
Abstract
Objective:
Chronic cerebrospinal venous insufficiency (CCSVI) was recently described in patients with multiple sclerosis (MS). The hypothesis of the vascular aetiology provides a new approach in the investigation and treatment of MS.
Methods:
Our open-label study included 94 MS patients who fulfilled ultrasound sonographic criteria required for CCSVI. The internal jugular and/or azygous veins by a catheter venography were dilated.
Results:
In 34.8% of the patients unilateral, in 65.2% bilateral venous abnormalities and in 2.1% no luminal obstructions were demonstrated. The patient group with the higher disability score had a significantly higher number of venous lesions (P < 0.005). Significant improvement of clinical disability in relapsing-remitting patients was (P < 0.001) achieved. In our study no stents were used. Re-stenosis occurred in 21.7% of the patients.
Conclusion:
The number of venous narrowings is higher in more disabled patients. A significant improvement in clinical disability in the relapsing-remitting group was observed.
Introduction
Multiple sclerosis (MS) is regarded as a chronic inflammatory progressive immune-mediated demye-linating disease of the central nervous system (CNS) characterized by inflammation, demyelination, diffuse axonal damage and neuronal loss.1–3 The cause of MS is still unknown. The role of infection, genetic and environmental factors is discussed in the literature.3, 4
The new vascular hypothesis and its relationship to MS have aroused immense interest in the neurological, vascular and other scientific communities. The disruption of venous flow, known as chronic cerebrospinal venous insufficiency (CCSVI), is characterized by multiple stenoses of the extracranial veins – the internal jugular (IJV) and azygous (AZV) veins as well as the spinal cord venous system.5, 6
For many neurologists, the venous role in the aetiology of MS is contradictory to the present knowledge of MS pathology.7–9
The primary endpoints of this open-label study were to detect and highlight the occurrence of obstruction in the extracranial venous pathway – the jugular and/or azygous veins of MS patients and the distribution of venous lesions. The secondary endpoints were to evaluate the relationship of the venous pathology to the clinical course and the disability of the disease.
Materials and methods
In our study we recruited 94 patients with proven diagnosis of MS diagnosed by revised McDonald criteria. 10 The patients were classified into the three stages of the disease - relapsing-remitting (RR), secondary progressive (SP) and primary progressive (PP) (Table 1). The disability was assessed by the Expanded Disability Status Scale (EDSS). 11 An EDSS score of 1-3 is considered as mild, more than 3 as moderate and 6 and above as severe impairment of ambulation. According to disability, we divided the patients into groups with EDSS <3.0, 3.0-6.0 and >6.0. MS patients included in the study fulfilled two or more of the five proposed criteria obtained by Doppler sonography required for CCSVI. 5 ,6, 12 The five parameters for CCSVI were evaluated by transcranial and extracranial colour-Doppler sonography (Esaote Biomedica Machine, Genova, Italy). Progress duplex ultrasound examination six and 12 months after angioplasty were performed.
Clinical and demographic data

MS, multiple sclerosis; N, number; RR, relapsing-remitting; SP, secondary progressive; PP, primary progressive; EDSS, Expanded Disability Status Scale; SD, standard deviation;
P< 0.001
Before catheter venography (CV) was started, the patients received low-molecular-weight heparin subcutaneously (Heparin Braun 5000 IE/mL). Under local anaesthesia, first the examination of the AZV and then that of the right and left IJV was performed. A luminal diameter reduction of 50% is frequently used as a threshold for angioplasty 5 , 6 ,13, 14 According to the outflow velocity, reflux and presentation of collaterals, the diameter of stenosis can be graded from 1 to 4. 13 To obtain more precise evaluation of the venous flow and the variability of vein lumen, contrast was injected at different levels of the vein.
For the AZV, balloon diameters ranged from 6 to 12 mm, depending on the segment and reference vessel diameters, and were 20-60 mm long. The balloons were expanded to 4-6 atmospheres for one minute. For IJV lesions, balloon diameters varied: distal segments required 7-8 mm balloons, middle segments 10-12 mm balloons and proximal segments 12-20 mm (20-40 mm length). The balloons were expanded at maximum 10 atmospheres and inflations were repeated several times. In hard stenoses, additionally hydrophylic ‘cutting’ wire close to the balloon or the double balloon technique was used. After angioplasty the results were checked with repeated venographic procedure.
After removal of the balloon and hydrophylic sheath, haemostasis by manual compression was achieved. In our clinic no stents were used.
The surveillance protocol consisted of regular neurological examination at three monthly intervals and a final assessment of clinical disability by EDSS score after 12 months.
