
Abstract
Objectives
We tested a novel technique to treat great saphenous vein (GSV) incompetence in an animal model.
Methods
V-block (VVT Medical Ltd, Kfar Saba, Israel), an occlusion device composed of a nitinol frame and anchoring hooks, was percutaneously deployed at the saphenofemoral junction in 12 sheep. Four of the 12 sheep were treated with adjunctive liquid sclerotherapy. Animals underwent duplex ultrasound, venography and histopathological evaluation immediately postimplantation at 30, 60 and 90 days.
Results
V-block was successfully deployed in all animals without adverse events. There was no device migration at follow-up. Histopathological analysis demonstrated V-block to be lodged within the GSV and surrounded by fibrous tissue in all samples. Obliteration of the GSV lumen, widespread intimal loss and multifocal medial smooth muscle loss was noted.
Conclusions
In this animal study V-block was deployed without complications, remained in stable position and led to GSV occlusion. This device has promise for future use in humans.
Introduction
Chronic venous disease (CVD) is caused by primary or secondary venous insufficiency that results from venous obstruction, valvular incompetence or calf muscle pump failure. Chronic venous insufficiency (CVI) leads to ambulatory venous hypertension and an array of other pathophysiological processes, currently under active investigation, which result in a wide spectrum of disorders whose manifestations range from varicose veins to leg ulceration. 1 CVI has a high prevalence, 1 is a source of significant morbidity,1,2 significantly affects the quality of life 3 and is responsible for significant health expenditure.1,4
Great saphenous vein (GSV) reflux is an important component of primary venous insufficiency and is commonly treated in symptomatic patients. Although the traditional treatment of GSV reflux was ligation and stripping of the GSV,5,6 minimally invasive techniques have recently displaced this surgical procedure.7–9 Percutaneous endovenous thermal ablation using radiofrequency 10 or laser 9 avoids the need for surgical incisions, has excellent efficacy, decreased postoperative pain and leads to quicker recovery.8–10 Thermal ablation of the GSV, however, requires the utilization of tumescent anaesthesia, is associated with risk of thermal injury to surrounding tissues and has a 16% rate of recurrent reflux at five years.8,9 Chemical ablation of the GSV using ultrasound-guided foam sclerotherapy has been shown to have excellent success rates but has been associated with thrombophlebitis, visual disturbances and stroke.11–13
V-block (VVT Medical Ltd, Kfar Saba, Israel) is an occlusion device that can be percutaneously positioned at the saphenofemoral junction and can lead to successful occlusion of the GSV. When incorporated with liquid sclerotherapy, using a proprietary double piston syringe system, it can allow for successful chemical ablation of the GSV without the need for tumescent anaesthesia. We have investigated the safety and efficacy of V-block with and without concomitant sclerotherapy in an animal model.
Materials and methods
V-block device and delivery system
The V-block device (VVT Medical Ltd) was designed for percutaneous occlusion of the proximal GSV. It consists of a conical, nitinol frame partially covered by a thin polytetrafluoroethylene membrane. A coil-shaped nitinol filter, attached to the inner base of the device, serves to capture and retain thrombus in order to avoid pulmonary embolism. Secure fixation of the device to the GSV wall is dependent on radial force and is bolstered by nitinol hooks positioned at its outer base (Figure 1a). The V-block device is deployed with the struts oriented distally and has a closed as well as open configuration. It is packaged in its open configuration, in a proprietary 6F delivery system (Figure 1b) which consists of a low-profile introducer catheter, a magazine containing the preloaded V-block and a pusher rod which allows for V-block deployment. The pusher rod contains an inner lumen that can be used for injection of liquids, while the cavity between the external grooves of the pusher and the catheter can be used for negative suction, which can maintain a negative pressure at the tip of the delivery catheter.
