
Abstract
Objectives
This is a retrospective study over 12 years reporting the healing rates of leg ulcers at a specialist vein unit. All patients presented with active chronic venous leg ulcers (clinical, aetiological, anatomical and pathological elements [CEAP]: C6) and had previously been advised elsewhere that their ulcers were amenable to conservative measures only.
Method
Seventy-two patients (84 limbs) were treated between March 1999 and June 2011. Patients were contacted in August 2011 by questionnaire and telephone. Of 72 patients, two were deceased and two had moved location at follow-up, so were not contactable. Fifty patients replied and 18 did not (response rate 74%), representing a mean follow-up time of 3.1 years.
Results
Ulcer healing occurred in 85% (44 of 52 limbs) of which 52% (27) limbs were no longer confined to compression. Clinical improvement was achieved in 98% of limbs.
Conclusions
This study shows that a significant proportion of ulcers currently managed conservatively can be healed by surgical intervention.
Introduction
Venous leg ulcers are a severe manifestation of chronic venous insufficiency. Leg ulceration is estimated to affect 1% of the adult population, with 0.3% of people having an open ulcer at one time.1–6 Traditionally, ulcers have been treated almost exclusively in the community, using conservative treatments such as compression bandaging, which represent the mainstay of treatment in most practices. There has been a growing diversion of treatment away from specialist care in hospitals.5,7
In 1992, Darke and Penfold 8 demonstrated that 40% of patients with leg ulcers were associated with superficial venous incompetence and/or ankle perforating veins, with no reflux in the deep system. This study showed that 90% of these patients healed with saphenous ligation alone.8,9 More recent work has shown that up to 60% of ulcers are associated with superficial venous incompetence alone, and logically are potentially curable with superficial venous surgery.10–12
A recent Cochrane review found that ulcers treated with compression therapy healed faster than those without. 13 However, there is evidence to suggest that recurrence rates and ulcer-free time are more favourable following superficial vein surgery when compared with compression bandaging alone. The Effect of Surgery and Compression on Healing and Recurrence (ESCHAR) study of 500 patients compared the long-term results of compression therapy alone versus compression plus surgery. Although the results did not seem to suggest that superficial venous surgery improved ulcer healing, it did reduce the number of ulcer recurrences at four years and the amount of ulcer free time. 2 In 1999, a study showed that the majority of patients with venous ulceration and isolated superficial venous incompetence can obtain healing with superficial venous surgery, without requiring postoperative compression bandaging, skin grafting or perforator surgery. 14 A non-randomized study showed that superficial venous surgery reduced the ulcer recurrence over three years, from 44% without surgery to 26% with surgery. 15 Another group showed that in 200 ulcerated legs the patients treated surgically had an ulcer-free rate of 72% compared with 53% in the conservatively treated group. The mean follow-up times were 29 and 26 months in the surgical group and non-surgical groups, respectively. 16
In 2006, there was a retrospective study of 173 legs with active ulcers that were surgically treated with a combination of high ligation, stripping, subfascial endoscopic perforator surgery, debridement and fasciectomy of the ulcer. An impressive 87% of ulcers healed and the five-year recurrence rate was 4.6%. 4
Venous ulcers are a large burden to the National Health Service (NHS); estimated to cost £400 million per year in 2004. Venous ulcers also consume approximately 1% of the annual health-care budget in Western European countries.16,17 The estimated cost of each venous ulcer to the NHS in 1999 was in excess of £2000 each year; 40 times the cost of simple venous surgery. 18 It is acknowledged that a wider use of venous surgery to correct the underlying cause of ulcers may improve long-term outcomes for the patient. 19 Therefore, there is a clear economic as well as clinical agreement to cure leg ulcers surgically.
