
Abstract
Objectives
To examine and compare the effects of downwards versus upwards total stripping of great saphenous vein (GSV) on saphenous nerve (SN) injury using clinical and electrophysiological studies.
Methods
Fifty patients with varicosities were equally and randomly assigned to undergo total, upwards stripping (group A) or downwards stripping (group B) of GSV during saphenectomy. SN function was measured with electroneurogram (ENG) before operation, two weeks and 12 weeks after, in order to record the incidence and type of SN injury. Clinical signs of SN injury were also recorded at the same time points. The results were statistically analysed.
Results
There were no statistical significant differences on the occurrence of SN injury between groups A and B at two and 12 weeks, respectively, as confirmed with ENG studies and clinical evaluation. There were no differences between the two techniques with regard to the type of SN injury. SN injury was significantly ameliorated from 34% to 6% during the first three months.
Conclusion
SN injury was equally observed after downwards or upwards total stripping of the GSV, as confirmed by ENG and clinical evaluation, with no differences in injury type. SN injury tends to be relieved through time in most patients.
Keywords
Introduction
Saphenous nerve (SN) injury represents a complication of great saphenous vein (GSV) stripping, with an incidence which ranges between 3% to above 50%.1–3 It is mainly associated with procedures of total GSV striping from ankle to thigh and attributed to the nerve trauma from the passage of the stripper head near or over the SN and its branches. In order to reduce its incidence invaginated and short stripping have been introduced as less traumatic techniques; however, the role of the first is debated through randomized studies,4,5 while the second, although reducing SN damage, may be associated with persistent below knee GSV reflux after surgery and recurrence of clinical symptoms. 6 Total GSV stripping may be a choice for treating patients with GSV reflux extending to its below knee portions, ignoring the higher incidence of SN injury because the latter is supposed to have minimal clinical significance. 7 Despite the debated clinical impact of SN injury,3,8 several attempts have been made in order to recognize and reduce the factors associated with its occurrence. The direction of stripping has been suggested as one of those; 9 however, data from several studies raise questions about its direct association with SN damage.10,11
In the present study, we compared upwards to downwards total GSV stripping with regard to the occurrence, type and clinical course of postoperative SN injury. In addition to clinical evaluation, electroneurogram (ENG) measurements were also used to reliable define the type and occurrence of SN sensory impairment.
Materials and methods
Preoperative characteristics of the patients according to age, sex, BMI and CEAP score
BMI, body mass index; CEAP, clinical, aetiological, anatomical and pathological elements
*P = 0.6 and 0.495 for age and BMI, respectively, when the two types of stripping compared (Mann-Whitney U test)
The day before surgery all patients underwent a baseline ENG measurement to exclude cases positive for SN injury prior to surgery, as well as patients with undetectable nerve responses. All procedures were performed under general anaesthesia by the same surgical and anaesthesia team. Surgery was consisted of a standard high ligation and disconnection of the GSV to the saphenofemoral junction accompanied by total, one-stage GSV conventional (not invaginated) stripping and local phlebectomies. We used medium stripper heads in all cases (TELIC, S.A. Barcelona, Spain). Distal capture of the GSV was done through a 10 mm incision above the medial malleolous. The subcutaneous fat and perivenous tissue were dissected carefully and the vein was ligated and cut only after we were sure that it was clear from any surrounding tissues. Local phlebectomies near the ankle were avoided to all patients. Leg compression bandage was applied after the end of the procedure in cases of downwards striping. In cases of upwards striping leg bandage was applied from the foot to the middle thigh simultaneously to striper removal. Patients were allowed to stand up and walk by the same day and dismissed home the day after.
Clinical and electrophysiological criteria for saphenous nerve injury

ENG, electroneurogram; SNAP, sensory nerve action potential; NCV, nerve conduction velocity
The study had 80% power to detect more than 30% differences between groups A and B as computed by IBM Sample Power 3 (IBM Corporation, Armonk, NY, USA). This power level was considered as adequate, taking into account the already published differences on SN injury between downwards and upward GSV stripping in studies comparing these two methods.9,16,17 Summarizing the results of these studies, the mean value of positive cases for SN injury was 49% for the upwards stripping and 11% for the downwards stripping at three months follow-up. The results were statistically analysed with the IBM SPSS Statistics 20 software (IBM Corporation, Armonk, NY, USA) using cross-tabulation and non-parametric statistics. P value of less than 0.05 was considered significant.