(a) The V-block device. (b) V-block delivery system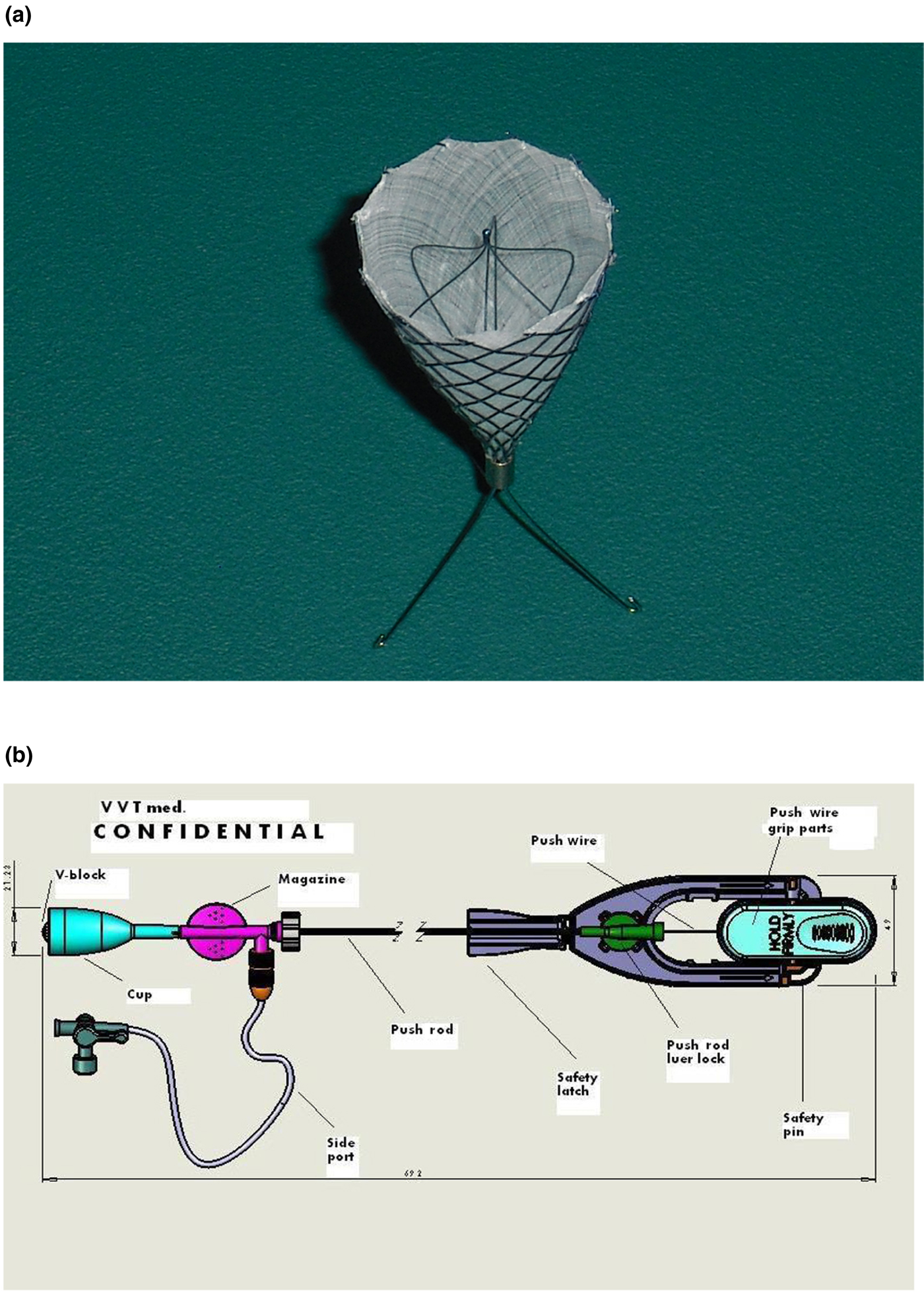
The Dual Procedure Syringe System, a proprietary, double piston syringe may be attached to the catheter. One syringe may contain a sclerosing agent that can be injected into the vein. This syringe is mechanically coupled to a second syringe, such that when the first syringe is pushed the second syringe is simultaneously withdrawn. The result is that the second syringe creates vacuum that results in the removal of blood from the vein.
Upon percutaneous insertion, using the Seldinger technique, the V-block delivery sheath is advanced, under ultrasound guidance, into the GSV and positioned with its tip 1–2 cm distal to the saphenofemoral junction and immediately distal to the superficial epigastric vein. The magazine containing the V-block is engaged with the sheath, and the pusher is used to advance the device to its final, predeployment position in the proximal GSV. The sheath is then pulled back to expose the constrained device, which can still be repositioned, if necessary. The device is released using a trigger wire and when fully deployed adopts its open conical configuration. The V-block device, when open, leads to significant flow restriction within the vein. At this point, the Dual Procedure Syringe System is attached to the V-block delivery catheter. Negative pressure on the catheter tip allows for removal of a significant amount of blood from the vein and leads to partial vein collapse, while in turn, a liquid sclerosant is injected into the vein. The delivery system is pulled back as sclerotherapy of the GSV is completed.
