
Abstract
Objectives:
Heterotopic ossification is defined as the abnormal formation of true bone within extraskeletal soft tissues. It may be associated with a variety of clinical conditions, but is most frequently seen with musculoskeletal trauma, neurologic injury or genetic abnormalities. It has also been described in patients with chronic venous insufficiency; however, it often goes underdiagnosed due to chronic ulceration that masks exam findings. To date, few reports of heterotopic ossification due to chronic venous disease exist within the literature with the most recent dating back to the 1970s.
Methods:
We present a case study of a man presenting with extensive leg ulceration and a history of chronic venous insufficency. He had a large non-healing venous stasis ulcer of the left lower extremity with extensive heterotopic ossification discovered intraoperatively.
Results:
The patient was managed with serial wound debridement, innovative woundcare and eventual split thickness skin grafting that achieved limb salvage despite the complexity of his wound.
Conclusions:
Our discussion focuses on the epidemiology, pathophysiology, diagnostic work-up and management of heterotopic ossification in the setting of chronic venous insufficiency. We propose that heterotopic ossification be included in any future modifications of the clinical, aetiology, anatomy and pathophysiology system classification as a complication of chronic venous disease.
Introduction
Heterotopic ossification is defined as the abnormal formation of true bone within extraskeletal soft tissues. It may be associated with a variety of clinical conditions, but is most frequently seen with musculoskeletal trauma, neurologic injury or genetic abnormalities. However, in 1960, Heinz Lippmann and Goldin 1 published a report of 60 cases with subcutaneous bone formation out of 600 patients with chronic venous insufficiency. Thus, the incidence of heterotopic ossification may be as high as one in 10 patients in the setting of venous insufficiency. Although a similar appearance due to calciphylaxis in the setting of chronic renal failure is not unusual, we believe that heterotopic ossification due to chronic venous insufficiency often goes unrecognized.
Case
A 59-year-old man with a longstanding history of venous insufficiency presented to our institution with a non-healing venous stasis ulcer of the left lower extremity. His surgical history was remarkable for a remote history of left great saphenous vein stripping for thrombophlebitis 30 years earlier as well as recent endovascular laser ablation of the remaining left great saphenous vein. His medical co-morbidities included hypertension, diabetes mellitus and tobacco dependence.
Physical examination revealed lipodermato-sclerosis of the left lower extremity and a malodorous, full thickness ulcer, covered with black eschar and purulent exudate. The ulcer measured 10.5 × 9.1 × 1.5 cm. In addition, there was porous, ossified soft tissue extending from the medial malleolus to the level of the tibial tuberosity (Figure 1). Laboratory studies were remarkable for normal calcium, phosphorus and alkaline phosphatase levels. Parathyroid hormone was decreased at 7.8 pg/mL. Plain films illustrated extensive sheet-like calcifications involving the subcutaneous fat of the medial, left lower leg (Figure 2). There were no signs of osteomyelitis or intramuscular calcification noted on magnetic resonance imaging.

Initial examination revealed a full thickness ulcer with black eschar and purulent exudate, as well as porous ossified soft tissue

Large medial soft tissue defect with extensive adjacent soft tissue calcification
During intraoperative debridement, the patient was found to have extensive heterotopic ossified subcutaneous tissue involving the base of the ulcer and extending up to the level of the tibial tuberosity without invasion of the underlying gastrocnemius or soleus muscles. A wide-local excision of the skin and subcutaneous tissue was performed resulting in a 21 × 27 cm defect (Figure 3). Consistent with a polymicrobial infection, methicillin-resistant Staphylococcus aureus, Pseudo-monas aeruginosa, Klebsiella pneumoniae, Enterococcus faecalis, Enterobacter cloacae, extended-spectrum beta-lactamase positive Prevotella oralis, Bacteroides fragilis and a Clostridium species were cultured from the wound. Histological examination was remarkable for dense, fibrous connective tissue with acute inflammation and focal osseous metaplasia without evidence of malignancy.
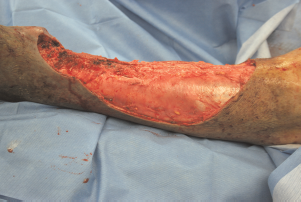
A wide-local excision of the skin and subcutaneous heterotopic tissue was performed resulting in a 21 × 27 cm defect
The patient received a 14-day-course of intravenous vancomycin and ertapenem and returned to the operating room for serial wound debridement during his hospital stay. Living bilayered skin substitutes were placed over exposed tibia to promote granulation, and a wound vacuum-assisted closure device was utilized to close the wound defect (Figure 4). We then used a two-layer skin regeneration system to further enhance closure. The outer layer consists of a thin silicone film that acts as a surrogate epidermis to protect the wound from infection, control heat exchange and limit moisture loss. The inner layer is constructed of a complex matrix of cross-linked fibres. This porous material serves as a scaffold for regenerating dermal skin cells thus enabling the re-growth of a functional dermal layer of skin (Figure 5). Once dermal skin has regenerated, the silicone outer layer is removed and replaced with a thin epidermal skin graft. Twelve weeks after his initial presentation, our patient underwent successful split-thickness skin grafting with approximately 95% incorporation of the graft (Figure 6).