Results
Saphenous nerve injury as detected by electroneurogram and clinical examination
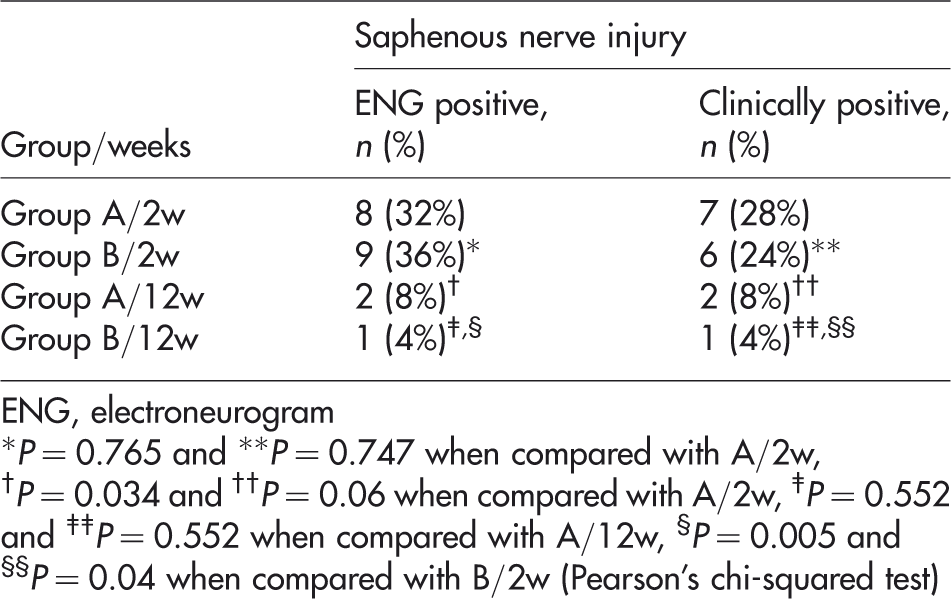
ENG, electroneurogram
*P = 0.765 and **P = 0.747 when compared with A/2w, †P = 0.034 and ††P = 0.06 when compared with A/2w, ‡P = 0.552 and ‡‡P = 0.552 when compared with A/12w, §P = 0.005 and §§P = 0.04 when compared with B/2w (Pearson's chi-squared test)
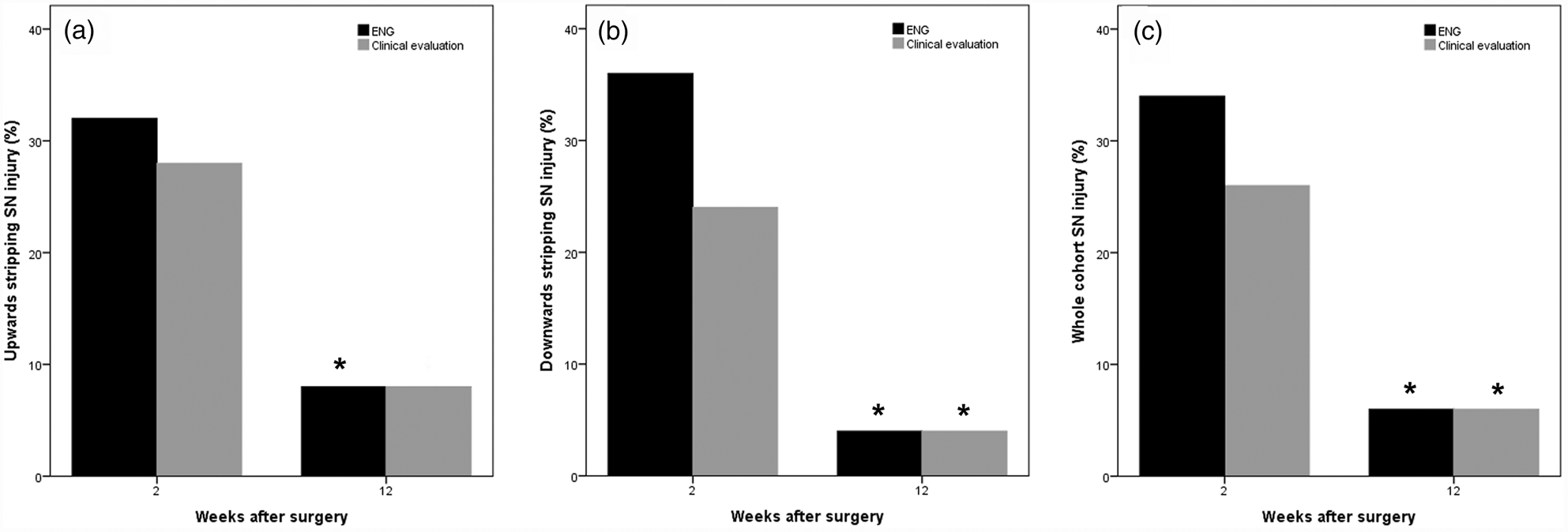
Charts showing the time course of saphenous nerve (SN) injury during follow-up, (a) after upwards stripping, (b) after downwards stripping and (c) for the whole cohort. *P < 0.05 when compared with two weeks follow-up for the same stripping group. Clinical evaluation (grey bars) compared with electroneurogram (ENG) measurements (black bars) underestimates SN injury at two weeks in all groups
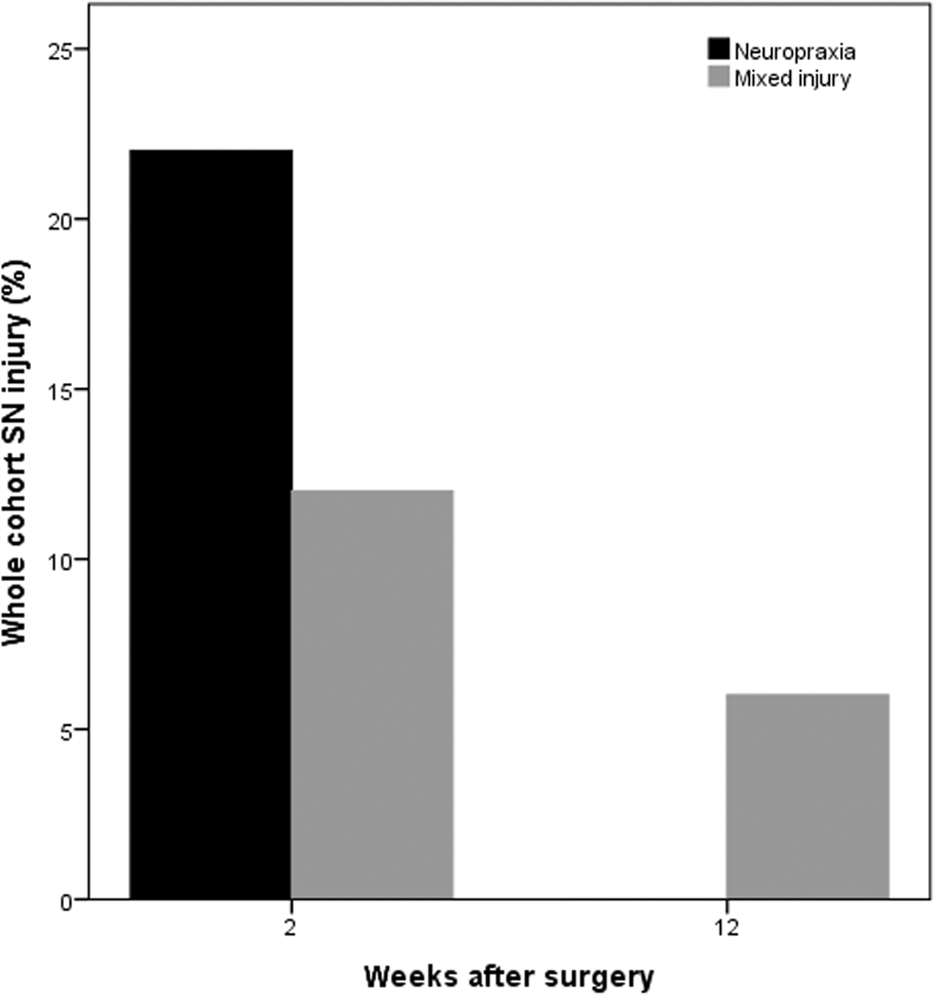
Chart showing the incidence and time course of each type of saphenous nerve (SN) injury as a percentage of the whole patient cohort. Neuropraxia is completely abolished during the first 12 weeks after surgery, while mixed injury is reduced by 50%