Animal model
The V-block device was evaluated for safety and efficacy in a sheep model, and the study protocol was approved by the Chaim Sheba Medical Center Animal Research Ethics Committee. Sheep were anaesthetized by a veterinarian using accepted standards and in compliance with local institutional animal care protocols. Once the animals were asleep, their hind legs were shaved, prepared with a disinfectant solution and draped in a sterile fashion. Access to the distal GSV was obtained, percutaneously, under duplex ultrasound guidance (Titan, SonoSite Inc, Bothell, WA, USA). The V-block delivery sheath was introduced into the GSV at the distal hind limb under ultrasound guidance, through a single entry needle, using the Seldinger technique over a 0.035-inch guidewire. The V-block device was inserted and positioned, under duplex ultrasound guidance, 1–2 cm distal to the saphenofemoral junction. Eight animals were treated with V-block placement alone. Four animals were treated with V-block placement and concomitant liquid sclerotherapy (3% sodium teradecyl sulphate, Spectrum Laboratories, New Brunswick, NJ, USA), using the Dual Procedure Syringe System. One control sheep was treated with high GSV ligation alone. Periprocedural evaluation included clinical assessment of the implantation site and duplex imaging to assess GSV diameter, final device position, GSV patency and assessment of flow across the V-block device after deployment. Contrast venography to assess final device position was also obtained. The animals were housed individually, and their vital signs were monitored daily. Follow-up assessments, on selected animals, were performed at 12, 30, 60 and 90 days after implantation.
In order to assess the short-term interaction between the V-block device and the GSV one animal was sacrificed immediately after successful device implantation. Two sheep were sacrificed after 30 days, five sheep were sacrificed after 60 days and then four animals were sacrificed after 90 days of follow-up.
Duplex ultrasound evaluation of the GSV to assess for device migration was performed in all sheep at 12, 30, 60 and 90 days. The index GSV, contralateral GSV used as control and lungs were harvested at follow-up intervals and fixed in 10% formalin. Gross pathological examination was carried out using visual inspection of the fixed gross specimens and documentation of the macroscopic findings at the implantation site. Multiple serial GSV sections were collected at 1 cm intervals around the device, proximal to it and distal to the V-block deployment site. Sections were stained with haematoxylin and eosin. Identical sections were obtained from untreated veins in contralateral extremities. Lungs were examined for evidence of thromboembolism. All pathological specimens were evaluated by a veterinary pathologist certified by the American College of Veterinary Pathologists. Outcomes in animals treated with V-block alone were compared with normal veins and control animal treated with GSV ligation.
Results
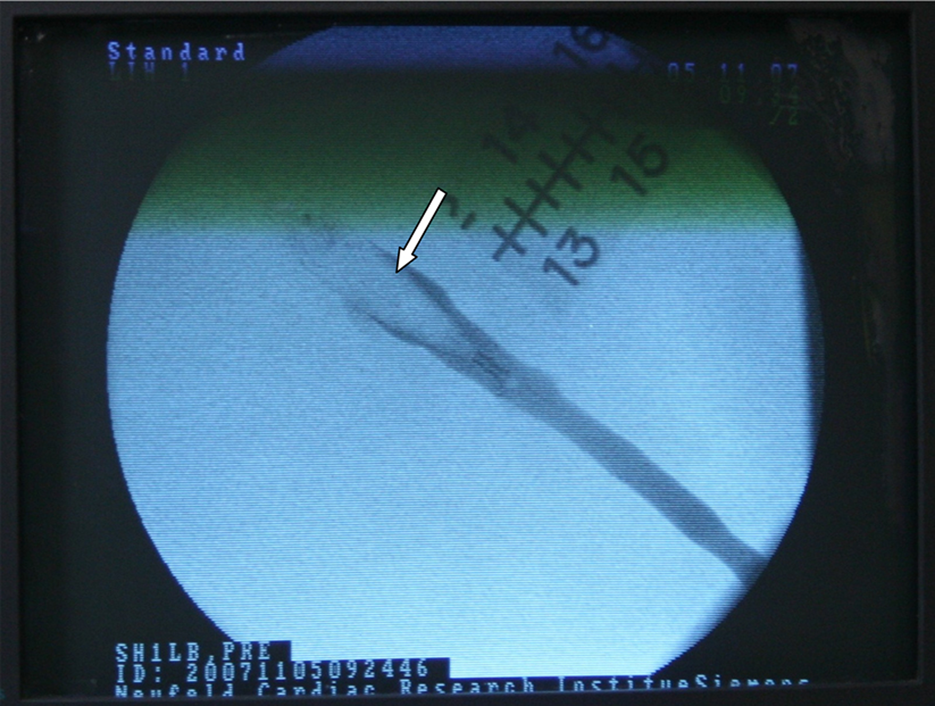
The V-block device was successfully delivered into the proximal GSV of all 12 animals. All devices were well visualized by duplex ultrasound and positioned 1–2 cm distal to the saphenofemoral junction (Figures 2a and b). There was no access or systemic periprocedural complications observed. After implantation, Doppler flow could not be detected in the GSV at the implantation site (Figure 2b) and distal to the device in all sheep. Contrast venography confirmed the absence of flow across the device (Figure 3).