Quality of life was evaluated by a simple Visual Analogue Scale (VAS) by pointing the filling on a vertical 100 mm scale (range 0–100). The patient is asked to label on the line the point that best indicates her/his filling. A higher score is compatible with better life performance.
All patients included in the study were available at one-year follow-up.
Exclusion criteria included relapse in the previous three months, starting immunomodulatory or immunosuppressive treatment, the presence of another major disease, and patients with psychiatric symptoms or respiratory insufficiency.
Most of the patients had a limitation of gait and were transported to the clinic. After the endovascular procedure the patients spent the night in the hospital. On discharge, to avoid possible thrombosis, low-molecular-weight heparin (5000 IE) was prescribed for three weeks.
Re-stenosis was evaluated by the control sonographic method according to the described criteria.
Informed consent was obtained from participating subjects and with the agreement of the National Ethical Committee (authorization in 26 August 2010; the position number 36/08/10).
Statistical analysis
Parameters are expressed as mean values with standard deviation. The differences regarding age, the duration of the disease, disability and the number of venous lesions between the three MS groups were calculated using one-way analysis of variance. The relationship between the disability score and the degree of stenosis was assessed by Pearson correlation. A regression analysis was performed to assess the relationship between EDSS and the various parameters (age, duration of the disease, stage/course of the disease and number of venous lesions).
Results
Our study involved a total of 94 MS patients. In two patients (2.1%) CV examination did not reveal any vascular abnormality and the further results were therefore applied to the remaining 92 subjects.
The RR patient group – 14/22 (63.6%) were on immunomodulatory treatment – was significantly younger than the other two groups (P < 0.001). The duration of disease in the RR group was shorter than in the SP group (P < 0.001), but did not significantly differ in comparison to the PP group. The disability of the patients with the RR course of the disease was significantly lower than in the SP and PP patient groups (P < 0.001) (Table 1). The regression analysis showed that the duration of disease (beta factor 0.309; P < 0.003) and the stage/course of disease (beta factor 0.436; P < 0.001) are important parameters affecting clinical disability.
The simultaneous involvement of all three veins was observed in 31/92 (33.7%) cases. Stenosis of AZV was found in 48/92 patients (52.2%), while IJV was affected in all cases.
In two-third of cases there was bilateral involvement of IJV (65.2%). In the cases with unilateral jugular vein narrowing, the left IJV was more often affected (75%) than the right (25%). The distribution of neck vein involvement is described in Table 2.
Distribution of jugular vein stenosis
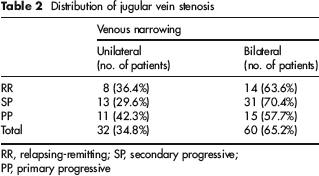
RR, relapsing-remitting; SP, secondary progressive; PP, primary progressive
The number of venous lesions is expressed as the number of any narrowing of a CV examined vein. The mean number of venous lesions in PP, SP and RR cases is shown in Figure 1.
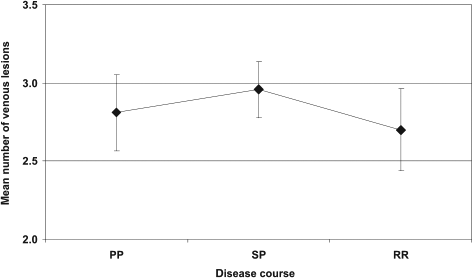
Mean number of venous lesions in three multiple sclerosis patient groups. PP, primary progressive; SP, secondary progressive; RR, relapsing-remitting
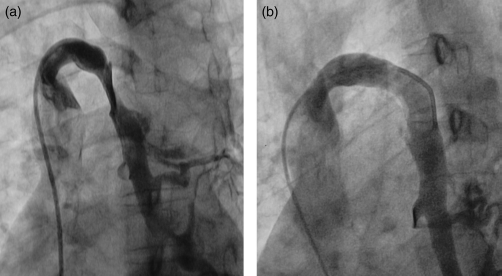
Figure 2 shows the abnormality of the IJV.

Venous pathology of the internal jugular vein: (a) membrane and (b) wall narrowing
An effective angioplasty is demonstrated in Figure 3.
