
Abstract

Telangiectatic matting is a well-known side-effect of various phlebological procedures, from sclerotherapy (70–84%) and phlebectomies (0.5–9%) to stripping of saphenous veins. 1,2 In many patients with new vessel formation, they disappeared spontaneously within a year. 1,2 In a prospective analysis of 100 patients treated by endovenous laser ablation, Timperman 3 noted the occurrence of new spider veins in one subject. It is believed that secondary telangiectasia are a consequence of neoangiogenesis as a response to inflammation and/or trauma to venous blood vessels, but firm evidence is lacking.
Over the past years we have noticed that some patients undergoing radiofrequency segmental ablation (RFSA) of saphenous veins have reported that new telangiectasia and venulectasia within the area of treated veins appeared de novo several weeks following the procedure. In some of them the vessels persisted for a year and longer. We used to treat them successfully with polidocanol foam sclerotherapy.
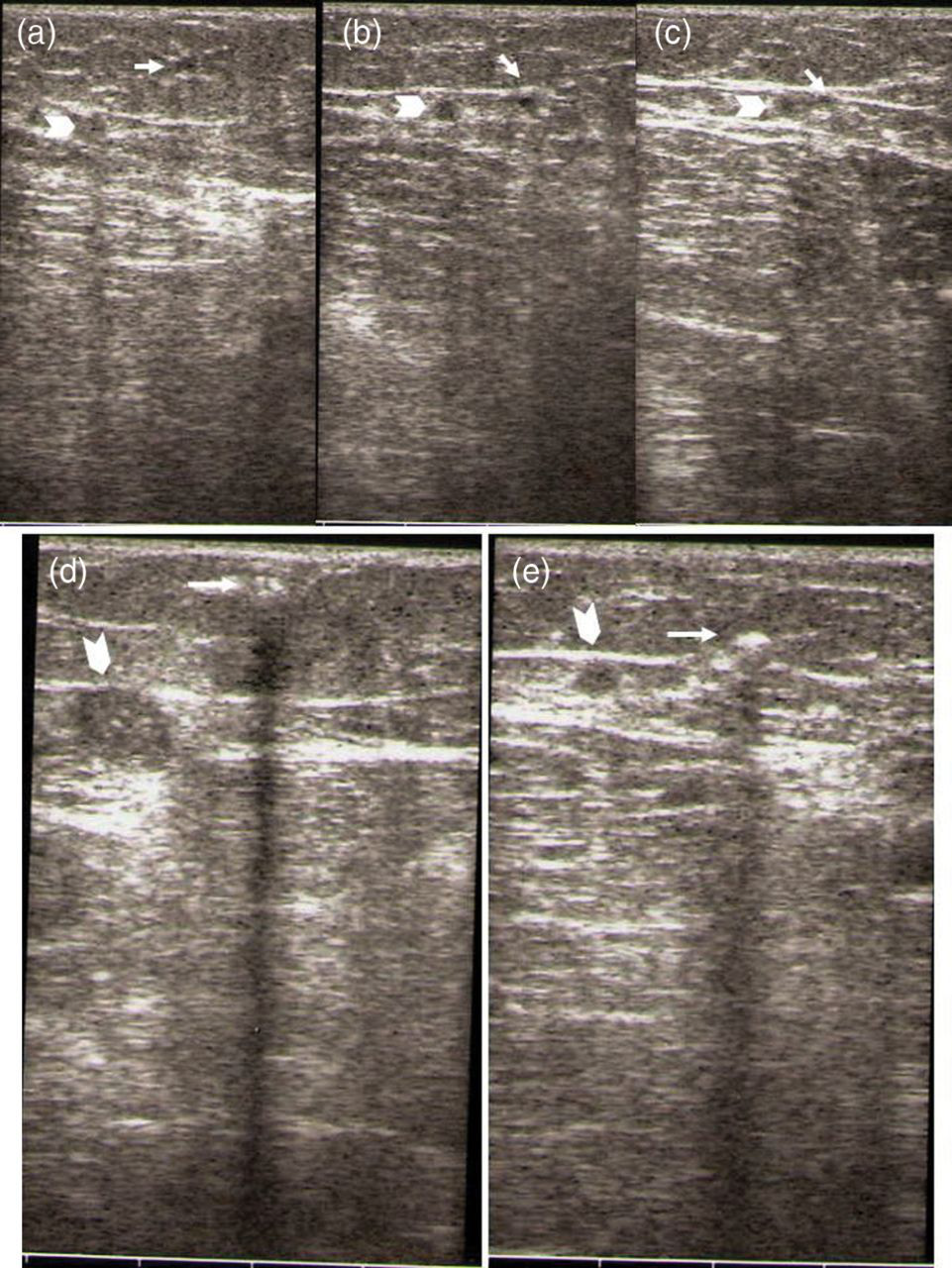
A 54-year-old woman complained of unsightly varicose veins in both lower legs, heavy legs, swelling of ankles at the end of day and occasional burning sensation over some varicosities. Duplex ultrasound examination revealed dilated and refluxing both great saphenous veins (GSV) and numerous subcutaneous varicose veins in both lower legs. In September 2011 we performed segmental RFA (VNUS® ClosureFAST) of both GSV along with phlebectomies of subcutaneous varicosities in the local tumescent anaesthesia. At a follow-up visit six weeks later she drew our attention to newly formed telangiectasia on the medial aspect of her left thigh (Figure 1). She claimed that the new vessels became visible as early as three weeks after the procedure. Both GSV were completely closed from the saphenofemoral junction to the proximal third of her legs. Other superficial and deep veins were unremarkable. On clinical examination, even with transillumination, no feeding vein could be traced from the telangiectatic flare. However, ultrasound revealed a small subcutaneous vein (diameter 1 mm) going from underneath the telangiectasia, directed cranially through subcutaneous tissue, piercing saphenous fascia and ending into the GSV (Figure 2). The feeding vein was not refluxing. We then injected 0.8 mL of the 0.5% polidocanol foam (Tessari, liquid:air ratio 1:4) into the visible cutaneous vessels. The foam quickly spread into the feeding vein we easily tracked by ultrasound up to its connection to the obliterated GSV (Figure 2). Four weeks later the feeding vein was closed and most telangiectasia disappeared but even finer telangiectatic matting over the area could be seen (Figure 1b).