Duplex ultrasound of the V-block device in the proximal saphenous vein. (a) A longitudinal view demonstrates the position of the V-block (arrow) is in the proximal great saphenous vein. (b) A transverse view shows the device (arrow) and no surrounding flow Contrast venography reveals the absence of contrast flow across the fully deployed V-block device (arrow) positioned in the proximal great saphenous vein
One sheep was sacrificed immediately postprocedure. The V-block device was firmly lodged within its GSV. Dilation of the vein wall at the implantation site as well as thrombus within the device was observed on histopathological analysis.
Duplex evaluation of animals at 12-day follow-up revealed that two of the 11 sheep had some flow in the GSV around the device. On subsequent evaluation at 30, 60 and 90 days these animals demonstrated no flow in the GSV. The control animal treated with vein ligation, likewise, had no flow detected in the GSV on follow-up. The V-block device was positioned in the proximal GSV without evidence of migration, tilting, perforation or fracture in all surviving animals at all follow-up time points. The mean diameter of the GSV at the implantation site increased from 4.95 mm before V-block deployment to 6.48 mm prior to sacrifice. Throughout the study, all sheep sustained normal vital signs and no adverse events occurred.
Pathological examination of vein samples collected on postoperative days 30, 60 and 90 from animals treated with V-block and V-block and sclerotherapy demonstrated obliteration of the venous lumen in all animals. A fibrous membrane was present over the proximal tip of the device in 10 out of 11 animals. Diffuse fibrous adhesions were noted, along the length of the V-block device that extended between the inner aspect of the venous wall and the outer aspect of the device (Figure 4). Material consistent with a chronic thrombus was present within the device filter.
