
Abstract
Objectives:
To investigate the effectiveness of bipolar radiofrequency-induced thermal therapy (RFITT) in a multicentre non-randomized study.
Methods:
Some 672 incompetent saphenous veins (85% great saphenous varicose vein, 15% short saphenous vein) in 462 patients (56.5% CEAP [clinical, aetiological, anatomical and pathological elements] class 3 or worse) were treated in eight European centres. Patients were assessed between 180 and 360 days postoperatively. Occlusion rates were determined by duplex ultrasound and compared with the power used for treatment, pull back rate and experience of the operating surgeon.
Results:
Complete occlusion rates of 98.4% were achieved when treatments were performed by an experienced operator (more than 20 cases), when the maximum power setting on the RFITT generator was between 18 and 20 Wand the applicator was withdrawn at a rate slower than 1.5 second/cm
Conclusions:
RFITT is efficacious, well tolerated by patients and has a low incidence of procedure-related post-operative complications.
Introduction
Treatment of great saphenous varicose veins (GSV) has traditionally involved surgery with an incision at the groin and stripping of the GSV. This method can cause significant postoperative pain and bruising and delayed return to normal activity.1,2 Complications include infection, haematoma and saphenous nerve injury.3–5
Less invasive endovenous techniques have been shown to be as effective as surgery in the treatment of varicose veins. They also produce less post-operative pain and bruising and enable early return to normal activity.2,6–9 Some endovenous techniques use thermal energy to cause vein ablation: endovenous laser ablation (EVLA), radiofrequency ablation (RFA) and steam treatment. All three techniques use a catheter to deliver thermal energy to the vein wall to cause venous occlusion. Early reports suggest that there appear to be differences in effectiveness and postoperative pain and bruising with RFA having slightly lower occlusion rates but causing less pain and bruising than EVLA.6–8 There is currently little data on steam ablation.
While there are several manufacturers and wavelengths for EVLA there has only been one system for RFA. The early catheter systems used resistive heating of the vein wall to cause ablation (Closure Plus, VNUS Medical Technologies, San Jose, CA, USA). These systems were reported to produce longer treatment times when compared with EVLA. More recently segmental ablation catheters have been used which use conductive heating of the vein using radiofrequency energy to heat a 7-cm coil (VNUS Closure Fast, VNUS Medical Technologies). For segmental ablation, as with EVLA, tumescence anaesthesia or fluid is required to reduce pain and thermal damage to surrounding tissues and to compress the vein wall onto the catheter.
A minimally invasive bipolar radiofrequency-induced thermotherapy (RFITT) technique (Olympus-Surgical Technologies Europe/Celon AG, Teltow, Germany) is widely used for minimally invasive surgery for tumour ablation and palatal ablation.9–14 This RFA system has the capacity to treat truncal varicose veins with and without tumescence. 15
The aim of the study was to investigate the effectiveness of RFITT for endoluminal treatment of varicose veins.
Methods
Eight institutions in Germany, The Netherlands, UK, Italy, Croatia, Czech Republic and Spain took part. The recruitment of patients occurred during a 45-month period between March 2005 and December 2008.
Patients aged 18 years and above with varicosities of the GSV or short saphenous veins (SSV) were eligible for inclusion. All patients had symptomatic varicose veins with a CEAP (clinical, aetiological, anatomical and pathological elements) class 1–6. 16 Patients with deep vein thrombosis, fresh thrombus in the vein to be treated, symptomatic peripheral arterial disease, severe systemic diseases, extremely convoluted saphenous veins (that might prevent insertion of the applicator) as well as lactating mothers or pregnant women were excluded. Patients had a preoperative duplex scan confirming incompetence of the GSV or SSV and venous morphology suitable for RFA. The venous morphology was similar to that required for EVLA or segmental RF Ablation. Veins up to 12 mm in diameter on duplex examination were included.
The RFITT system was used for all treatments and comprised the bipolar CelonLab Precision radiofrequency power control unit with foot switch and a flexible bipolar RFITT applicator Celon ProCurve 1200 (Olympus Surgical Technologies Europe/Celon AG, Teltow, Germany). The bipolar arrangement of electrodes of the applicator enabled a resistive heating of the vein wall to cause ablation and closure of vein. The impedance of the venous tissue was continuously monitored and indicated by an acoustic signal (impedance feedback) on the power control unit allowing even distribution of energy to the vein wall. This system also allowed the withdrawal speed of the catheter to be altered by the operator depending on the amount of energy required. The applicator catheter was echo-genic and easily seen on duplex scanning where the two electrodes produced visible acoustic shadows.