A living bilayered skin substitute was placed to promote granulation over exposed bone

A two-layer skin regeneration system was used as a scaffold to regenerate dermal skin cells, enabling the re-growth of a functional dermal layer of skin

Intraoperative photo of definitive split-thickness skin graft
Discussion
Chronic venous insufficiency is a common condition with an annual incidence of about 275,000 people per year over the last 25 years. 2 In 1917, Homans 3 theorized that the characteristic skin changes and ulcerations of chronic venous insufficiency were due to the relative hypoxia of static venous blood, thus decreasing the amount of oxygen reaching the skin surface of the distal lower extremities. Such tissue hypoxia may be due to congenital incompetent valves, acquired incompetent valves related to trauma such as with vein surgery or arteriovenous malformations. 4
Multiple hypotheses exist as to the pathogenesis of subcutaneous ossification in chronic venous insufficiency. These include fat metaplasia, haematoma formation, trauma, hormonal influence and chronic inflammation. Older theory proposes that heterotopic subcutaneous ossification is the result of fat necrosis and subsequent calcification. However, in the case series published by Lippmann and Goldin, evidence of fat necrosis was not noted in any histological sampling. Moreover, the role of heterotopic bone formation due to haematoma was disputed by the Lippmann study, which did not report haematoma formation in the diseased lower extremities of any of their patients. 1 Trauma as the causal mechanism for heterotopic ossification has also been proposed. In 1963, Condin proposed that traumatic displacement of periosteal or cartilaginous cells activated by traumatic stimuli can lead to bone formation in soft tissues. 5 While this phenomenon is certainly plausible, the common finding of heterotopic ossification in patients without trauma is not explained by this mechanism.
Interestingly, venous insufficiency occurs with a typical female to male ratio of 4:1, and heterotopic ossification is most frequently reported in postmenopausal women. In fact, all 60 cases in Lippmann's study were postmenopausal women. Thus, altered hormonal activity may play a role in heterotopic ossification. Hormonal influences on venous dysfunction related to progesterone include passive venous dilation. Also, oestrogen relaxes smooth muscle fibres and softens collagen fibres. 6 Cases of heterotopic ossification have been reported in men with neither a history of trauma nor congenital malformations. In these instances, the primary risk factor was a longstanding history of chronic venous insufficiency in association with chronic ulceration. 1 Recent theories propose that de novo metaplasia transforms subcutaneous tissue into viable bone, likely enhanced by chronic venous insufficiency. 1 The exact pathogenesis remains unknown and is an area that requires future research.
The typical presentation of subcutaneous ossification in the setting of chronic venous insufficiency usually involves a recurrent or non-healing ulcer consistent with CEAP clinical class 6. The CEAP classification is a descriptive classification system for chronic venous disorders created at the consensus conference of the American Venous Forum in 1994. 7 CEAP is an acronym that stands for: clinical, aetiology, anatomy and pathophysiology. Currently, the clinical CEAP classification includes stages C0–C6:
C0: No visible or palpable signs of venous disease;
C1: Telangiectasies or reticular veins;
C2: Varicose veins; diameter of 3 mm or more;
C3: Oedema;
C4: Changes in skin and subcutaneous tissue:
C4a: Pigmentation or eczema.
C4b: Lipodermatosclerosis or atrophie blanche;
C5: Healed venous ulcers;
C6: Active venous ulcers;
S: Symptomatic, including ache, pain, tightness of skin, irritation, heaviness and muscle cramps and other complaints attributable to venous dysfunction;
A: Asymptomatic.
Other findings of advanced stage venous insufficiency noted concurrently with subcutaneous ossification include lipodermatosclerosis, chronic ulceration and granular induration. In addition, in our patient large sheets of woody subcutaneous tissue were palpable. These findings should alert the clinician caring for the wound that subcutaneous ossification may be present. The differential diagnosis includes collagen vascular disorders such as Ehlers–Danlos syndrome, scleroderma/ morphea and dermatomyositis; malignancy such as soft tissue sarcomas, osteogenic sarcomas and metastatic carcinoma; and hyperparathyroidism. 8 If chronic venous insufficiency is the culprit, laboratory evaluation will fail to demonstrate a disturbance in calcium or phosphorus metabolism. 1 Radiographically, extensive calcification in the soft tissues can be appreciated on plain films as well as computed tomography. 8 Pathologically, the ossified tissue consists of mature cancellous bone in plates, sheets or rings; as well as inflammatory cells with scattered hemosiderin-laden macrophages consistent with benign diffuse osteoma cutis. 8
Non-operative medical management of heterotopic ossification is primarily preventive, treating chronic venous insufficiency before ossification occurs with compression stockings and intermittent extremity elevation. 6 Management of heterotopic ossification with ulceration requires surgical intervention. Ulcerative lesions with concomitant heterotopic ossification do not heal until the ossified tissue is completely resected. 1 Once resected, aggressive wound care is essential to promote wound healing and prevent infection. Additional wound coverage with an autograft or biosynthetic skin substitute can assist in the ultimate goal of salvaging the limb.
Conclusion
As in our case, operative management of heterotopic ossification in the setting of chronic venous insufficiency can lead to successful closure of the non-healing wound. Our patient underwent resection of the cancellous tissue with aggressive wound care and negative pressure wound therapy. Once a healthy bed of granulation tissue evolved, the patient underwent placement of a bilayered living skin substitute and eventual split thickness skin grafting with subsequent full functional return.
Heterotopic ossification is a pathological process that may be caused by chronic venous insufficiency. Diseased tissue at the subcutaneous level likely promotes long-term chronic ulceration that requires resection of the calculus tissue and subsequent skin grafting in order to achieve healing. This surgical intervention contrasts with the usual approach of local wound care and compression therapy for venous stasis ulcers. It requires different treatment with a distinct expected clinical outcome. Therefore, we propose that any future modifications of the CEAP system clinical classification should include a consideration of heterotopic subcutaneous ossification. Making a distinction in this regard will not only heighten awareness but also assist in future research regarding this serious complication of longstanding chronic venous insufficiency.
Disclaimer
The views expressed herein are of the authors and do not reflect the official policy of the Department of the Army, Department of Defense or the US Government. The authors report no conflict of interest – financial, personal or professional – concerning the preparation of this manuscript.