With regard to ENG studies at two weeks, pathological measurements were found in 32% (8/25) of group A patients and 36% (9/25) of group B patients. At 12 weeks, ENG studies revealed SN injury in 8% (2/25) of group A patients and in 4% (1/25) group B patients. Statistical analysis found no significant differences between groups A and B both at two and at 12 weeks follow-up (P = 0.765 and P = 0.552, respectively, Pearson's chi-squared test). ENG measured nerve function showed statistically significant improvement from two to 12 weeks with both methods of stripping (Table 3).
Clinical evaluation at two weeks detected sensory deficits in 28% (7/25) of group A and 24% (6/25) of group B patients. At 12 weeks the detected sensory deficits were 8% (2/25) and 4% (1/25) for groups A and B, respectively. Deficits at 12 weeks were seen as hypoesthesias with positive touch tests in all patients, while one additionally suffered from occasional pain. Statistical analysis found no significant differences between groups A and B both at two and at 12 weeks follow-up (P = 0.747 and P = 0.552, respectively, Pearson's chi-squared test). All clinical positive cases were also ENG positive; however, clinical examination failed to detect four cases at two weeks. Significant improvement in clinical symptoms was detected from two to 12 weeks in group B and marginally insignificant, possibly due to underestimation of injury, in group A (Table 3).
