
Abstract
Objective:
A pilot study to clarify the association between popliteal vein compression (PVC)and deep venous thrombosis (DVT).
Method:
It is assumed that PVC and the associated change in blood flow increases the likelihood of DVT. We have selected patients who were referred to a vascular laboratory for a DVT duplex and scanned for both DVT and PVC. Duplex criteria for the diagnosis of a DVT were lack of flow and inability to compress the vein. The study was performed over 12 weeks.
Results:
Of the 54 eligible patients, 16 had a DVT. Five of 18 patients with PVC had a distal DVT (27.7%), while five of 36 patients without PVC had distal DVT (16.7%). The difference was statistically significant (relative risk 2.9, P < 0.05).
Conclusion:
There appears to be an association between the presence of PVC and an increased likelihood of developing a DVT. If confirmed in larger studies, this will have strong implications for patient positioning in theatres, as there is a high incidence of PVC in supine anaesthetized patients.
Introduction
It is assumed that popliteal vein compression (PVC) increases the incidence of perioperative deep venous thrombosis (DVT). 1 Patients who are supine and under general anaesthetic are at risk of heel pressure ulcers. The European Pressure Ulcer Advisory Panel (EPUAP) and the corresponding North American (NPUAP) body recommend that these patients should have the heel off-loaded to prevent heel pressure ulcers. 2 The incidence of PVC in patients who are supine and under general anaesthetic with the heel off-loaded is 64%. 3 PVC results in decreased venous outflow 1 and decreases the efficiency of calf compressors. 4 This pilot study attempts to clarify the association between PVC and DVT.
Method
Consecutive patients who were referred to the South Coast Vascular Laboratory for venous duplex scans for possible DVTs were also examined for PVC. Reasons for referral were various; however, all patients were at risk for DVT. The incidence of PVC in the group who did not have a DVT was then compared with the group who did have a DVT.
Duplex scans were used for the study. Consecutive patients were examined and data collected pro-spectively. Qualified vascular technicians using Toshiba Xario XG duplex scanners performed all examinations. PVC was defined as a decrease in the diameter of the popliteal vein of 50% or greater which, in the context of this paper, is being studied specifically with regards knee hyperextension. The figure of 50% was chosen from the paper by Leon, 1 in which he showed that subjects who have a diameter reduction of greater than 50% have a significantly reduced venous outflow fraction (VOF). The VOF returns to normal when the knee is slightly flexed.1, 3 Measurements were done when the subject was standing with the knee flexed, then locked, and again when the subject was lying on a horizontal surface with the knee flexed, and then with the heel off the bed and the knee allowed to fall back unsupported (hyperex-tended). The full length of the popliteal vein was studied for compression and the maximum diameter measured when the knee was flexed, and again when the knee was locked. A similar procedure was done when the subject was lying.
A DVT was diagnosed by duplex scan using venous compression and the absence of venous flow. All veins from the calf to the iliac veins were studied. Any isolated DVT in the peroneal or posterior tibial vein was sufficient to be positive.
Statistics
The statistics were performed using Excel with Add-in Analyse-it.
A Fisher's exact test was utilized to establish the relative risk (RR) of DVT in those whose popliteal vein is compressed by >50% on hyperextension of the knee compared with those whose popliteal vein is compressed by < 50%.
Results
Sixty-one subjects were referred to the South Coast Vascular Laboratory with symptoms or signs consistent with a DVT, or when a DVT was suspected. Of these, 16 had a DVT; however, five had DVTs which involved the popliteal vein. Because this study relies on the phenomenon of change in flow with venous occlusion, and its knock-on effect of likely increase in DVT, these five patients whose popliteal vein was already occluded by thrombus were not included in the study.
Two further subjects were excluded. One was excluded because he could not extend the knee and could not be examined for PVC. A second was excluded because he had a history of previous DVTs, the wall of the vein was thickened, making PVC studies inaccurate.
This left 11 subjects with a DVT and a popliteal vein suitable for examination, and 43 subjects who did not have a DVT. The distribution of patients is shown in Table 1. Thirty-three percent of all subjects had PVC. Of the 11 subjects who had a DVT, 45% had significant PVC. Of the 43 subjects who did not have a DVT, 30% had PVC. The difference was statistically significant with a RR of 2.9 with P < 0.05.
Relationship between DVT and popliteal compression (n = 54)
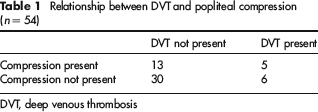
DVT, deep venous thrombosis
Discussion
PVC (as opposed to popliteal vein entrapment) is a condition, which was described by Leon 1 who examined the popliteal veins of 100 subjects. He found that the popliteal vein was compressed with a diameter reduction of greater than 50% in 17% of subjects. This was significant, because the VOF, as determined by volume plethysmography, was either moderately or severely depressed in all these subjects. The VOF reverted to normal in all when the knee was flexed. A subsequent study looking at patients who were supine and anaesthetized with the heel off-loaded (to prevent heel pressure ulcers) had an incidence of PVC of 64%. 3 The question that we have tried to address in this pilot study is whether there is an association between PVC and DVT.
In this pilot study, it would appear that the presence of PVC significantly increases the risk of developing a DVT (RR = 2.9, P < 0.05). In a larger study, precise positioning of DVT would be useful and informative, as would the association between degree of PVC and the prevalence of thrombosis. In addition, in a larger study, correlation between the above and age, weight and gender may also be useful. These data were not collected in this study.
Approximately 60% of operations are performed with the patient supine and the heel off-loaded (as is recommended in the EPUAP/NPUAP consensus document 2 ) and a large proportion (up to 64%) have PVC. 3 This means that many patients (up to 39%) undergoing surgery are at unnecessary increased risk of DVT due to PVC. Although this is a small study, until a definitive study is conducted, we recommend that patients who are undergoing surgery and are supine and anaesthetized should have the heel elevated and the knee flexed slightly in order to prevent PVC. This is the current recommendation of the EPUAP/NPUAP consensus document. 2 This needs to be done without placing anything behind the popliteal fossa, as the weight of the leg is enough to compress the popliteal vein (Huber D, unpublished magnetic resonance imaging data). This must also be done using a supportive device that distributes the weight of the leg over a large area, as other techniques may place parts of the leg or other body areas, at risk of pressure ulcers. 5
To conduct a definitive case/control study with a power of 0.95, 110 patients with DVT would be required. This is based on the rate of PVC in patients without DVT (i.e. the rate of exposure in the control group) found in this study, and the calculated RR of 2.9. It is also assuming that people with PVC have a higher incidence of DVT, and therefore the calculation has been done with a one-tailed t-test.
Conclusion
This pilot study shows that there is a likely increased risk for DVT in patients who have PVC. A larger study would need to be done to confirm these findings. If confirmed, there would be significant ramifications in the way patients are positioned in the operating theatre.