After a period of training in the technique and approval from the relevant ethics or clinical governance committees, each investigator was asked to evaluate the RFITT system. There was a variation in the methods for inserting the RFITT catheter and in the use of adjunctive procedures to treat varicosities. Prior to the training for this study, three investigators had experience of endovenous thermal ablation techniques while the remainder had not used either EVLA or RFA prior to their training for this study.
Procedures were performed under general, regional or local anaesthesia according to local practice. Target veins were cannulated by one of two methods: either a 5 F or 6 F sheath was placed at the distal point of incompetence of the vein under duplex ultrasound guidance using the Seldinger method and the flexible RFITT applicator was then passed through the sheath. Alternatively, the applicator catheter was passed directly into the vein via a cut down without the use of a sheath. Once the applicator was in the vein, it was passed proximally to lie in a position 1–2 cm inferior to the saphenofemoral or saphenopopliteal junction. The applicator had a rounded tip to minimize the risk of perforating the venous wall on correct use.
In some patients fluid (tumescence) was injected into the perivenous sheath in a similar fashion to that used for EVLA or segmental RFA. In some cases, no fluid was injected and the leg was elevated and treatment commenced. In others, there were no injections but an Esmarch bandage was used to compress the vein on to the applicator prior to treatment, http://www.complete-feet.co.uk/minor-surgery/sterile-esmarch-bandage
The power output of the applicator was activated by a foot switch via the power control unit. The maximum output power was selected by the investigator at their discretion and preference: Settings between 18 and 25 W were used during the course of the study. Activation of the foot switch triggered the release of radiofrequency energy as the applicator was slowly pulled back under control of the audible impedance feedback. If coagulum collected on the applicator tip, the applicator was removed, cleaned and re-inserted and the treatment recommenced.
Adjunctive procedures such as phlebectomies or sclerotherapy were performed as necessary. Postoperative care was carried out according to local policy but typically utilized a 15-cm crepe bandage worn for one day followed by a light compression stocking worn for two weeks. Patients were discharged the same day on recovery from anaesthesia and successful ambulation. Analgesia in the form of non-steroidal anti-inflammatory medication was prescribed as necessary.
Follow-up investigations
Patients were asked to complete visual analogue scores (VAS) for their perception of pain on days 1, 7 and 21. Clinical and postoperative duplex follow-up was done after six and 12 months. Duplex ultrasonography of the treated veins was carried out to determine treatment success as defined by:
Complete ablation (closed) was defined as no flow seen throughout the entire treated length of vein;
Partial ablation (partial) was defined as no flow seen in part of the treated length of vein but some areas were still compressible and had flow. In this category the preoperative truncal reflux had been abolished but the whole length of the intended treatment zone had not occluded;
Failed ablation (open) was any vein that had truncal flow throughout the intended treatment zone. This included patients where the vein had narrowed and where the reflux was of a shorter duration than had been detected on the preoperative duplex scan.
The incidence of haematoma, pigmentation and other skin changes as reported by the patient or clinician were recorded. Patients were asked to provide subjective assessment of their symptoms and any complications were recorded (e.g. sensory disturbances). Patients were asked to state their satisfaction with the procedure.
Data collection and analysis
Each investigator provided data using a standardized sheet which was sent to a central data collection centre. In addition to patient reported outcomes, data included gender, age, treated saphenous vein, CEAP classification (CI–6), method of anaesthesia, use of tumescence, selected maximum output power, length of treated vein segment, total time of energy application, and occlusion status documented by duplex scan.
Data management and statistical analysis were performed by professionals independent of the investigators and the manufacturer of the RFITT system.
Data were analysed for patients who had a final follow-up between 180 and 360 days after treatment. The treatment time per centimetre and power used were calculated for each treatment. The outcome of treatment was compared with three factors in order to identify the conditions for the use of RFITT that resulted in the best occlusion rates: (1) pullback rate, (2) power setting and (3) experience of the operator.
Complications which were not related to the RFITT procedure were not analysed (e.g. side-effects of adjunctive procedures like phlebectomy or sclerotherapy).