With regard to the quality of the ENG results, 11 (5 upwards, 6 downwards) of the 17 recorded pathological cases at two weeks had characteristics of predominant neuropraxia (normal or slightly reduced SNAP, but with significant lowering of NCV). The remaining six cases (3 upwards, 3 downwards) showed mixed injury results of both neuropraxia and axonal damage (significantly reduced or absent SNAP and NCV). At 12 weeks, three (2 upwards, 1 downwards) of the six mixed injury cases were still detectable, while none of the 11 cases of predominant neuropraxia did. No significant differences were found when compared group A with group B for each type of SN injury at both time points.
Discussion
The direction of total GSV striping has been examined in several studies to its relation with the SN injury. Some authors have found that downwards stripping results in lower incidence of postoperative lower calf sensory deficits compared with upwards stripping.9,16,17 This was attributed to the inverted V formation of the SN branches that cross directly the saphenous vein at the lower calf, which predisposes to their entrapment by the striper head and avulsion when the latter is pulled in an upwards manner.9,16 However, and in contrast to the above findings and suggestions, a number of other authors have concluded in their studies that the direction of stripping does not affect the incidence of postprocedural sensory neurological impairment.10,11 Our clinical findings are in agreement with the latter. Moreover, and apart from the clinical symptoms which may sometimes be misjudged, we have reliably shown that the incidence of true SN injury as this can be determined through functional ENG studies by measuring the SNAP, NCV and latency times, does not differ significantly between upwards and downwards stripping. The fact that previous studies of histological examinations of stripped saphenous veins have shown that nerve fragments can be also found in a significant number of downwards stripped veins could additionally support these findings. 18 The assumption that downwards stripping is an atraumatic method may not be valid in the clinical setting. When the stripper is pulled in a downwards manner, after passing the level of the knee, already carries a large segment of GSV and avulsed tributaries, which significantly increase its head diameter. In that way its passage through the calf, a region with far lower compliance than thigh, requires a significant amount of strength and leads to an extensive subcutaneous trauma, which undoubtedly may injure the crossing SN branches. Passage through calf might be easier when the striper is pulled upwards.
The objectively recorded SN injury using ENG, was found to be higher than the clinically detected neurological deficit at two weeks. These findings suggest that the difference between clinical and ENG studies could be a result of either borderline severity of the injury, with subsequent subclinical effect, or misjudgments of the aetiology of the symptoms by the examiner. In any case it seems that not all of the functional deficits can be detected or are revealed clinically, especially at the first weeks of follow-up where additional clinical situations (e.g. presence of haematoma and oedema) may outshine them. The overall ENG-detected SN injury in our study was 34% at two weeks. This finding is well correlated with recent histological results of dissections, where in one-third of individuals the SN was very close to the GSV wall; a fact that could be a possible cause of injury in cases of total GSV stripping. 19 Similarly to the mechanical damage of stripping, endovenous ablation may result in thermal nerve injury when it is extended to below knee GSV. Thus, tumescent-dilute anaesthesia should be applied into the below knee saphenous compartment in order to increase the distance of GSV from the nerve and prevent neurological injury.20,21
In both upwards and downwards stripping, sensory impairment was significantly ameliorated and the clinical symptoms tended to be relieved during the first 12 weeks after surgery. This injury and symptom relief supports the low clinical impact of SN injury and could be explained by the detected type of neurological damage. Most of the positive cases consisted of predominantly neuropraxic injury, which is generally a mild nerve injury with a benign clinical course. Neuropraxic injury is usually self-resolved within a time of several weeks. 17 All such injuries in the present series were disappeared between two to 12 weeks. Apart from neuropraxia, almost one-third of the positive patients had characteristics of mixed type of injury. Mixed nerve injury, which includes axonal damage in addition to neuropraxia, is considered as a more severe injury. Usually two to six months are needed for this injury to be resolved in cases of limited axonal loss. 22 In our series 50% of mixed injuries were resolved during the first 12 weeks, which suggests that axonal nerve damage during GSV stripping is usually limited and of low clinical importance. It has to be mentioned that no differences were recorded between upwards and downwards stripping in terms of the type of nerve injury.
In conclusion, the present study has shown that there are no significant differences between upwards and downwards total GSV striping in terms of incidence, time course and type of SN injury, as confirmed by electrophysiological nerve studies and clinical examination. The ENG-recorded incidence of SN injury after total GSV striping is 34% at two weeks but is ameliorated to 6% after three months. The predominant type of nerve injury is neuropraxia, which is totally abolished after 12 weeks. Further studies that will examine the occurrence of SN injury after invaginated or short stripping with the use of electrophysiological methods, may offer additional important information for the current clinical practice.
Footnotes
Acknowledgements
We would like to thank Dr Alexis Martzoukos for his excellent assistance on electrophysiological nerve studies.