
Abstract
Objectives
Primary aneurysms of superficial venous system are rare and frequently misdiagnosed as varicose veins. Clinical presentation is variable depending on the presence of compression to surrounding structures. We report a rare case of primary cephalic vein aneurysm presented with wrist pain due to radial nerve compression.
Method/case
A 61-year-old woman was admitted with right wrist pain and localized mass. Physical and imaging examinations showed a localized cephalic vein aneurysm compressing radial nerve. Simple excision was performed successfully.
Results
Cosmetic and clinical results at the first month follow-up were successful.
Discussion
Although primary superficial venous aneurysms of upper extremities are very rare, the treatment of choice is most commonly same as the ones in lower limbs. Simple excision is the best approach in the most of the cases, while sclerotherapy could be preferred in order to obtain better cosmesis or to avoid injuries to surrounding structures.
Objectives
Primary venous aneurysms (VAs) are very rare and defined as idiopathic. Etiological causes for secondary VAs are most commonly defined as inflammation, trauma, iatrogenic and presence of arteriovenous malformations and chronic venous hypertension. 1 Reviewing the literature we found only a few previous reports of primary VAs in the upper extremities. We report a case of a primary large aneurysm in the cephalic vein which treated successfully by simple excision.
Method case
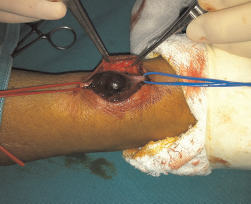
A 61-year-old woman was admitted with increased right wrist pain and numbness during extension of hand and radiates to first, second and third finger and localized mass appeared spontaneously six months ago. She has no history of trauma or infectious event at the corresponding area. Physical examination revealed a 4 cm × 3 cm, superficial, non-pulsatile, compressible mass with no tenderness (Figure 1). Doppler ultrasonography showed its origin from cephalic vein and absence of any communication with radial artery. Presence of signs of venous hypertension and thrombosis were also excluded in Doppler investigation. Excision of mass with local anaesthesia was planned. Following a 3-cm longitudinal skin incision above mass, dissection confirmed a saccular aneurysm (Figure 2). Because of close proximity of radial nerve, surrounding tissues were separated carefully and VA was excised after ligation of proximal and distal necks with 2/0 silk.
Appearance of venous aneurysm before surgery Surgical excision of venous aneurysm
Results
At the first month follow up the cosmetic results were satisfying as no visible scar tissue was eminent. Neurological symptoms were completely disappeared. Histopathological investigation of aneurysm sac revealed fragmentation of elastic tissue and loss of smooth muscle cells along with focal areas of endothelial denudation consistent with VA. Also pathological examination was excluded the presence of an organized thrombus formation inside the VA.
Discussion
Many studies mentioned the rarity of primary superficial VAs.2,3 A study about primary VA showed that, 4.77% of the VAs were located in the lower extremities and most of them were in the deep venous system; 10% were located in the upper extremities. 4 To date only 17 reports of superficial VAs of upper extremities have been published in the English language literature and just one case described radial nerve compression induced by a cephalic VA.2,5
The aetiology of VA remains unclear, although several theories have been elaborated. Primary VA of the superficial venous system occurs due to congenital weakness of the vessel wall which may be related to increased expression of matrix metalloproteinase-2, −9 and −13, 6 but secondary type of aneurysms of the superficial venous system occurs due to trauma, inflammation, degenerative changes in the vessel wall or increased pressure within the venous system, including varicose veins. 1
Primary VA of superficial venous system is a rare clinical entity, thus it can be misdiagnosed as varicose veins, arteriovenous malformations and subcutaneous soft tissue tumours 7 accordingly, our patient was misdiagnosed as lipoma. When suspected, ultrasonographic scanning not only enables confirmation of the diagnosis, but also reveals associated conditions such as thrombosis or compression of surrounding tissues in most cases.5,8
Although simple excision is adequate in most cases, sclerotheraphy could also be a non-surgical alternative in order to obtain better cosmetic results in appropriate cases. 7 In our case simple excision was elected in order to guarantee to abolish radial nerve compression causing forearm pain.
In conclusion, despite their rarity, VAs should be considered in patients with compressible, non-painful masses. In all cases, an accurate preoperative diagnosis with Doppler ultrasonography and evaluation allows appropriate surgical planning.