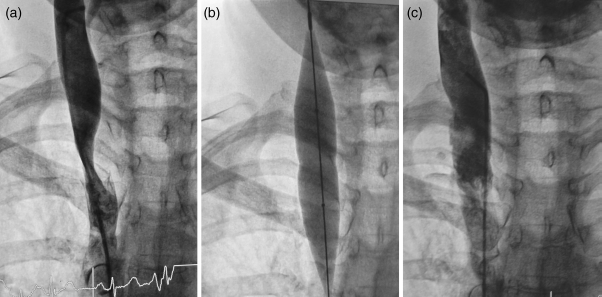
(a) Severe abnormality of the right jugular vein, (b) angioplastic balloon and (c) improved flow after dilation
After dilation of the tight annular stenosis by inflation of the removed angioplastic balloon, the deformity of the balloon with the impressions was observed (Figure 4).

Impressions of the removed inflated balloon
The successful dilation of the AZV is shown in Figure 5.
Stenosis of azygous vein (a) and lumen after dilation (b)
In the clinically severely disabled patients with an EDSS score of more than 6.0, the number of venous lesions was significantly higher (P < 0.005) than in patients with a lower disability score (Figure 6).
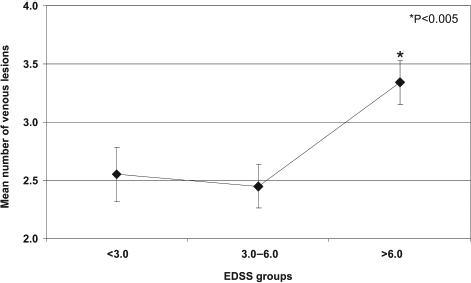
Expanded Disability Status Scale and number of lesions
In the RR group of patients, a significant improvement of clinical disability on the EDSS scale (Figure 7) was observed at 12 months (P < 0.001). An amelioration of ≥1.0 EDSS score in 10/22 (45%) of the RR patients was achieved. During the one-year period of follow-up, 3/22 (13.6%) of RR patients suffered clinical relapses. The strong correlation between EDSS and disease duration (r = 0.42; P < 0.001) and number of lesions (r = 0.253; P < 0.05) was observed.
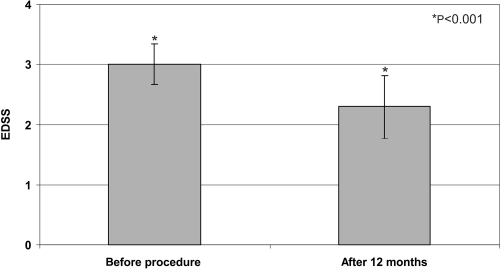
Amelioration of clinical disability (Expanded Disability Status Scale, mean±SD) in relapsing-remitting patients group
The improvement of the quality of life after one year of angioplasty is depicted in Figure 8.
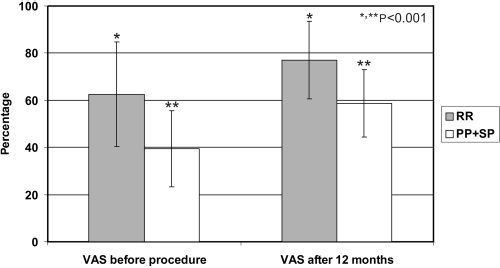
Assessment of quality of life after one year of the endovascular procedure (mean±SD). PP, primary progressive; SP, secondary progressive; RR, relapsing-remitting; VAS, Visual Analogue Scale
During angioplasty, haematoma – in two cases, both in the groin – in the region of the catheter placing was observed. In one case a small surgical procedure due to a disrupted angioplastic balloon in the groin was needed. The postoperative thrombosis in the IJV and deep veins was not found.
Discussion
In 92 of the 94 MS patients enrolled in the study (97.9%), with varying courses and disability, obstruction of the venous pathway was detected and angioplasty was performed. The neurological examination of two patients without any venous abnormality revealed mild clinical disability – EDSS less than 3.0 and the duration of disease was shorter than five years. The benign course of disease may explain the occurrence of normal venography. Similar results of the absent venous anomalies have been reported.13, 14 According to the proposed criteria, the preoperative vein changes were detected by extracranial and transcranial echo-colour Doppler protocol5, 6, 12 and confirmed by CV. There is no defined or exact non-invasive diagnostic screening method to rule out anomalies in the extracranial venous pathway. Some of the studies using sonography, phase-contrast magnetic resonance imaging and contrast-enhancing magnetic resonance angiography could not demonstrate the difference in the venous outflow between MS patients and healthy controls.15–18 By contrast, other authors have demonstrated the high sensitivity of extracranial Doppler sonography in demonstrating anomalies in the extracranial venous outflow.5,12,19–22 The best procedure to detect CCSVI is still undetermined, and it seems that the multimodal approach, including Doppler sonography, magnetic resonance venography, computed tomography venography, intravascular sonography and CV, is most appropriate at the moment.23–26
In one-third of patients, the simultaneous involvement of all three veins was observed (33.7%). In some cases, an extra soft stenosis not visible by CV was discovered during inflation of the balloon. To dilate severe annular stenosis – usually close to the inflated balloon – cutting wire was used. The deformity of the inflated balloon presenting after the removal from the vein supports the occurrence of the tight stenotic vein (Figure 4). Stenosis of IJV was found in all cases, while AZV was affected in around half of the patients (52.2%). This different involvement of the IJVs has already been reported in the literature13, 14 and the role of embryological development of these veins is discussed. 27 It seems that the venous lesions in IJVs are more important than the insufficient vertebrospinal venous system.