Despite this evidence, it would appear that there is a population of people with leg ulcers who are not being offered diagnostic tests for their superficial venous incompetence, or treatment of the condition if found. This paper shows our experience of a cohort of patients who presented with active venous leg ulcers (clinical, aetiological, anatomical and pathological elements [CEAP]: C6). They had previously presented to their local leg ulcer services and deemed unfit to be cured surgically, so had been offered conservative treatment only. They subsequently sought a second opinion and presented to our clinic. This study reports on the outcomes of those patients who we found to have a significant venous component to their ulceration, reversible with the latest venous surgical techniques. Due to the length of study period, these techniques changed over time as the techniques for treating superficial venous reflux have evolved. However, the principle of all treatments was the elimination of superficial venous reflux.
Methods
Seventy-two patients (84 legs) presented with currently active, chronic venous leg ulcers (CEAP: C6) between March 1999 and June 2011. The treatment group had a mean age of 68.8 years at the time of their first operation (range 21–92 years). There were 32 men and 40 women giving a male-to-female ratio of 1:1.25.
Patients self-referred or were referred by their general practitioner. Previously, they had all been managed conservatively, and had either been told that they were surgically incurable or had not been offered surgery.
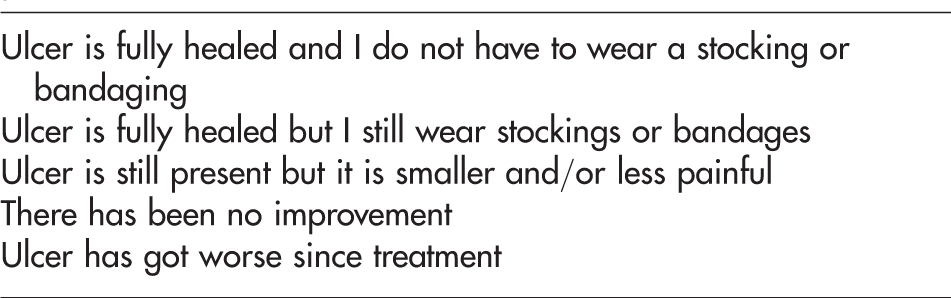
Questionnaire given to the patient to determine the subjective outcome of their treatment
As per our protocol, all patients presenting with active venous leg ulcers had had their lower limbs scanned using duplex ultrasound. Several different machines were used over the time period. All diagnostic scans were performed pre-treatment by two experienced vascular technologists (JMH and CCH).
Operations performed to treat venous reflux
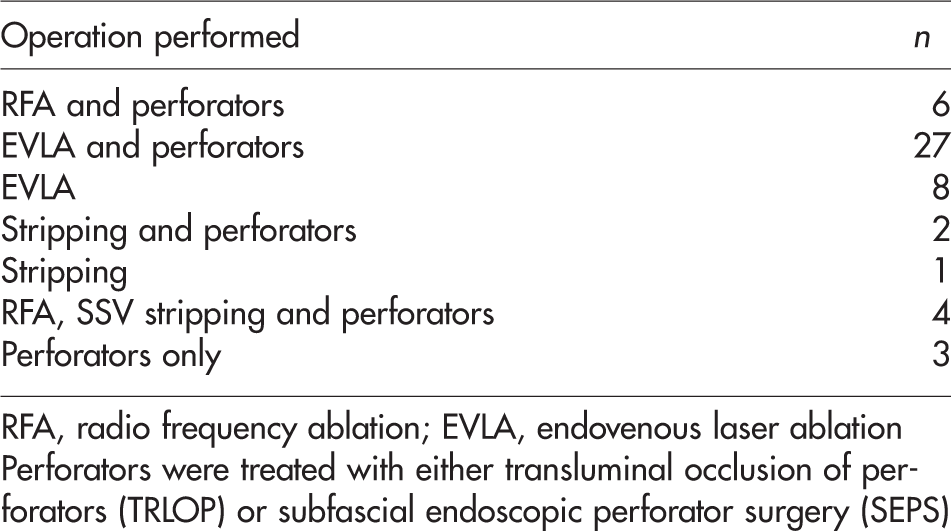
RFA, radio frequency ablation; EVLA, endovenous laser ablation
Perforators were treated with either transluminal occlusion of perforators (TRLOP) or subfascial endoscopic perforator surgery (SEPS)
Results
Patients
Of the 72 patients, two had deceased and two had moved location, so were not contactable. Out of the 68 contactable patients 50 replied to our questionnaire, giving a response rate of 73.5%. Four of these patients were excluded, as they were all still undergoing treatment.