The Fisher's exact test was used for statistical analysis of contingency tables instead of chi-squared test because the expected values in some of the cells of the analysed contingency tables were below 5. Because of multiple testing the Bonferroni criterion was used to adjust the level of significance: P = 0.05/4 = 0.0125. 17 The statistical test was performed by using SPSS 17.0 (SPSS Inc., Chicago, IL, USA).
Results
During the study period, 953 patients had 1400 incompetent truncal veins treated with RFITT (1172 GSV and 228 SSV). Of the 953 patients, 462 patients completed follow-up between 180 and 360 days. The remainder did not attend for medium term follow-up. The outcome data for the 462 patients who attended follow-up (569 GSV and 103 SSV) were analysed.
The majority of patients had symptoms classified as CEAP class 3 or worse (56.5%). Some 81.5% of patients had general anaesthesia. Seventy-three percent of patients had tumescence fluid injected. The use of additional tumescence decreased during the course of the study: while for the first half of treatments in the study additional tumescence was used in 85.4%, only 60.7% of treatments in the second half were combined with tumescence. The average generator output power was set to 23 ± 3 W. The mean length of vein treated was 50 ± 20 cm and the mean total treatment time was 89 ± 66 s which equates to a mean pullback rate of 1.8 ± 1.3 s/cm.
After a mean follow-up period of 290 ± 84 days, 621 veins (92.4%) were occluded, 30 (4.5%) were partially occluded and treatment failed in 21 (3.1%). The results for all patients are summarized in the left data column of Table 1 (all patients) and in the Kaplan-Meier graph (Figure 1).

Kaplan-Meier graph showing numbers at risk, cumulative complete occlusion and combined complete and partial occlusion rates over time for the whole cohort of veins treated with RFITT (n = 672). Complete or partial occlusion rates were 99.2% and 95.4% at 180 and 360 days (solid line). Complete Occlusion rates were 98.5% and 88.2% (dash line) at 180 and 360 days
Patient data for all patients group and for the optimum group

pt., patient; FU, follow-up
*All-patient group = patients with last follow-up between 180 and 360 days after treatment
†Optimum group = treatments selected by (1) pullback speed 1.5 cm/second or slower, (2) maximum power 20 W or lower, (3) experience of >20 treatments
‡Number (percentage)
§Mean ± standard deviation (minimum-maximum)
∗∗Number (mean number per pt.)
Complications
Complications occurred in 61 of 672 treatments (9.1%). The numbers and the rates of complications after procedure are shown in Table 2. The most frequent complication was sensory disturbance which occurred in 5.8% of patients but this resolved after a median of nine weeks. Other complications included bruising, erythema, haematoma, hyper-pigmentation, matting and phlebitis occurred with frequencies below 1% each. There were no DVTs and no thermal injuries.
Complications after the RFITT procedure
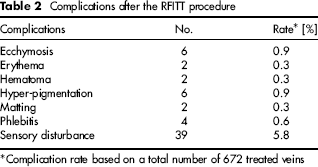
Complication rate based on a total number of 672 treated veins
Pain scores and patient satisfaction
The median VAS level for pain was 2/10 at one day of follow-up which decreased to 1 after seven days follow-up and was 0 at all subsequent follow-up visits of 21, 180 and 360 days. Some 99.3% of patients were satisfied with the therapeutic/cosmetic outcome of treatment. Likewise 99.6% would recommend the treatment method to others.
The effect of pullback rate
Figure 2 shows the effect of different pullback rate in cm/s on occlusion rates. Occlusion rates were significantly higher (P = 0.005) when pull back rates were slower than 1.5 s/cm when compared with faster pullback (Figure 3a).

Pull back time and occlusion rates
Power setting
Power settings of between 18 and 20 W produced complete occlusion in 95.3% of treatments compared with 91% when settings of greater than 20 W were used (Figure 3b). This difference was not statistically significant (P = 0.015).
