
Abstract
Objective:
To assess the patterns of referral for chronic venous disease (CVD).
Method:
General practitioners (GPs) were invited by an email to complete a validated online survey evaluating the referral and community management of CVD.
Results:
A total of 138 participants were recruited. Most GPs (85%) saw fewer than 50 patients with CVD a year. Thirty-one percent were aware of National Institute for Clinical Excellence referral guidelines for CVD and 36% were aware of and agreed with local referral guidelines. Eleven percent were aware of clinical venous scoring systems. Sixty-three percent believed mild CVD would progress and 84% believed treatment would improve the quality of life. Sixteen referred C3 disease, 43% C4, 37% C5 and 65% C6 disease. Forty-one percent would refer on request. Pain symptoms increased referral in C2 disease. Endothermal ablation was believed available to 33% and traditional stripping to 62% and 27% were unaware of the treatment options. Forty-five percent were happy to provide postoperative care.
Conclusions:
Despite national guidelines, the management of CVD in the UK is variable.
Introduction
Chronic venous disease (CVD) is extremely common, affecting 25–50% of the population.1–3 It is associated with a high level of morbidity and socioeconomic cost, and accounts for 2% of the National Health Service (NHS) budget per year. 4 Ulceration is the endpoint of venous disease and alone consumes 1% of the NHS budget. Varicose vein intervention is common and over 37,000 treatments are performed each year in the NHS. 5
Symptoms from varicose veins can vary widely; however, significant swelling, prominent varicosities, itching and pain are common. 6 The treatment of varicose veins has advanced considerably in the past 15years with the advent of endovenous ablation, regional or local anaesthetic for open surgery and an increased interest in foam sclerotherapy.7, 8–10 Extensive work has shown the cost-effective nature of intervention11, 12 and a poor compliance of patients with stockings, which ranges between 18% and 25%.13, 14 Minimally invasive treatments now can provide large quality of life improvements at a low cost.7, 11
General practitioners (GPs) are the gatekeepers to secondary care in the UK. Standard GP training, however, does not include any formal teaching on CVD and GPs have variable exposure to the surgical specialties during their medical training. 15 GP trainees do though undergo an extensive apprentice-ship with GP trainers and will cover such topics during this period. Interestingly, work by Chassany et al. 16 demonstrated the disparity between patient-reported and GP-reported symptom severity with GPs routinely reporting lower levels of pain and quality-of-life impairment compared with patients. Conway et al. 17 have also shown that patient reported symptoms are unreliable compared with standardized questionnaires due to the subjectivity of symptoms.
In order to aid GPs in the management and referral of CVD, extensive guidelines have been developed in the UK by the National Institute for Clinical Excellence (NICE) 18 and more recently by the Royal Society of Medicine's Venous Forum. 19 In the USA, guidelines on management of CVD patients have also been created. 20 In order to stratify CVD, various clinical scoring systems have also been developed and validated, such as VCSS (Venous Clinical Severity Score).21, 22 Despite the existence of guidelines and scoring systems, the treatment of varicose veins has been classified and is viewed of low clinical value, 23 leading to the creation of disparate and confusing local guidelines and these are often in contention with national guidelines.
GPs are now also expected to perform routine postoperative follow-up for surgical procedures, such as varicose veins and hernia repairs, 24 without appropriate remuneration or support. Previous work 25 surveying patients, GPs and surgeons after postoperative outpatient attendance found that in the context of benign general surgical disease, 95% of patients found follow-up specialist consultations useful, and only 49% would prefer to see their GP. Importantly, management was changed by the specialist in 44% of cases. Preference for specialty follow-up was mirrored in a similar study by Frew et al. 26 in cancer patients.
The aim of this study was to assess patterns of referral and the management of CVD in primary care in the UK.
Methods
Following ethical review and categorization as service evaluation by the local ethical subcommittee, a 23-question electronic survey was created which assessed different aspects of CVD management and treatment pathways. The questionnaire was tested and validated for content and construct by GPs and vascular surgeons, with internal, external and independent assessors as previously described by other authors. 27 In England there are approximately 34,101 GPs. Invitations to complete the survey were sent via email to an estimated 300 GPs throughout England (http://kwiksurveys.com?u=gpvaricoseveins), at random using local and national mailing lists. Please see Appendix 1 for the complete survey. Responses were collated by the survey server (KwikSurveys, Dover, UK) over a six-month period and results were analysed using Microsoft Excel 2011 (Microsoft Corporation, Redmond, WA, USA) and GraphPad Prism (Graph-Pad Software Inc., La Jolla, CA, USA) software.