Forty-six patients (52 legs) were included in the study (Figure 1). This represented 20 men and 26 women (male-to-female ratio of 1:1.3), with a mean age of 68.8 years at the time of their first operation (range 25–92 years). The time between operation and follow-up ranged from one month to 12 years with a mean of 3.1 years. A statistical comparison of the responders to the whole group showed no significant difference in terms of age and sex and therefore the study group is considered representative.
Trial profile showing the breakdown of limbs and patients treated in the study group
None of these patients had had previous arterial surgery, although one had had previous leg angioplasty, one had had previous coronary angioplasty and one had had previous coronary artery bypass grafting and stenting of coronary arteries. Four patients gave a history of possible previous deep vein thrombosis although none of them had deep vein reflux or occlusion on preoperative venous scanning.
Demographic data on patients in study

M, male; F, female; N, no; Y, yes; DVT, deep vein thrombosis; IBS, irritable bowel syndrome; MI, myocardial infarction; VV, varicose vein
Treatment
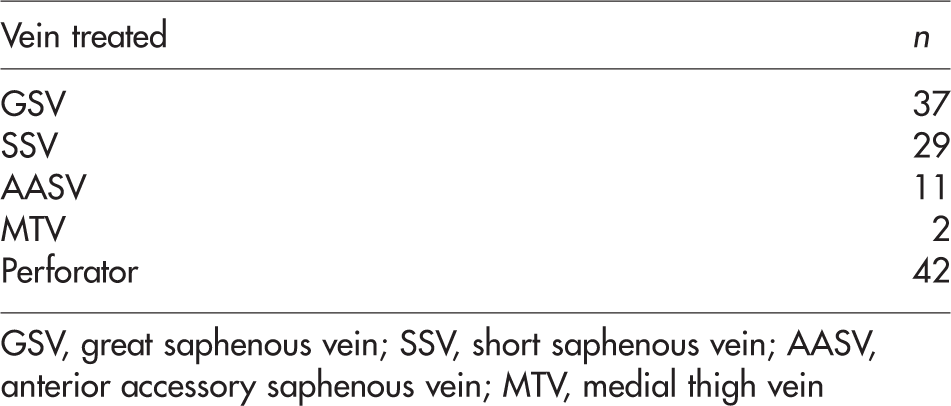
Combinations of vessels treated

GSV, great saphenous vein; SSV, short saphenous vein; AASV, anterior accessory saphenous vein; MTV, medial thigh vein
Shows the number of times each vein was operated on during the study period
GSV, great saphenous vein; SSV, short saphenous vein; AASV, anterior accessory saphenous vein; MTV, medial thigh vein
Different methods of treatment used

EVLA, endovenous laser ablation; RFA, radio frequency ablation; TRLOP, transluminal occlusion of perforator; SEPS, subfascial endoscopic perforator surgery
Healing rates
Forty-four (85%) of 52 legs had healed ulcers at follow-up. Furthermore, 27 (52%) of all the limbs were no longer confined to any long-term compression. Of the eight legs in which the ulcer had not healed at follow-up, seven reported that the ulcer had improved since surgery and was smaller and/or less painful. One patient reported that his ulcer was worse since surgery.
