deep veins to be associated with worse CEAP scores (Table 2), but no such relation was shown for reflux in superficial veins and distal deep veins. In a second study, the same group showed superficial venous reflux to be the most important risk factor for onset of PTS symptoms and 64% of patients with severe PTS were shown to have a combination of superficial and deep reflux. 78 A combination of deep and superficial reflux therefore seems to underlie PTS pathogenesis.
Insufficient quality of anticoagulant therapy
Vitamin K antagonist treatment is still one of the cornerstones of DVT treatment. 46 Insufficient quality of anticoagulation might inhibit the recanalization process and worsen clinical outcome in the affected limb. Ziegler et al. 35 indeed showed this relation. They described insufficient anticoagulation measurements in half of the patients suffering from venous ulcers. More recently an increased incidence of PTS (OR 2.71) was described in patients whose international normalized ratio (INR) level was below 2.0 for >50% of the time. 64 Moreover, longer treatment duration with oral anticoagulants significantly reduces the risk of recurrent thrombosis, which is an important risk factor for PTS. 15
Thrombophilia
The presence of factor V Leiden or the G20210A prothrombin gene mutation has been shown to increase the risk of a first venous thrombosis.79,80 Moreover, in family members of patients with one of these mutations, an OR of 1.68 was found for DVT incidence. 81 There is conflicting evidence on the role of these thrombophilia markers on PTS incidence. Kahn et al. 17 showed factor V Leiden or the prothrombin gene mutation to be independently associated with a decreased incidence of PTS (OR 0.33) and a 1.6 decrease in Villalta score. However, in another study by the same group, these results could not be replicated and the same is true for a number of other recent studies.31,33,63-65
D-dimer
Elevated plasma
Inflammatory markers
Recently, a number of studies have focused on the role of inflammatory cytokines and adhesion molecules in the development of PTS. These include interleukin 6, 8 and 10 (IL-6, IL-8 and IL-10), C-reactive protein (CRP), monocyte chemotactic protein-1 (MCP-1), intracellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1). Studies were based on the hypothesis that the inflammatory response to DVT leads to vein wall abnormalities. PTS patients were shown to have a 1.6-fold increase in mean IL-6 level and a trend towards higher median levels of IL-6 four months after DVT diagnosis. 44 Roumen-Klappe et al. showed that IL-6 and CRP levels measured on the day of DVT diagnosis did not correlate with Villalta score one year post-DVT and only weakly correlated with CEAP classification one year post-DVT, but strong associations were seen between these markers and venous outflow resistance 90 days post-DVT (which in itself correlates with PTS incidence after 1 year), and in the case of IL-6, Porter's thrombosis score (based on thrombus extent and site involvement).43,91 ICAM-1 levels are also associated with PTS 44,92 No correlations between PTS and IL-8, IL-10, MCP-1 and VCAM-1 were shown.43,44 An association between inflammatory markers and reflux was not seen, supporting the notion that the inflammatory response may act on vein wall characteristics rather than venous valves.43,44,92 However, studies in animal models strongly suggest a role of inflammatory pathways in the development of venous valve degradation in chronic venous insufficiency, which indicates that secondary damage due to pathological haemodynamics post-DVT might contribute to PTS progression rather than initiation.93,94 Moreover, increased plasma levels of IL-6, IL-8 and MCP-1 have been shown to be increased in patients with recurrent DVT, which is an independent risk factor for PTS development. 95 The value of inflammatory markers in the prediction of PTS is currently being evaluated in a large prospective study. 96
Conclusion
General interest and awareness of the PTS have recently been stimulated by improved standardization of PTS measurement and the emergence of new potential treatment modalities such as new oral anticoagulants, catheter-directed thrombolysis and deep venous stenting procedures. However, effective stratification of the risk for progression to PTS in patients presenting with a first or recurrent DVT remains elusive. Recurrence of thrombosis in the same extremity as the index DVT, with resultant increased venous damage, seems to be one of the most important risk factors for PTS development. Residual venous occlusion and valvular reflux, signifying venous damage, also seem to predict PTS incidence to some degree. Based on promising preliminary work, the value of
Footnotes
Acknowledgements
SRK is a recipient of a National Research Scientist Award from the Fonds de la Recherche en Santé du Québec.