Varicose veins and chronic venous disorders (CVD) have been categorized using various clinical classifications such as the Widmer or Porter's classification of venous disease.1,2 However, these classifications could not reflect clinical signs related to CVD. These classifications also focused mainly on clinical severity but did not differentiate between underlying aetiology and pathology. An international ad hoc committee initiated the process to introduce a classification scheme that did take this differentiation into account. Its aim was to develop a comprehensive classification combining the manifestation of different clinical stages and underlying aetiology and pathology. In 1994, the CEAP (clinical, aetiological, anatomical and pathological elements) classification was introduced and since then has been widely used in practice and scientific settings.3 Recently, the basic CEAP classification was revised recognizing that the merits of using the full advanced CEAP classification system is reserved for standardized reporting in scientific journals.4 In practice, it has been found that there is a need for additional classification of symptomatic or asymptomatic varicose veins and a differentiation between the clinical signs in the C4 into two groups of symptoms. It also appeared that in practice many physicians do mostly use the C of the CEAP classification to categorize venous disorders. In published articles, patients are categorized into C0–C6, the majority of which is classified as having C2 varicose veins.5,6 Yet, we are led to doubt the correctness of this classification. As an example, a patient classified as C2 in the CEAP classification in interventional studies may not have visible clinical trunk varicosity (Figures 1 and 2), but may have reflux as determined by duplex examination. In