Reflux patterns in superficial and incompetent perforating veins, including whether reflux is primary or recurrent
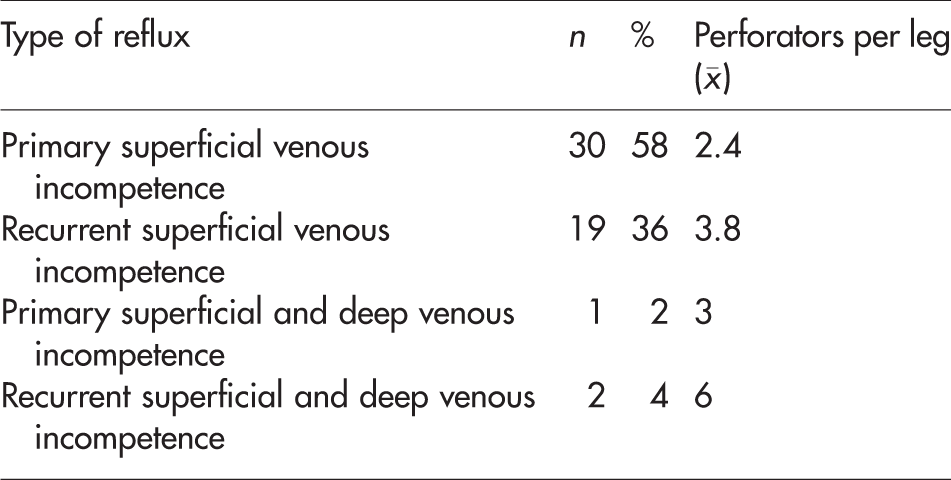
The presence of refluxing calf perforators was associated with 88% (74/84) of limbs with ulcers. Patients with primary reflux had a lower number of refluxing perforators compared with those individuals who had previously undergone attempted reflux corrective surgery. Only one patient had had any attempted surgery previously to her refluxing perforators in the form of subfascial clipping. The number of perforators in the limbs of the primary reflux group (n = 54) had a mean of 2.2, compared with 3.7 in the recurrent reflux group (n = 30). This is statistically significant. (P = 0.0028; unpaired t-test).
In our cohort, 30 limbs with primary reflux only in the superficial veins and perforators, received treatment and the ulcers were successfully healed in 26 (87%). In those with recurrent superficial reflux, 15 of 19 limbs had successful ulcer healing (79%). This difference does not reach the level of statistical significance (X2 = 0.083; P = 0.77). Only three limbs had a combination of deep and superficial reflux so that a reliable result regarding ulcer heal rate cannot be made. Figure 2 summarizes the ulcer healing rates of patients with primary or recurrent superficial reflux.
Pie charts demonstrating the ulcer healing rates of all patients in the study. (a) Patients with primary superficial reflux and (b) patients with recurrent superficial reflux
Discussion
All patients in this study had either been advised previously by their local leg ulcer services that their leg ulcers were not suitable for surgery or the appropriate diagnostic tests had not been performed. Therefore, they had been offered palliative compression bandaging and elevation of the leg, which is traditional treatment for gravitational or venous leg ulcers. However, studies have now shown that 60% of chronic venous ulcers are associated with superficial venous incompetence, so it is logical that surgical correction of the underlying superficial venous pathology should promote healing.10–12,14,15
In our unselected group of patients needing a second opinion, the treatment of superficial veins and perforators, using a variety of methods to correct reflux, resulted in ulcer healing in 44 of 52 legs (85%). Of the eight unhealed ulcers, seven showed improvement after surgery. The ulcer was either smaller and/or less painful. One patient reported his ulcer to be worse since surgery. Therefore, it is reasonable to conclude that treatment was beneficial for 98% of patients in our cohort.
Of course it is important to note that we are looking at a self-selected group of patients. As we are a specialist unit in the private sector, all of these patients were motivated to find out about our services themselves to either request referral from their general practitioner or other doctor, or to self-refer.
Of note are the perforator data collected in this study; ulcerated limbs with recurrent reflux were found to have, on average, a significantly higher number of incompetent perforators than those with primary reflux, previous studies have also found patients with recurrent varicose veins to have a greater number of incompetent perforating veins than patients with primary varicose veins. 20 This suggests that the original vein surgery they underwent in an attempt to correct their refluxing veins had not dealt with the perforators effectively or had not targeted the perforators at all, resulting in them suffering the effects of more perforators over time. In fact, only one out of the 30 recurrent patients had had previous surgery to correct their incompetent perforators in the form of subfascial clipping.