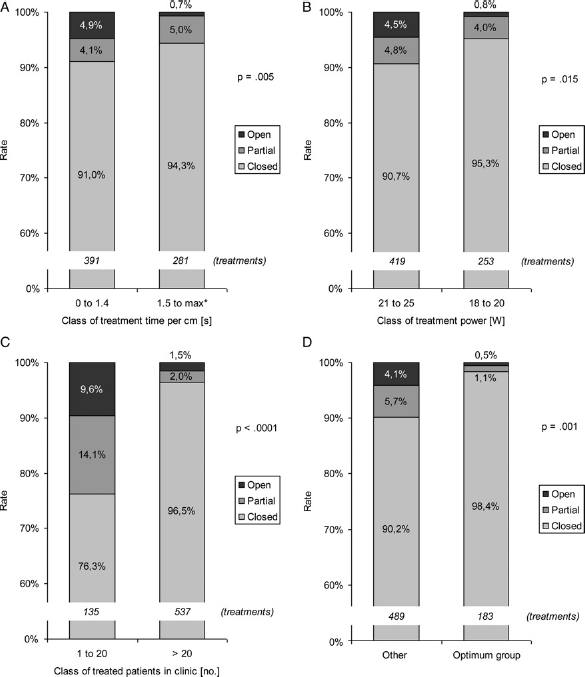
Rates of complete, partial and failed treatment by. (a) Pull back time in cm/s. (b) Treatment power, (c) Operator experience, (d) Optimum group (all class criteria of right bars from a-c applied) versus other patients (none, only one, or only two class criteria of right bars from a-c applied). Fisher's exact test was used for P values.
Influence of the learning curve
Operator experience influenced outcome. On average, for the first 20 veins treated, only 76.3% were completely occluded which was significantly lower (P < 0.0001) compared with 96.5% when more than 20 treatments had been performed by the operator (Figure 3c).
A subgroup analysis was done to identify those treatments where the operator was experienced (more than 20 cases), the power setting was 18–20 W, and the pull back time was slower than 1.5 s/cm. There were 183 treatments in this category (optimum group) and 98.4% of veins were completely occluded compared with 90.2% occlusion in the other 489 treatments when power and pull-back speeds were higher and experience less. This difference in outcome was both clinically and statistically significant (P = 0.001). This result is shown in Figure 3d.
Discussion
This study shows that RFITT is an effective method for treating truncal varicose veins under local or general anaesthetic. A 98.4% complete occlusion rate can be obtained when the operator has experience of at least 20 treatments, uses a power setting of between 18 and 20 W and pulls the applicator back at a speed of 1.5 s/cm or slower.
This was a large international study in countries with differing healthcare systems. The design included clinicians from different clinical centres, ranging from ambulatory offices through day surgery centres to hospitals. The multiple sources of data should minimize the impact of differences in clinical routine by individual surgeons, because of different experience and personal preferences. The results are therefore what other practitioners might expect if they chose to use the RFITT system.
It was not possible to follow up all patients because some were reluctant to return for appointments when they saw no need to do so. Nearly all patients were happy with the outcome of their vein surgery and would recommend it. It is accepted by the authors that some patients may not have returned for follow-up because their treatment had failed or they were unhappy with the outcome. This is unlikely as the presented results are comparable with the outcomes of other forms of endovenous thermal ablation.
It is important to understand what the difference is between RFITT, EVLA or VNUS ClosureFast in the way energy is delivered to the vein.
The thermal effect of RFITT results in a shrinkage and irreversible denaturation of collagen and other cellular proteins. The structure of collagen changes as its bonds break and it forms a gel-like substance that acts as glue between vessel walls. To achieve this effect the tissue needs to be heated to between 70 and 95 °C, sufficient for collagen and elastin in the tissue to convert into gelatin. 18 The thermal energy with RFITT is not, as is the case with the laser or VNUS ClosureFast, emitted by the catheter, but originates directly in the venous wall. This was how the original Closure plus system worked, albeit with longer pull-back times than with the RFITT system 19 The RFITT applicator itself is not actively heated and remains colder than the treated tissue. There is therefore a lower risk of inadvertent thermal injury. There were no thermal complications in this study. The bipolar arrangement of the electrodes of the RFITT applicator creates an effect comparable to an ‘induction cooker’, with the venous wall used as a conductor between the two poles. Radio-frequency energy can generate heat in biological tissues by causing high frequency oscillations of ions or water molecules. 12 In an ex vivo study with bovine veins heated in a water quench, it was shown that the greatest shrinking by 36% as well as the largest increase of wall thickness by 38% was found at temperatures of 85 and 90 °C.