Results
A total of 138 completed responses were received, representing a response rate of 46%. All received surveys were analysed and none were excluded.
Cases seen
The vast majority of GPs (85%, P < 0.001) stated that they saw less than 50 patients with varicose veins per annum, which is an average of less than one per week. Seventy-eight percent managed CVD patients conservatively in the community, with one providing treatment with sclerotherapy. If specialist care was required most GPs (78%, P < 0.001) referred to a vascular surgeon, 10% to a general surgeon and 11% to a vascular nurse specialist.
Reasons for referral
In all, 40% of GPs would refer a patient at their request and 10% for cosmesis, 43% for venous skin changes and 58% for pain (see Figure 1).
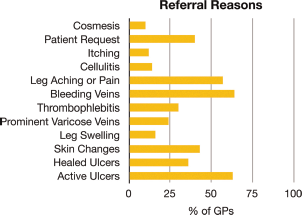
Reasons for referral from primary care (% of GPs). GP, general practitioner
Available treatments
Figure 2 demonstrates which treatments GPs believe are available to their patients. Thirty-three percent believed that endovenous treatments were available in their locality, but a surprisingly low figure of 60% believed traditional open surgery to be available as a treatment option, despite its usually universal availability (P < 0.001).

Interventions believed available (% of GPs). GP, general practitioner; RFA, radiofrequency ablation; EVLA, endovenous laser ablation
Guidelines and scoring systems
Only one-third of GPs (31% versus 69%, P < 0.001) were aware of the NICE Referral Guidelines (published in 2001) for CVD. Sixty-one percent were aware of local Primary Care Trust (PCT) referral guidelines, but only 36% agreed with these guidelines. Twenty-six percent of GPs said that they were aware of NICE Treatment Guidelines; however, these guidelines do not actually exist. Local PCT guidelines do exist and 41% of GPs were aware of these, although again only 26% agreed with them. Eleven percent were aware of clinical scoring systems and 89% were not (P, 0.001).
How to manage CVD
Overall, for patients with varicose veins, 62% of all treatment was conservative with reassurance (15%), compression hosiery (38%) or compression bandaging (10%). Twenty-nine percent of patients would be referred to a specialist and 8% would undergo further investigation prior to referral. One GP would treat varicose veins with sclerotherapy in the community. Fifty-three percent of GPs would refer active ulceration (C6), and 41% venous skin changes (C4). Pain symptoms would increase the referral rate for CEAP (clinical, aetiological, anatomical and pathological elements) clinical stage C2 disease from 2% to 24% (P < 0.001) and from 20% to 55% for C3 disease (P < 0.001). Pain is not a discriminator in national guidelines.
Role of intervention
Figure 3 illustrates how GPs determined whether there was a role for intervention using sample cases. Pain appeared to be the most important factor in this decision with 16% agreeing that CEAP class C2a (asymptomatic) warranted intervention but with pain (C2s) the referral rate increased to 71% (P < 0.001). In patients with leg swelling and varicose veins (C3), 42% of GPs felt that pain-free patients should have treatment compared with 83% if patients also had pain (P < 0.001). Interestingly, only 62% of GPs believed that venous skin changes warranted intervention. Moreover, only 78% believed venous ulceration required intervention compared with 8% who did not and 14% were unsure (P < 0.005).
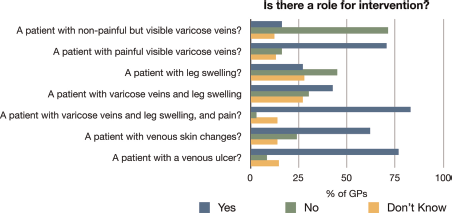
Role of intervention in example cases (% of GPs). GP, general practitioner
Progression, quality of life and cost-effectiveness
Sixty-four percent of GPs believed that mild CVD would progress to severe disease, compared with 36% who did not (P < 0.001). Eighty-four percent of GPs thought that treating varicose veins would improve a patient's quality of life, and only 26% felt that it was not a cost-effective use of NHS resources. The majority (75%) believed that CVD for the purpose of improving quality of life could be managed conservatively.