The ESCHAR study of 500 patients showed that patients with isolated superficial venous reflux had the best clinical outcome. 2 Patients in this study with primary and superficial reflux appeared to have a better outcome and had the highest ulcer healing rate of 86.7%. Patients with recurrent venous reflux had a lower cure rate of 78.9%, and although not statistically significant, it suggests that recurrent venous incompetence is more difficult to treat than primary superficial venous incompetence. This may be due to the hostility of the tissues secondary to chronic longevity and increased scarring from previous surgeries being present.
We looked for any factors that would influence outcome, looking at healed against not healed ulcers. Having analysed the data no significant difference was found in age or sex. One factor which was significant was the presence of lymphoedema severe enough to require preoperative treatment. Of those whose ulcers did not heal six of eight had lymphoedema severe enough to require preoperative treatment, whereas of the ulcers that healed, 12 of 44 had lymphoedema. This is a statistically significant difference (X2 = 5.76; P = 0.016). From this it can be assumed that it is harder to treat these patients resulting in poorer outcomes.
The influence of lymphoedema coexisting with superficial venous reflux in patients with leg ulcers is clearly a complex one. For this simple retrospective study we have assumed all of these ulcers to be due to superficial venous reflux as this was identified on duplex ultrasonography. We have therefore noted the presence of significant lymphoedema and, when found and patient amenable, have recommended manual lymphatic drainage as part of the preoperative strategy. This simplistic approach would warrant further investigation in future studies to ascertain the importance of the lymphoedema in the ulceration process.
Despite evidence showing that the majority of leg ulcers are associated with superficial venous incompetence, which is potentially correctable,10–12,14,15 the patients used in this study had either been labelled as ‘incurable’ or not offered surgery. Age, infirmity and perceived risks to patients undergoing general anaesthesia maybe factors in the clinical decision-making, as well as the high-morbidity considerations from the presence of a large open ulcer with a high surface bacterial population. However, with the arrival of modern techniques using local tumescent anaesthesia, it should be possible to be far more inclusive with patients who were previously denied surgical options.
There appears to be a passive approach to venous ulceration from a number of institutions. Some recently formed ‘leg clubs’ do not appear to advocate active investigation, diagnosis or cure in their online information. A quote from one brochure states ‘through education and on-going advice and support, members are taught that the care and the prevention of recurrence of leg-related problems is for life, and that prevention is better than cure’. 21 This suggests that the ulcer is an ongoing problem rather than a treatable event, which is erroneous in a large proportion of cases.
Of course there are weaknesses with this study which are recognized by the authors. It is a retrospective study that used as its entry criteria patients who had been referred to this private specialist unit who had not been cured previously by recommended treatments, and who were deemed suitable for surgery on the results of their venous duplex scans. Leg ulcers due to deep vein occlusion or isolated deep-vein reflux without a superficial component were not offered superficial venous surgery and therefore were not included.
Also, as a retrospective study, the follow-up was performed at the time the study meaning the range of follow-up was between one month and 12 years rather than a regular follow-up where points of healing and recurrences could be identified precisely. This precludes us from presenting our results as a life table analysis but, on a positive note, as the mean follow-up was 3.1 years, and the healing rate is so good, it does suggest that the treatment of the superficial venous reflux has a long-lasting effect in a number of patients. Clearly, a prospective observational study would be useful which would include size of ulcer, chronicity and then regular follow-up for life table analysis. Such a study is being considered in our unit and will be performed if ulcer patients continue to present without having had the option of superficial venous surgery.
Despite these weaknesses in this study, it is clear from this study alone that there are a number of patients who do not have the underlying cause of their leg ulcers treated for a variety of reasons. We contend that a more aggressive approach to investigation and treatment is required to reduce the number of ulcer patients in the population, and with it the burden on already overstretched hospital and community services.
In conclusion, our study has revealed an ulcer heal rate of 85%, and improvement in 98% of patients suffering chronic venous leg ulcers, refractory to established conservative management and who had not been offered surgery. In the light of recent treatment developments used in this study, we suggest a more active strategy may be effective for patients with venous leg ulcers.