Histological analyses of treated veins from rabbit ears and human veins obtained by stripping indicate that proteins of the venous endothelium are converted into gelatin and then cause occlusion of the venous walls. 18
The energy applied to the tissue is an adequate parameter to estimate the treatment effect, as the heat dissipation and therefore the temperature increase in the treated tissue region is proportional to the energy applied. An often used ratio is the so-called linear energy density, which is the applied energy (in Joule) per length of the treated vein (in centimetres). In laser treatments, a linear energy density of 60–90 J/cm, depending on the laser wavelength, is usually considered to result in sufficient occlusion rates while keeping complications at an acceptable level. 20
It is not appropriate to compare the energy used for RFITT and the energy used for EVLA. The ratio of linear energy density (J/cm), often quoted with EVLA, does not consider all physical aspects and is therefore only of limited suitability to predict treatment success. Energy dissipation is a three-dimensional effect, as heat is generated in the tissue volume surrounding the energy source, i.e. the tip of the catheter. The energy required to sufficiently heat a vein segment of a certain length depends, besides its length, on the diameter of the vein segment and the thickness of the vein wall. As a consequence, thicker vein segments require more energy than thinner ones to achieve a sufficient thermal effect. In the case of the RFITT system, the impedance control determines both the emitted power and the withdrawal speed of the catheter. The impedance, in turn, depends on the dehydration of the tissue surrounding the tip, which is related to the tissue temperature. Therefore, more energy is applied to segments in which more energy is required for a sufficient heating effect (e.g. bigger vein wall thickness), and less energy e.g. in thinner vein sections, leading to an appropriate J/cm3 value while the J/cm values will vary. As the vein diameters have not been recorded in this study, further research is required to evaluate this relationship.
Significantly better occlusion rates were achieved when a lower power setting (20 W) and a slower pull back rate was used 1.5 s/cm. This observation suggests that a lower power setting leads to a slower increase of tissue temperature; therefore, to a slower dehydration and a slower increase of impedance. As a consequence, the withdrawal speed needs to be lower. This again leads to a higher energy emission to the vein wall resulting in a more thorough vein wall protein denaturation. It is possible that power settings of less than 18 W could result in even better occlusion rates but those settings were not the subject of this study. Laboratory studies would be required to confirm these hypotheses.
The use of tumescence is not mandatory when using RFITT. Additional tumescence was used in 73% of all patients. Unlike ablation techniques using conductive heating or laser, involving temperatures of between 120 and 500 °C which make tumescent infiltration essential, the results suggest that patients can be treated with RFITT without the additional cost or time involved in injecting fluid. This is because the RFITT system induces a lower temperature in the vein compared with other technologies leading to a reduced risk of thermal damage to surrounding tissue.
Patients had very little pain after the RFITT procedure with a maximum score on day 1 of 2 (VAS range 0 to 10). Kabnick reported an average pain score of 2.2–2.6 on a visual analogue scale of 0–5 after endovenous laser therapy. 21 The reduced pain with RFITT compared with 810-nm laser EVLA has been re-ported previously in a study of 38 patients with bilateral disease. 15 One of the reasons for lower pain scores with RFITT may be the significantly lower temperature used, combined with the rounded catheter tip which reduces the risk of mechanical injury of the vein wall.
Complication rates were similar to other methods of endovenous thermal abalation. Haematoma occurred in only two patients (0.3%), significantly lower than reports on EVLA. Paresthesia, dysesthesia and hypoaesthesia were documented separately but combined in the evaluation as sensory disturbances (5.8%), since in some patients both paresthesia and hypoesthesia was diagnosed. Sensory disturbances could be caused by mechanical injury during the intervention (including phlebectomies), through thermal destruction, or because of postoperative inflammation during the reparative and reactive changes in the area surrounding the vein. The latter might explain why symptoms settled after a median of nine weeks.
One criticism of the study is that the diameter of the treated veins was not recorded. There was no record of selection or exclusion of patients on the basis of vein diameter. The overall results do reflect the performance of RFITT in a large and diverse patient group that probably represents that of daily practice in clinical reality. According to the investigators, the largest vein diameters that have been successfully treated in this study were 23 mm.
Long-term results of RFITT are not yet available. Several studies have shown good results for RFA up to 24 months and it is probable that the results of RFITT will be similar.1,2,22,23 As most of these technologies are new, the lack of long-term results with a follow-up time of five years or more is a general weakness for all endoluminal techniques.
Conclusion
This large multicentre study of RFA using the RFITT method has demonstrated that it is efficacious, well tolerated by patients and has a low incidence of procedure-related postoperative complications. Complete occlusion rates of 98.4% can be achieved with adequate experience and the correct settings.