(a) A flare of spider veins on the inner aspect of thigh in a patient six weeks after radiofrequency closure of the great saphenous vein. (b) Four weeks after sclerotherapy of the feeding vein by 0.5% polidocanol foam most previous telangiectasia disappeared replaced by finer telangiectatic matting over the area (white arrows) Ultrasound (B mode) tracking of the feeding vein (white arrow) underlying the spider vein flare: (a–c) the subcutaneous vein is going directly into the closed great saphenous vein (white arrowhead); and (d–e) polidocanol foam flowing from the cutaneous telangiectasia into the feeding vein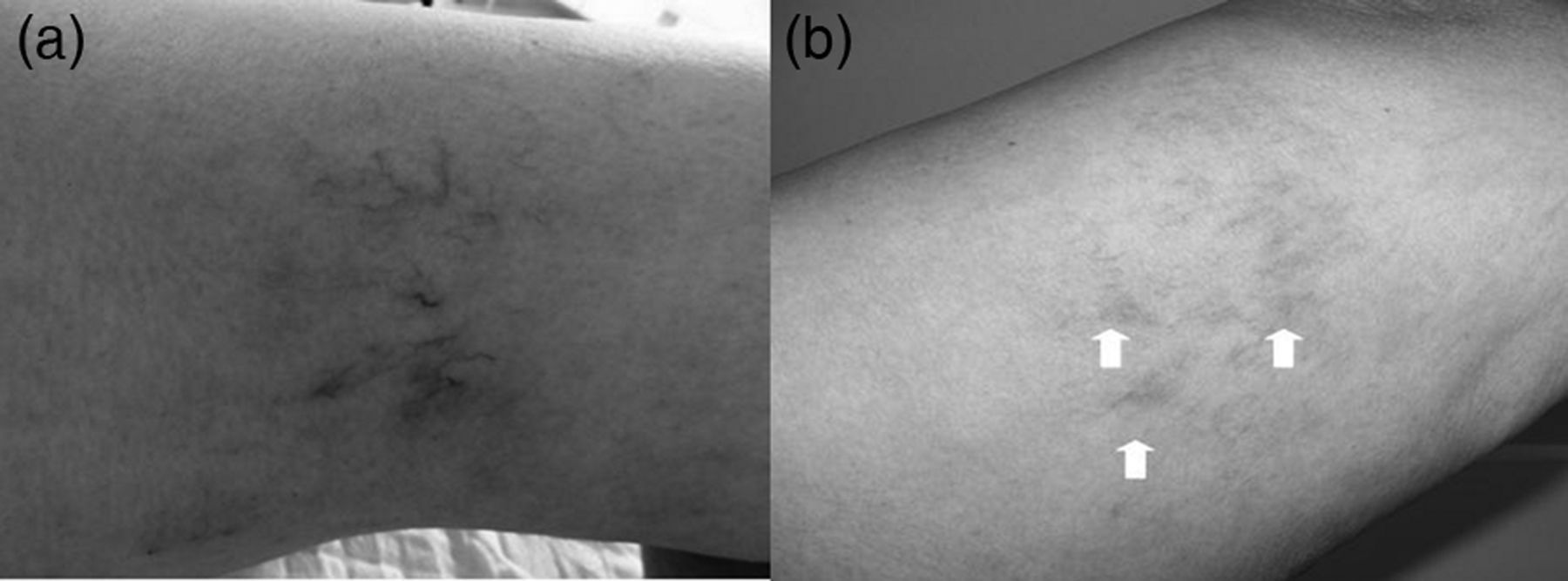
This patient clearly shows that telangiectasia may appear soon after RFSA, probably as a result of the obstruction of normal outflow of cutaneous and subcutaneous veins, in this case into thermally obliterated GSV. Now being aware of the phenomenon, in the meantime, we have observed another case of secondary telangiectasia in the thigh after RFSA of the GSV. We speculate that a sudden increase in pressure within the functionally disconnected vein may cause its dilation and occurrence of visible vessels in the skin. This process is rapid, taking probably a few weeks. In contrast to telangiectatic matting which is presumably a result of neoangiogenesis, the secondary telangiectasia are probably vessels dilated due to a sudden rise in the intraluminal pressure caused by outflow obstruction. In the absence of sufficient collaterals, the hypertension will be prolonged causing visible cutaneous vessel dilation. The outflow obstruction at the level of GSV may have the same consequences as the incompetence of ‘boundary’ valves in GSV tributary veins as recently described by Vincent et al. 4 The occurrence of fine telangiectatic matting after successful occlusion of the feeding vein by sclerotherapy might add further proof to the theory: additional rise in the pressure caused by vessels’ obstruction by sclerotherapy induces dilation of more distal thinner (red) vessels. It may well be that this matting will gradually disappear with time.