
Abstract
Objectives
To determine whether bioimpedance spectroscopy was suitable for detection of hand lymphoedema.
Methods
The hands of 50 participants without a history of lymphoedema were measured with perometry and bioimpedance spectroscopy after positioning two ways for three minutes: (a) both hands rested at heart height and (b) the dominant hand at heart height and the non-dominant hand at head height. In addition, 10 women with secondary hand lymphoedema were also measured.
Results
Impedance and volume measurements were found to be strongly related (dominant hand r = −0.794). Both measurements were reliable (ICC2,1 = 0.900–0.967 and 0.988–0.996, respectively). Impedance was more sensitive to small changes in hand volume due to the postural change (position × device interaction: F = 23.9, P < 0.001). Finally, impedance measurements had better discrimination of women with lymphoedema than volume measurements.
Conclusions
Bioimpedance spectroscopy is a promising tool for the detection of secondary hand lymphoedema.
Introduction
Lymphoedema of the hand is a relatively common impairment following treatment for breast cancer. It is estimated to be present more than 60% of the time in women with secondary lymphoedema, 1 contributing to interference with daily activities and reduced quality of life. 2 To date, measurement of the volume of the hand has been a challenge due to the shape of the digits and palm of the hand. The ‘gold standard’ for the measurement of hand volume has traditionally been the water displacement method. The participant's hand is submersed in lukewarm water with the quantity of water displaced being equal to the volume of the hand. 3 Clinically, this measurement is not commonly used due to concerns about hygiene as well as difficulties in completing it accurately and quickly.4,5 An alternative strategy has been to derive the volume from hand circumference measures, taken either with a tape measure at 3 cm intervals 6 or with a perometer. 7
Water-displacement and circumference-based calculated volumes, such as perometry, are indirect measures of hand swelling as they measure the volume of all tissues including bone, muscle and fat. In conditions such as lymphoedema, the change in volume is primarily due to an increase in the quantity of extracellular fluid (ECF). In contrast to the other measurement approaches, bioimpedance spectroscopy (BIS) measures the quantity of ECF directly. At low frequencies, the quantity of ECF is inversely proportional to the impedance faced by the current. The ability to measure ECF specifically allows BIS to detect changes in ECF volume that occur in lymphoedema in the arm in the latent phase 8 and we propose, may also do so in the hand.
The primary aim of this study was to determine whether BIS can be used as an indicator of hand swelling, by detecting small changes in hand volume, when compared with perometry The second aim of the study was to determine the relationship between the measurements of the BIS and perometer. The third aim was to examine the reliability and validity of the BIS and perometry measurements. Finally, the utility of the measurement technique in a sample of women with lymphoedema of the hand was established.
Methods
Participants
A sample of convenience was used to recruit 20 males and 30 females without a history of swelling or lymphoedema. Control participants had a mean (standard deviation) age of 33.6 (15.2) years and body mass index (BMI) of 23.6 (3.3) kg/m2. All self-reported as being right handed. In addition, 10 women with hand lymphoedema secondary to treatment for cancer were recruited through lymphoedema clinics. All lymphoedema participants had been previously diagnosed by a lymphoedema therapist and treated using, at minimum, compression garments and lymphatic drainage massage for the hand. Lymphoedema participants had a mean age of 56.8 (14.8) years and a BMI of 28.4 (4.7) kg/m2 and swelling was present in their non-dominant hand for half of these participants. Participant characteristics for both groups are reported in Table 1.
Participant characteristics
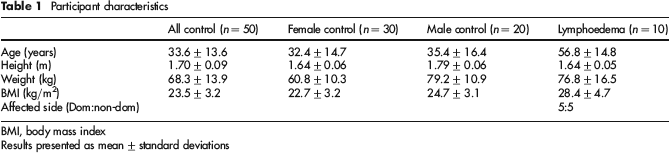
BMI, body mass index
Results presented as mean ± standard deviations
The Human Research Ethics Committee of the University of Sydney approved the study and all participants provided written informed consent before testing commenced.