Representative macroscopic findings from a sheep on postoperative day 60. (a) Specimen of proximal great saphenous vein containing V-block. (b) The specimen following longitudinal sectioning. The arrow points to fibrous tissue continuous with and covering the proximal tip of the device. Diffuse fibrous adhesions are present between the inner aspect of the vein and the outer aspect of the device. (c) The specimen following separation of the device. The arrow points to the fibrous tissue which covered the proximal end of the device. The inner aspect of the vein is rough due to the presence fibrous adhesions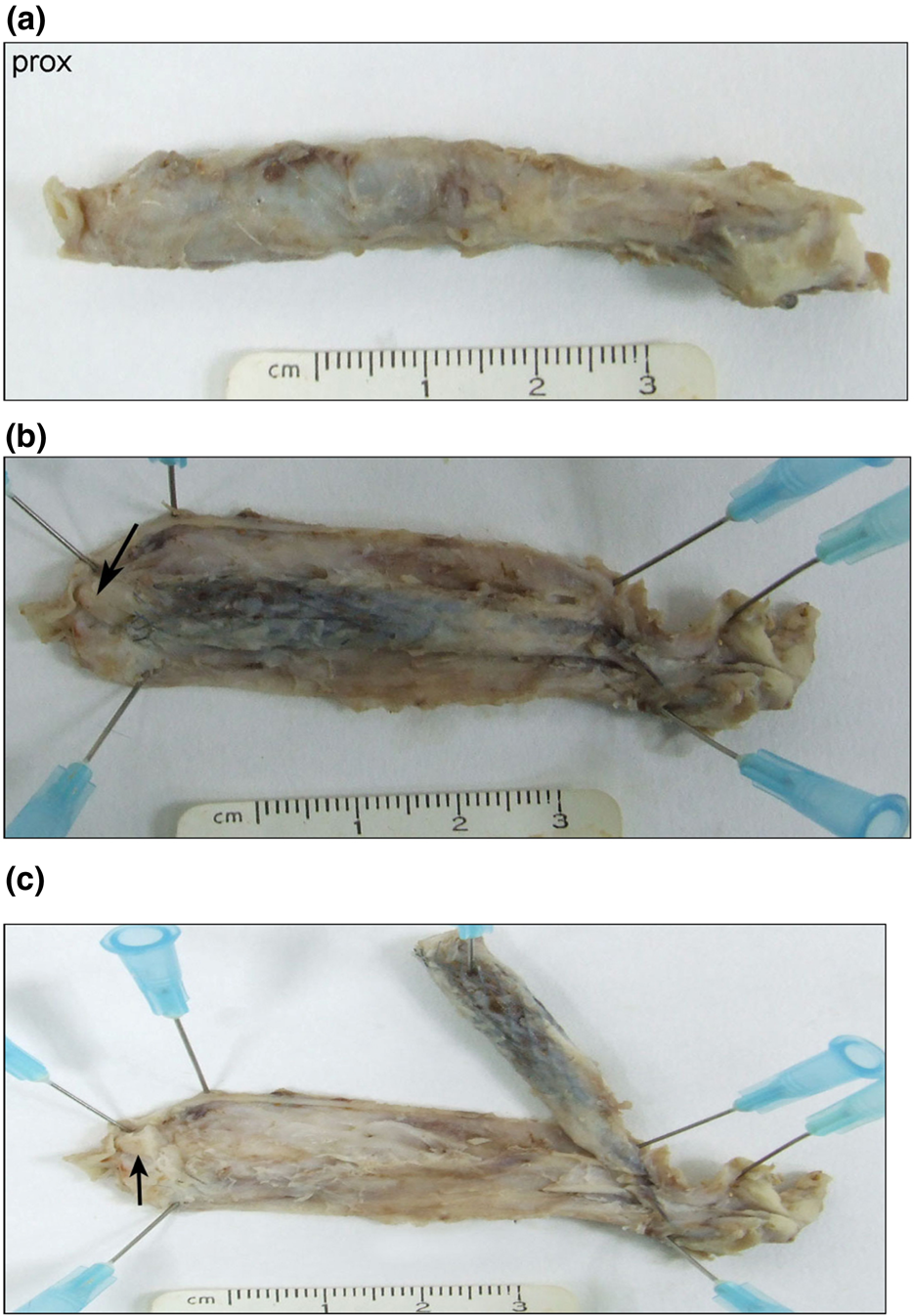
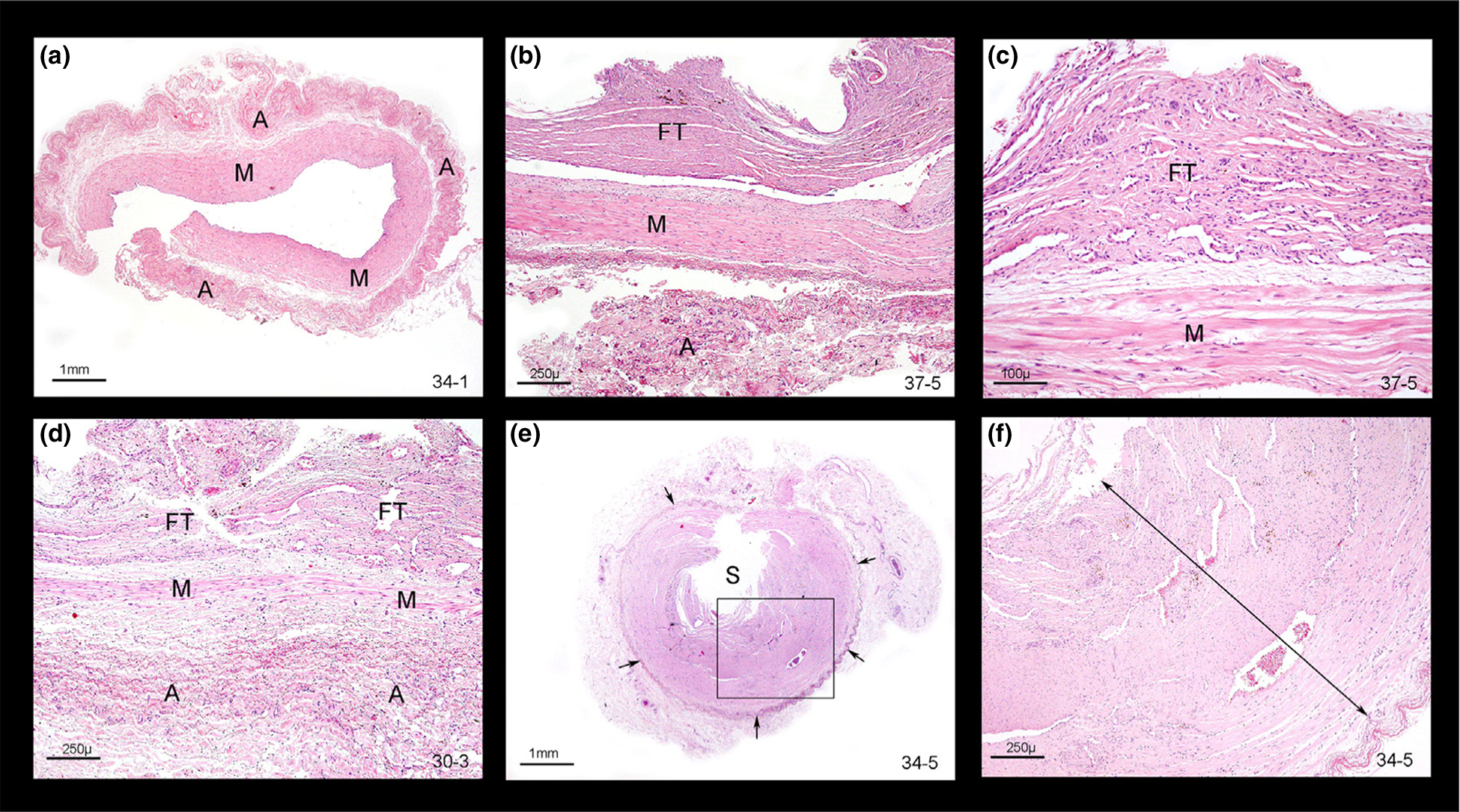
Histopathological analysis of GSV harvested from animals at day 30 of follow-up revealed widespread loss of intima, multifocal loss of medial smooth muscle cells and moderate medial fibrosis (Figure 5). Significant progression of fibrosis was noted in samples harvested on postoperative day 60 (data not shown). Vein samples obtained from animals on postoperative day 90 showed extensive fibrous replacement of the media and in one out of four samples medial smooth muscle cells could not be identified (Figure 6). Macroscopic and microscopic evaluation of harvested lungs showed no evidence of thromboembolism.
Representative microscopic findings on postoperative day 30 (haematoxylin and eosin staining). (a) A transverse section of the open vein at the level of the mesh part of the device. There is stretching of the venous wall seen as attenuation of the width of the adventitia (asterisks) and media (M). Fibrous tissue (FT) is present within the lumen and is connected in one area to the venous wall (arrow). The boxed area is shown in (b). The stretched adventitia (asterisks) is at the bottom left of the field. Internal to it is the M showing stretching and multifocal replacement by FT. The arrows point to several stretched smooth muscle cells. FT of moderate cellularity is attached to the fibrotic M. (c) This field is the other end of the same sample shown in (a, b). As above, there is marked stretching of the adventitia (asterisk) and M. In the lumen there is a thrombus with a wide attachment to the venous wall. The thrombus is composed of fibrino-haemorrhagic material (FIB) internally and FT peripherally. On its innermost aspect there are regularly spaced depressions (arrowheads) caused by compression against the mesh. The boxed area is shown in (d) (the plane of section is oblique in the top right corner). (d) At higher magnification the internal laminar arrangement of the fibrin (FIB) is apparent. This indicates that this material is in the earliest stages of thrombus formation. Thrombus maturation proceeds centripetally. Thus, the most peripheral part of the thrombus at the bottom left corner has the lowest cellularity (seen as blue dots at this magnification) and is the most mature. (e) A transverse section of the open vein approximately at the level of the joint between the mesh and the anchoring hooks. The venous wall is stretched. The most notable change is the presence of FT (light pink staining fibrous material) within the M where it surrounds and separates bundles of smooth muscle cells (arrows). The intima is lost in most sections, although it appears to be present in this sample to the right of the arrowhead. The adventitia is identified with asterisks. (f) A transverse section of the open vein at the level of the anchoring hooks. The adventitia is identified (arrowheads). Internal to it is the M. Both layers show pronounced stretching and there is partial fibrous replacement of the M (barely seen at this magnification). The venous lumen is occupied by a thrombus predominantly composed of FIB. The thrombus is attached to the venous wall at two opposite points via FT. Arrows point to two small spaces near the points of attachment which are consistent with spaces produced by the anchoring hooks Representative microscopic findings on postoperative day 90 (haematoxylin and eosin histological staining). (a) Low magnification of a transverse section of the open vein less than 1 cm cranial to the device. The vein is normal. The media (M) and adventitia (A) are identified. The intima is difficult to discern at this magnification. (b) A transverse sample of the open vein in the area of the mesh part of the device. The A is at the bottom. The M is markedly stretched. On the inner aspect of the M there is widespread proliferation of fibrous tissue (FT) which corresponds to the macroscopic adhesions. In