Free of charge treatment
Figure 4 shows which treatments GPs felt should be provided free of charge on the NHS. Interestingly 11% of GPs believed that CEAP class C2a (visible but asymptomatic veins) should be treated free of charge and 8% were unsure. As CEAP class increased the proportion favouring free treatment also increased. Once again the onset of pain vastly increased the favour for free treatment.

Should treatment be free of charge on the NHS? (% of GPs). GP, general practitioner; NHS, National Health Service
Follow-up and ‘Me Too'?
Forty-five percent of GPs were happy to provide aftercare for varicose vein intervention, and 8% felt that no follow-up was required.
In the ‘Me Too’ question, 71% of GPs stated they would like invasive treatment if they have varicose veins, with none wanting traditional open surgery.
Discussion
The management of CVD is a common scenario encountered in general practice. The important aim of treatment is to avoid ulceration. From our results, it is evident that there is no clear consensus on the management of CVD in the community. While the majority of patients are no doubt treated appropriately, there is a reticence of primary care fund holders to allow referral for invasive treatment and consequently the burden of disease remains widespread. From our study, the treatment options also appear not to be universally available and in addition, there is patchy GP awareness of their availability.
Interestingly, GPs saw relatively few patients with CVD – with a 25–50% prevalence the average GP practice should have 1600–3200 patients with the condition. 28 This is likely due to a combination of public and medical ignorance of the benefits of treatment.
What has become clear from this survey is that the CVD knowledge base of GPs is limited due to both a lack of exposure to the condition in their training and recent treatment progress. The number of GPs unaware of classification criteria, local and national guidelines, and the treatment options available demonstrates this. A substantial portion of GPs were also unsure of the benefits of treatment on a patient's quality of life (11%), disease progression (23%) or on cost-effectiveness of treatment (34%), despite extensive literature published on these areas in the last two decades. Our results would also suggest that follow-up should be with the treating physicians, and 92% of GPs felt that this was required, with only 45% were happy to provide postoperative care themselves.
National advice for referral for patients with CVD recommends referral to a specialist if there is quality-of-life detriment from prominent varicosities, not for cosmetic reasons or pain specifically. A key finding of the study is that pain is the main discriminator for patients being referred to secondary care. While this is unsurprising, as patients will not attend without symptoms, our study also demonstrates that only about one third of GPs were aware of the NICE Referral Guidelines and that among them only about one-third agreed with these guidelines. Crucially, 71% of GPs felt that C2 disease with pain (prominent varicose veins) should have intervention compared with 63% (NS) who thought that venous skin changes warranted treatment. This is concerning as the treatment of C4 disease is vital in the prevention of venous ulceration. Moreover, CVD intervention is far quicker and cheaper than ulcer treatment.
In an era of austerity and primary and secondary care commissioning, there must be improved discourse between venous specialists and primary care physicians. This must include mutual education sessions in order to disseminate recent advances. Surgical exposure in GP training is limited and topics such as venous disease are taught during an 18-month mentorship with GP trainers. It would therefore be prudent to encourage careful updating of these experienced GP trainers by the specialists to whom they refer.
This study is limited by two main factors – numbers and participants. There are approximately 34,101 GPs in England. It was not feasible to contact all GPs and therefore a representative sample of approximately 300 GPs was sought. The study additionally suffers from responder-bias, as those GPs willing to respond to the study are likely to be more engaged with local PCTs and commissioning services. They are also more likely to keep abreast of current treatments. Despite this the disparity between guidelines and practice was significant.
Conclusion
Despite clear national guidance and advice, referral and treatment patterns are extremely heterogeneous. This is the driving force behind the formulation of the various guidance documents available. CVD education is also lacking from GP training programmes despite CVD being a common condition, and venous specialists should aim to aid the lifelong learning needs for new and mature GP colleagues. For the benefit of our patients improved communication with GPs will lead to better patient care. We suggest that this should be sought at a local level with the development of clearer lines of feedback between primary and secondary care.
Footnotes
Acknowledgements
None.