The mean number of venous lesions did not differ significantly in the three groups of patients, suggesting the occurrence of endovascular venous abnormalities even in the early course of the disease (Figure 1). This finding suggests that even in the patient group with an earlier disease course – the RR form of the disease – important vascular anomalies may develop. In our study, a statistically significant improvement (P < 0.001) of EDSS disability score in the RR group of MS patients (Figure 7) was achieved. In 45% of RR patients an improvement of ≥1.0 EDSS point was recorded. The demonstration of the venous obstacles in the RR group of patients supports the decision to use timely vascular intervention to prevent the development of multilevel vessel abnormalities and increased disability. The model of regression analysis showed the important role of disease duration and stage of disease in clinical disability, and an early treatment should be discussed.
After 12 months in patients with the progressive course of the disease 70/92 (76%) – the SP and PP groups – no changes in the disability was noticed.
A significant improvement in functional score in RR patients was recently reported. 28 Also the assessment of quality of life in our study group of patients – RR and progressive cases – using VAS, showed significant amelioration in both groups (P < 0.001, Figure 8). The improvement of quality of life in RR patients was higher than in the group of patients with the progressive course of disease (Figure 8). This finding corresponds to the lower disability of RR cases at the beginning of disease. The quality of life in patients is assessed by VAS and not by the validated MS questionnaires due to their different native languages. Benefits in physical and emotional conditions after endovascular treatment were recently reported. 29
Baracchini et al. 30 in 2011 reject the occurrence of venous disturbances in patients with the progressive course of disease. According to our findings (Figure 6), patients with greater disability – EDSS >6.0 – are inclined to develop a higher number of venous lesions than those with lower EDSS (P < 0.005).
From a strictly clinical neurological point of view, the endovascular procedure in more disabled patients with a need for constant bilateral assistance to walk is to be discussed. Neurologists are often focused on decreasing the number of relapses and slowing disease progression, whereas the patients – particularly with the progressive course of disease – often point out the importance of mental health and emotional factors. Nevertheless, in a severe long-lasting pyramidal lesion, an amelioration of functional neurological disability cannot be expected. Higher disability is usually a sign of the neurodegeneration with a less pronounced inflammatory phase of the immune process, leading to the deficient response of immunomodulatory drugs.2, 3 The degenerative phase of MS with higher disability score may favour the greater number of vascular anomalies. The disease duration and the disability are, namely, correlated with the number of vascular interventions.
The re-stenosis which occurred in 21.7% of patients was diagnosed by Doppler sonography.
The disadvantage of the study is the small number of patients. The clinical follow-up of patients was too short to allow us definite conclusion about the effectiveness of the endovascular procedure. However, the effect of angioplasty on the relapse rate and clinical disability of RR patients group, favour an early vascular treatment. The major shortcoming of our study is that it is not a blinded study. The follow-up MRI findings were only partially evaluated. The MRI evaluation presented recently in the multicentre study may corroborate the study findings. 28 The comparison of the RR patients group, treated with the immunomodulatory drugs, with the clinical outcome of patients who undergo pharmacological treatment and angioplasty, should be of great value in assessing the effectiveness of vascular treatment. A randomized blinded multicentre study to assess the role of CCSVI in MS is needed.
Conclusion
Many authors do not accept the CCSVI concept in the development of MS.7, 8, 9 Contrary, in many articles the role of the deficient venous drainage was emphasized.13, 14, 28 The association of genetic malformation and the number of venous malformations supports the venous role in the aetiology in MS. 31 Recently a lower annual relapse rate and clinical improvement in patients two years after angioplasty was reported. 32
The deficiencies in long-term immunomodulatory treatment endorse the search for additional factors which may contribute to the aetiology and ameliorate the therapy of MS. Our data suggest that early treatment for CCSVI may be beneficial, but more research is needed to support our recommendation.