our opinion this patient should be classified as C0-1, Ep, As, Pr. Thus, the duplex can misleadingly determine the C classification as it is common practice to always classify a patient with reflux of a truncal or tributary vein as C2, irrespective of the visible veins. As a second example, a patient with visible telangiectasias and primary reflux in the proximal great saphenous vein will always be classified as C2, Ep, As, Pr. However, in our opinion the clinical class should be C1, Ep, As, Pr (Table 1 and Box 1).
Revised C of the CEAP classification
C0
No visible or palpable signs of venous disease
C1
Telangiectasias or reticular veins
C2
Varicose veins
C3
Oedema
C4a
Pigmentation or eczema
C4b
Lipodermatosclerosis or atrophie blanche
C5
Healed venous ulcer
C6
Active venous ulcer
S
Symptomatic, including aches, pain, tightness, skin irritation, heaviness and muscle cramps, and other complaints attributable to venous dysfunction
A
Asymptomatic
CEAP, clinical, aetiological, anatomical and pathological elements
Box 1 CEAP classification
Venous disease of the legs can be classified according to the severity, cause, site and specific abnormality using the CEAP classification. Use of such a classification improves the accuracy of the diagnosis and improves communication between specialists. The elements of the CEAP classification are:
Clinical severity (0–6)
AEtiology or cause (primary, secondary)
Anatomy (superficial, perforating, deep)
Pathophysiology (reflux, obstruction, both)
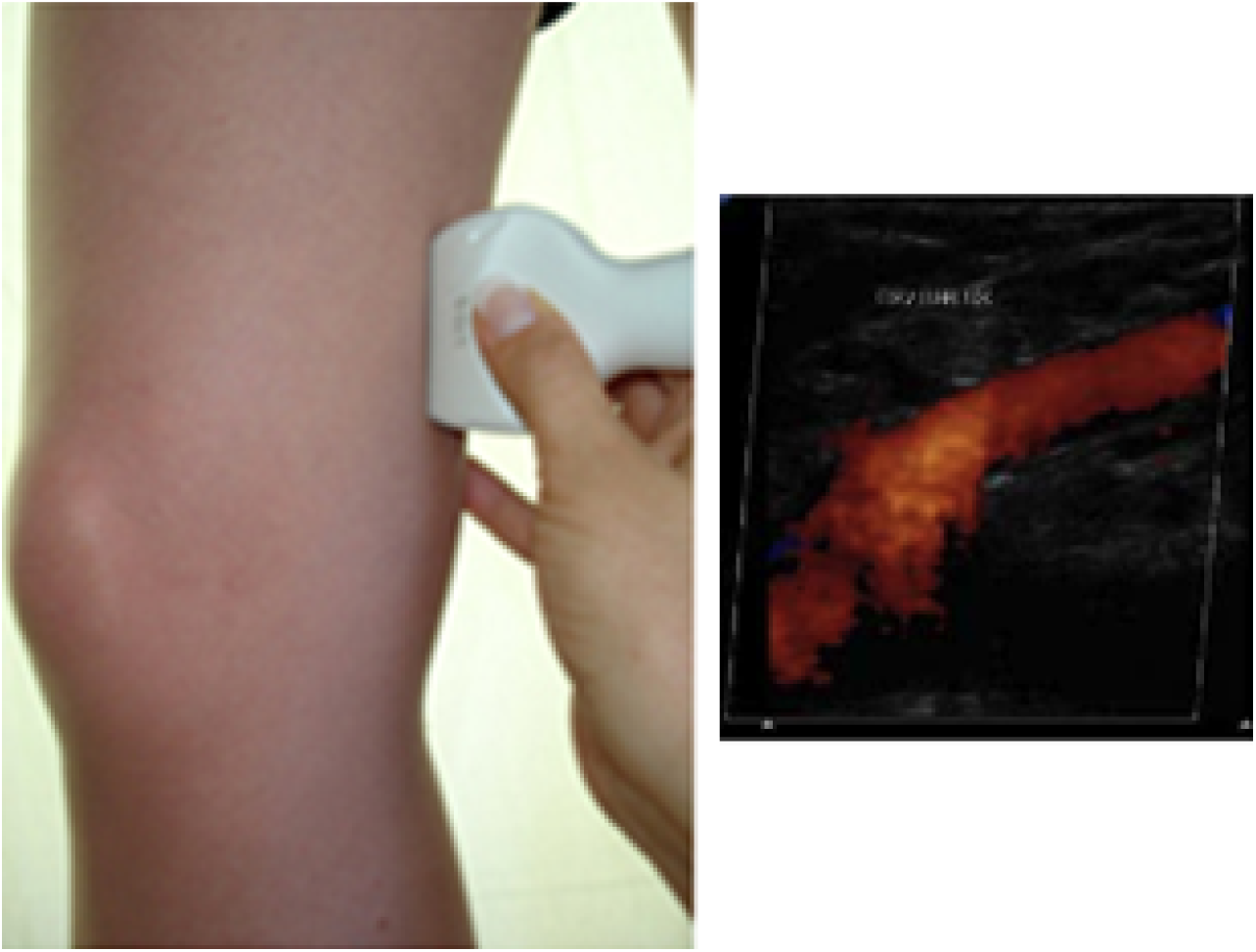
Patient with venous complaints, no visible varicosity in the truncal area, yet with duplex examination reflux in GSV above knee is found (C0sEpAsPr2). GSV, great saphenous vein
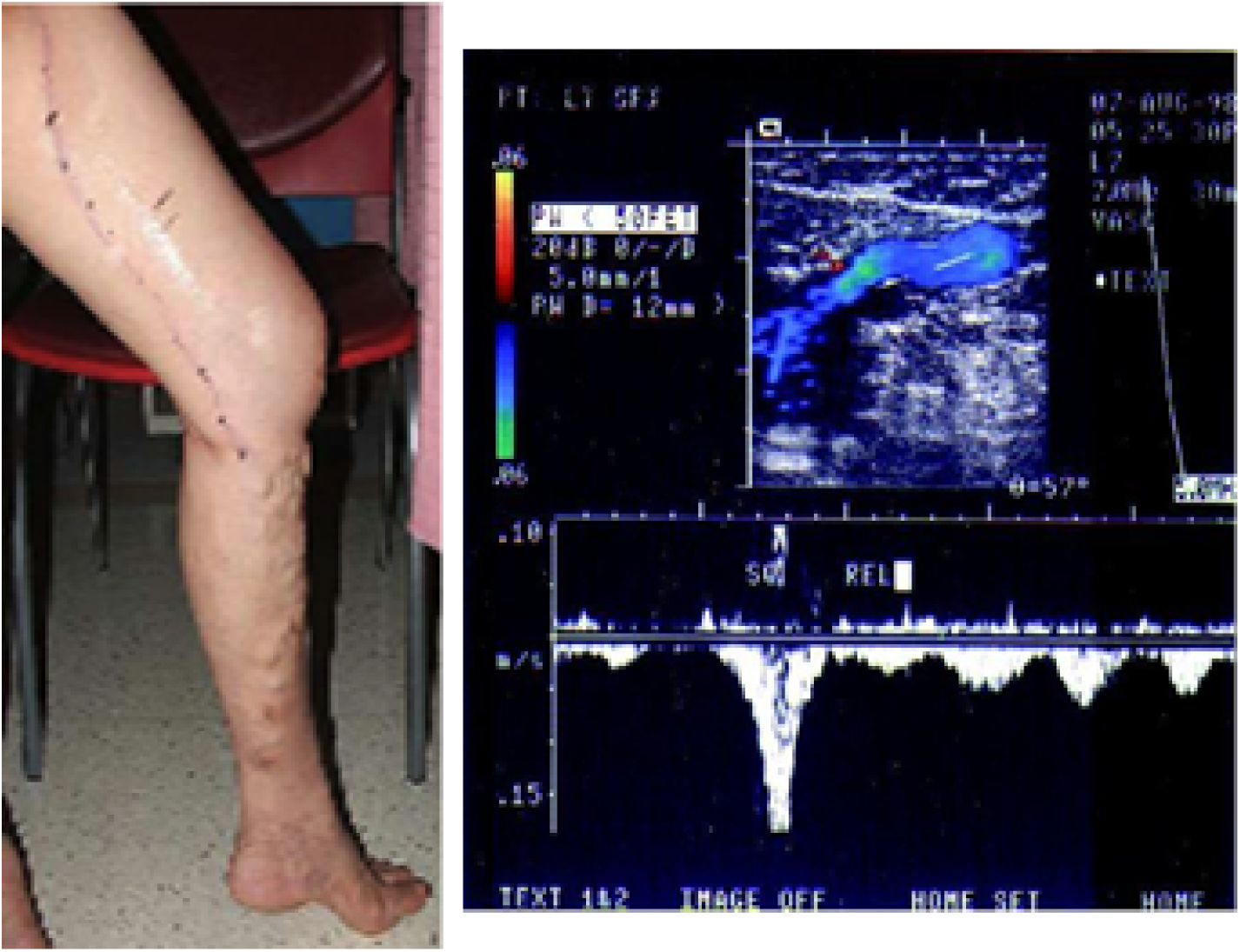
Varicose veins in truncal area (C2EpAsPr2,3) with reflux detected from the groin to the ankle