this sample the FT is apposed to but not directly attached to the M. (c) Another field from the sample shown in the panel b. In this area the FT is attached to the underlying M. (d) A transverse sample of the open vein in the area of the mesh part of the device from another vein. The histological findings are similar to (b, c). The A is at the bottom. The M is markedly stretched and has undergone extensive fibrosis. It is diffusely continuous with adhesions composed of FT. In other areas in this sample the M could no longer be identified. (e) Low magnification view of a transverse section of the open vein at the level of the distal mesh/crimp. The original vein is identified by the presence of the A (arrows). The M is not identified. The lumen is occluded by a thrombus. At the centre of the thrombus there is a space (S) from where the device was removed. The boxed area is shown in (f). Internal to the A, seen as red fibres in the bottom right corner, the tissue (double headed arrow) is composed spindle cells (i.e. FT, possibly with some residual smooth muscle cells from the M). The latter are difficult to identify in this stain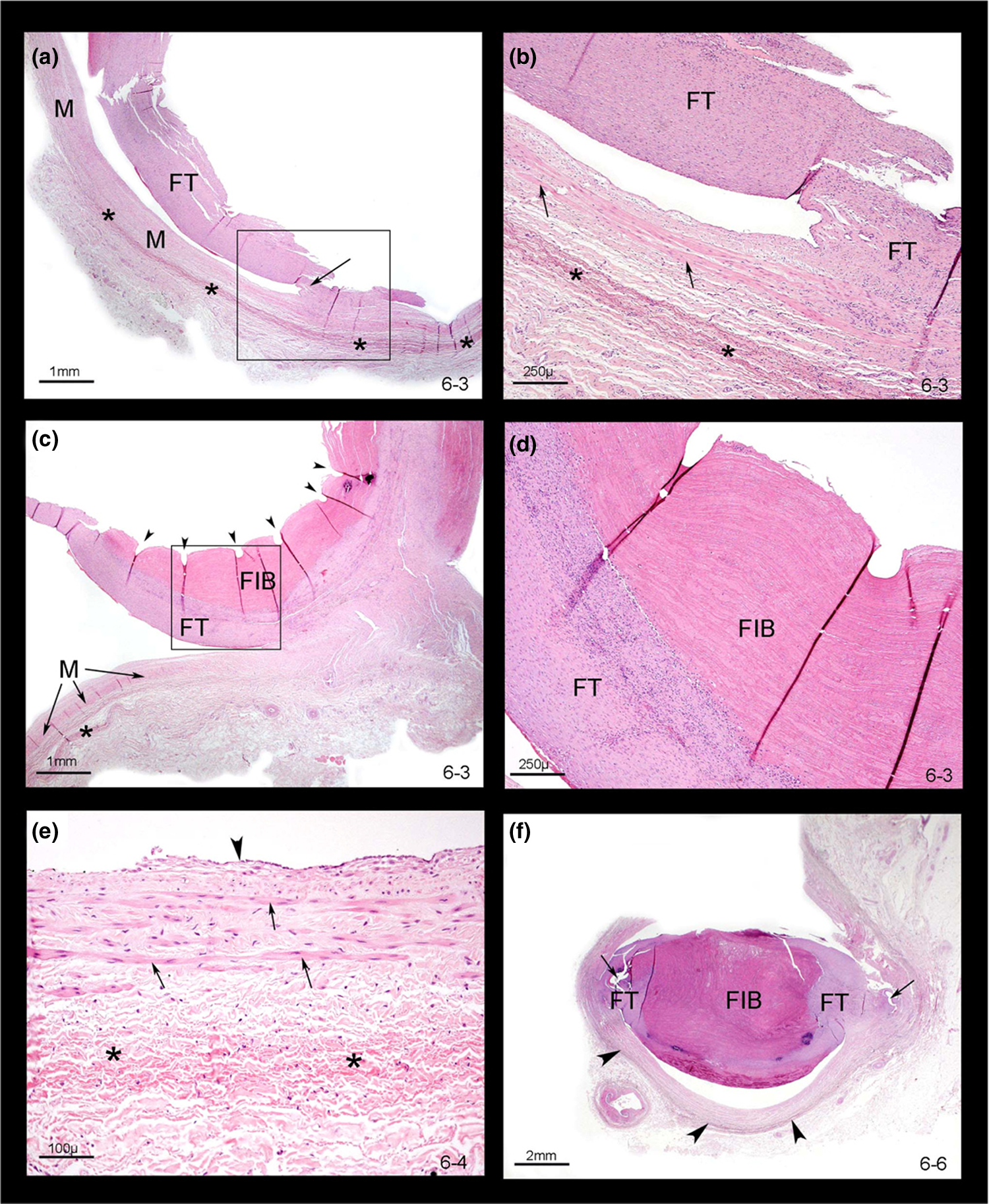
Discussion
The treatment of GSV incompetence has been a cornerstone for management of symptomatic CVD given that 70–80% of patients with CVD have reflux in the GSV. 14 We have developed a novel procedure to treat GSV reflux and report initial data on its use in an animal model. This procedure involves the percutaneous deployment of V-block, a novel occlusion device. This device has some similarities with other occlusion devices, which have been successfully used in the arterial system. 15 Upon deployment into the proximal GSV V-block is secured by the combination of radial force and anchoring hooks and, thereby, it is similar to some vena cava filters which have comparable characteristics. 16 The delivery system allows for injection of a liquid sclerosant through the Dual Procedure Syringe System in tandem with withdrawal of blood from the vein. This technique optimizes the contact between the sclerosant and vein wall which allows for successful vein ablation.
