
Abstract
Objectives:
A case of delayed popliteal artery injury (PA-INJ) onset after total knee arthroplasty (TKA) in a patient under postoperative anticoagulation therapy is reported. The role of anticoagulation both in late PA-INJ presentation and in PA-INJ management is discussed.
Report:
An obese 76-year-old woman was presented with a common femoral vein thrombosis coupled with pulmonary embolism five days after TKA. She was immediately placed under anticoagulation therapy. Four days later, during physiotherapy-supervised mobilization, she developed a calf haematoma and large retro-articular pseudoaneurysm. Angiography revealed a minor PA-INJ successively treated with a covered stent-graft.
Conclusions:
In cases of initially undetected and staunched TKA-related PA-INJs, postoperative anticoagulation therapy may act as a potential trigger for final arterial rupture during mobilization exercises, followed by acute bleeding; in these cases, endovascular management represents an excellent treatment option.
Close clinical and instrumental monitoring is strongly recommended after TKA, in patients who imperatively require full-dose anticoagulation therapy.
Introduction
Popliteal artery injury (PA-INJ) represents a relatively rare but potentially limb-threatening complication of total knee arthroplasty (TKA)1,2 with a reported incidence ranging from 0.03% to 0.51%.1,3 Revision TKA-surgery is associated with an approximately doubled risk of arterial injuries. 3
PA-INJs may occur both intraoperatively or in the first postoperative hours but may also occur several days or weeks after surgery.1,3
We report a case of delayed PA-INJ presentation after TKA in a patient under anticoagulation therapy for postoperative deep vein thrombosis (DVT) coupled with pulmonary embolism and discuss the role of anticoagulation both in late PA-INJ onset and in iatrogenic arterial injury management.
Case report
An obese 76-year-old woman suffering from severe debilitating right knee arthrosis underwent surgery for TKA. No particular intra or postoperative problems were reported. Immediately after TKA, to reduce postoperative pain she was submitted to repetitive local anaesthetic injections into the posterior knee joint capsule (via 18G-needle). The patient had undergone usual low-molecular-weight heparin DVT prophylaxis (weight-adapted nadroparin calcium). Five days after surgery she complained of moderate ipsilateral calf pain coupled with impending dyspnoea. Local physical examination evidenced only mild lower limb swelling, especially at calf level; peripheral arterial pulses were all palpable. Duplex ultrasound scans evidenced a common femoral vein thrombosis originating approximately 10 cm under the inguinal ligament while computed tomography (CT) pulmonary angiography showed a small pulmonary embolus in the left lower lobe peripheral vessel. She was immediately placed under full-dose anticoagulation therapy. Repetitive duplex ultrasound scans, performed for DVT surveillance, resulted negative for PA-INJs.
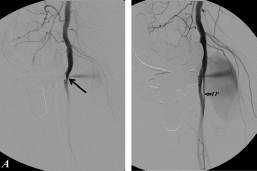
Four days later, during physiotherapy-supervised mobilization exercises, she experienced a sudden sharp pain in the calf and swelling. Duplex ultrasound scans showed a large haematoma in the gastrocnemius muscular bellies and suggested a popliteal artery pseudoaneurysm. Lower limb angio-CT confirmed this suspect but failed to show the exact localization because CT imaging was hampered by the knee prosthesis (Figure 1). Digital subtraction angiography revealed a small posterior PA-INJ (near an anomalous high tibialis posterior origin), feeding a large retro-articular pseudoaneurysm (Figure 2); PA-INJ was successfully treated with a small covered stent-graft, percutaneously implanted (5 mm x 25 mm; VIABAHN®, WL Gore Associates Inc., Flagstaff, AZ 86004, USA) (Figure 3). At the moment of arterial bleeding international normalized ratio (INR) values were within the therapeutic range (INR: 2.45). The patient was discharged under oral anticoagulation (warfarin) coupled with antiplatelet medication (aspirin). At four-months follow-up no pseudoaneurysm recurrence or stent-related complications were observed.