That implies that also stage C0 and C1 can represent a venous disorder that should be treated as it is haemodynamically compromising the venous return.
We therefore conclude that there are some discrepancies in the use of the C component in the CEAP classification. We would like to suggest the need to at least combine the C and the P (reflux or obstruction) of the classification. Also, we suggest physicians should define patients clinically into C0 and C1 if no varicose veins are visible (adding an s = symptomatic in case of venous complaints) and also add Pr if duplex shows reflux in the truncal vein. Combining C and P would help to characterize venous disorder and leads the clinician to the proper treatment.
References
1.
WidmerLKZempE. Diagnosis and treatment of varicose veins. Deductions from on a Basel prospective epidemiological study. Helv Chir Acta1988;54:531–9
2.
PorterJMMonetaGL. Reporting standards in venous disease: an update. J Vasc Surg1995;21:635–45
3.
BeebeHGBerganJJBergqvistDClassification and grading of chronic venous disease in the lower limbs: a consensus statement. Vasc Surg1996;30:5–11
4.
EklöfBRutherfordRBBerganJJFor the American Venous Forum International Ad Hoc Committee for Revision of the CEAP Classification, revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg2004;40:1248–52
5.
ProebstleTMAlmJGöckeritzOThree-year European follow-up of endovenous radiofrequency-powered segmental thermal ablation of the great saphenous vein with or without treatment of calf varicosities. J Vasc Surg2011;54:146–52
6.
ChristensonJTGueddiSGemayelGBounameauxH. Prospective randomized trial comparing endovenous laser ablation and surgery for treatment of primary great saphenous varicose veins with a two-year follow-up. J Vasc Surg2010;52:1234–41