Our initial animal experiments have demonstrated that V-block can be safely and successfully deployed into the proximal GSV. V-block can be readily visualized using duplex ultrasound during deployment and in follow-up. During up to 90-day follow-up, the sheep did not experience any complications and there was no evidence of device migration or fracture. Although flow around the device was observed at 12-day follow-up in two of 11 animals, this finding was transient. Histopathological analysis showed significant fibrous incorporation of the device into the sheep saphenous vein. Furthermore, luminal obliteration associated with endothelial loss and replacement by fibrous tissue was noted. These changes are similar to ones observed in varicose veins after conventional sclerotherapy. 7
A number of techniques to treat GSV incompetence have been utilized including GSV high ligation and stripping, endovenous thermal ablation using radiofrequency or laser, and chemical ablation using foam sclerotherapy. High ligation and stripping of the GSV has been shown to be efficacious in multiple clinical trials.17–20 However, it is associated with a significant complication and prolonged recuperation rates. In one study, this procedure has been associated with a 19.4%, 33.3% and 5.6% echymosis, haematoma and paraesthesia rates, respectively. The average number of postoperative days to return to work was 12.4. 10 Others reported wound complications, nerve injury and thromboembolic complications to be as high as 16%, 39% and 5%, respectively. 7 Because of these findings and emergence of endovenous techniques, the indication for high ligation and stripping of the GSV has become limited to patients with superficial, aneurismal or very tortuous veins.
Endovenous thermal ablation is a minimally invasive procedure that is performed under ultrasound guidance, requires tumescent anaesthesia and can be executed in an outpatient setting. It includes radiofrequency ablation (RFA) and endovenous laser ablation (EVLA) and involves a percutaneous introduction of a RFA catheter or EVLA fibre, which causes direct thermal injury to the vein resulting in endothelial destruction, medial collagen denaturation and fibrothrombotic occlusion of the vein. 7 RFA, in a large prospective registry, has been shown to have a five-year 87.2% saphenous occlusion rate and >70% relief from clinical symptoms. 8 However, paraesthesias, thrombophlebitis, echymosis and skin pigmentation have been reported in 3.2%, 0.8%, 6.3% and 2%, respectively. 8 EVLA has been shown to have an 88–100% saphenous occlusion rate and significant short-term symptomatic benefits. 21 However, in one EVLA registry 75%, 3%, 1.9% and 0.5% of patients experienced bruising, paraesthesias, thrombophlebitis and skin burns, respectively. 22 Although, both RFA and EVLA are associated with faster recovery compared with high ligation and striping, the mean return to work time has been published to be 6.5 23 and 4–2024,25 days, respectively.
Finally, endovenous chemical ablation involves the introduction of sclerosant foam into the GSV and consequent ipsilateral leg elevation to limit the introduction of the foam into the systemic circulation. Foam sclerotherapy of the GSV has been associated with an 80% saphenous occlusion rate at 4–6 years of follow-up. 26 Despite these results, complications such as visual disturbances, migraine-like headache, confusion and stroke have been described.27,28 These symptoms likely relate to the persistence of foam particles in the circulation.
V-block with associated liquid sclerotherapy promises multiple advantages over the currently available GSV treatment options. This procedure can be performed in an outpatient environment, does not require tumescent anaesthesia and allows for use of a liquid sclerosant which due to dilution has a short circulatory half-life. It promises to eliminate the risk of skin burns and nerve injury associated with thermal ablation methods. Also, it obviates the need for capital investment required with use of thermal ablation techniques and thereby may be more cost-effective.
Conclusion
We deployed and tested the V-block device in an animal model. In this pilot study, we have demonstrated it to be safe and efficacious for treatment of GSV incompetence. This device led to successful ablation of GSV in our animal model as evidenced by both duplex ultrasound and histopathological findings. This device promises to provide a novel way to treat GSV incompetence and clinical trials are currently under way.