Angio-CT: large pseudoaneurysm at popliteal artery level (small arrow) coupled with extended haematomas in the gastrocnemious muscular bellies (large arrows). CT-imaging is hampered by knee prosthetic material in situ. CT, computed tomography Digital subtraction angiography: active bleeding from a small posterior PA-INJ (small arrows) feeding a large retro-articular pseudoaneurysm. Note the anomalous high TP origin in proximity of the PA-INJ location. PA-INJ, popliteal artery injury; TP, tibialis posterior artery Digital subtraction angiography: no signs of arterial bleeding are evident after PA-INJ exclusion via small covered stent (5 mm × 25 mm; VIABAHN®) (large arrows). PA-INJ, popliteal artery injury; TP, tibialis posterior artery

Discussion
Arterial injury mechanism during TKA may be direct or indirect. Thrombotic arterial occlusions are generally caused by indirect blunt traumas such as joint manipulation or tourniquet application which can cause intimal damage or atheromatous plaque disruption.1–3 In contrast, intraoperative arterial laceration or transection is generally related to a direct penetrating trauma which can occur with any form of surgical instrumentation (vibrating saw, insertion of screws, scalpel blade, diathermy or misplaced sharp retractors), or may even be caused by exposed sharp bony edges remaining after tibial osteotomy.2,3 Cadaveric studies have demonstrated that during TKA posterior knee retraction, hyperextensions and hyper-flexions may expose popliteal vessels to high risk for injuries. These injuries may present as intraoperative haemorrhage, pseudoaneurysm, arteriovenous fistula or recurrent haemarthrosis. 3
In this case, considering PA-INJ characteristics and size, the minor vessel-wall laceration may be related to a direct trivial arterial penetrating trauma or, most probably, incorrect anaesthetic-needle insertion into the posterior knee-joint capsule. This procedure is normally practiced via intra-articular approach. Needle insertion into the posterior knee-joint capsule is therefore performed visualizing only the articular surface of the posterior knee-joint capsule. To prevent possible vascular injuries this manoeuvre is performed carefully via a small needle avoiding deep insertion into the posterior knee-joint capsule. In this case, however, the patient's anatomical characteristics (overall obesity including the knee and lower limbs), significantly increased the risk of intraoperative injuries of the vessels. In this regard it should also be noted that vascular injuries occurring during TKA may not be immediately evident because the operation is normally performed under tourniquet-induced limb ischaemia.1,3 It also seems probable that the small PA-INJ was initially staunched by local thrombus formation and that anticoagulation, mandatory in this case, may have promoted final arterial rupture during knee-joint mobilization exercises, followed by acute bleeding. It must also be noted that DVT requiring anticoagulation therapy may coexist and can frequently occur following venous compression by mass effect of a popliteal artery pseudoaneurysm.1–3 In this case, however, this relationship is highly unlikely because of the location of the thrombosis and the time of appearance.
There is no consensus on the optimum management of TKA-related iatrogenic pseudoaneurysms. Some authors state that the best results are obtained with bypass surgery 4 but this is associated with significant morbidity. 5 These lesions may also be treated with simple patch angioplasty or excision and repair. However, in most cases (as in this one), this management can be technically challenging due to scarring, haematomas, limb swelling and adiposities. Percutaneous injection of thrombin to occlude popliteal pseudoaneurysms is also established. 1 In the present case, however, pseudoaneurysm size and anticoagulation therapy precluded this approach. Few cases of TKA-related popliteal pseudoaneurysm treatment via covered stent-grafts have been reported to date. 1 Considering both PA-INJ size and location (near the high-origin tibialis posterior) and the absolute necessity for anticoagulation, we implanted a small covered stent-graft percutaneously No pseudoaneurysm recurrence or stent-related complications were detected at four-month follow-up.
Conclusions
In cases of initially undetected and staunched TKA-related PA-INJ, postoperative anticoagulation therapy may act as a potential trigger for final arterial rupture during mobilization exercises, followed by acute bleeding; in these cases, endovascular management represents an excellent treatment option.
Close clinical and instrumental monitoring is strongly recommended after TKA in patients who imperatively require full-dose anticoagulation therapy.
Footnotes
Acknowledgements
The authors wish to thank Ms Elena Harwood for the linguistic revision of this paper and the operating-room nurses Ms Brigitte Hofer, Ms Margot Messner and Ms Birgit Schnarf for their help in the careful analysis and revision of the instruments employed during the different phases of total knee arthroplasty surgery.