Protocol for BIS and perometry measurements of the hand
Control participants attended the laboratory for a single measurement occasion in which both hands were measured. Height was measured to the nearest 1 mm and weight to the nearest 1 kg with the participant dressed in light indoor clothing with shoes removed. The participant's hand length, from the tip of the third finger to the ulnar styloid, and finger length, from the tip of the third finger to the third metacarpal-phalangeal joint, was measured using a non-stretchable tape measure. Participants were then seated, arms extended horizontally, with the hands and arms supported at heart height (from henceforth referred to as the horizontal position; Figure la) for three minutes during which time they were instructed not to move. Baseline BIS followed by perometry measurements were then undertaken on each hand. Following the completion of these measurements, the right hand was returned to the horizontal position while the left hand was held upwards at head height by elevating the arm to shoulder height and flexing the elbow 90° (referred to as the vertical position; Figure 1b). The arms were supported in these positions for three minutes. Previous research has shown that this position will lead to an immediate reduction in volume of the arm as measured by water displacement.
3
BIS measurements were then completed with the hands in this position. For the perometry measurements, as the design of the perometer precluded making measurements of the hand while in a vertical position, the left hand was quickly lowered to the horizontal and the measurement was completed within three seconds to minimize any fluid shift from the postural change. It has been previously shown that it takes one minute for approximately 50% of the volume change to occur with elevation
9
and it was assumed that the return of fluid would be similarly paced on return to the horizontal position.
Positioning of left hand for measurements, (a) Horizontal position: right and left hand placed horizontally, (b) Vertical position: right hand supported horizontally, left arm flexed vertically to 90°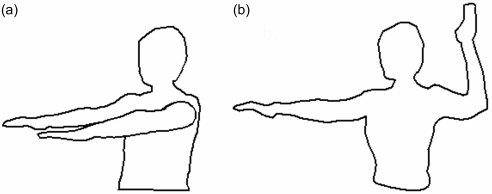
Participants with lymphoedema were measured in position 1 only.
Measurement methods
Measurement of the impedance of the hand
The volume of ECF in the hand was determined by BIS using an SFB7 impedance spectrometer (Impedimed Ltd, Brisbane, Australia). After cleaning the skin with an alcohol wipe, Ag-AgCl gel electrodes (Impedimed Ltd), cut in half lengthways, were placed immediately proximal to the nail bed on the third finger and on third metacarpal-phalangeal joint. Full-sized electrodes were placed in-line with the ulnar styloid and midway up the forearm. The volume measured by BIS using this electrode arrangement has been previously shown to be between the third metacarpal-phalangeal joint and the ulnar styloid, excluding the thumb. 10 BIS measurements were performed first on the right and then the left hand.
Hand volume measured by perometry
Hand volumes were measured with an optoelectrical perometer (Perometer, 1000M Juzo, Wuppertal, Germany) using the protocol previously described.
7
Briefly, participants were positioned in sitting with their left arm extended in front of them while the right arm remained in the supported position. The hand and forearm were centred over the central track and the end of the third finger was positioned against the front of the hand rest, modified to allow for measurement of the entire hand (Figure 2). The frame of the perometer was moved slowly along the track until it had reached the mid-forearm region and then was slowly returned to the starting position. The same procedure was then conducted with the right hand.
Positioning of the hand for the perometer measurements
The perometer measures the circumference every 4.7 mm. From these measurements, volumes of the segments are computed by the custom-modified Peroplus software™ (Pero-system, Wuppertal, Germany) using an algorithm known only to the manufacturer. Volumes are reported for contiguous 4 or 5 mm segments. These segmental volumes were then divided into 1 mm segments allowing the total volume of the hand to be computed accurately to the nearest millimetre by summation of individual 1-mm-segment volumes. To correspond with the bioimpedance measurements, only the volume of the body of the hand was considered. The body of the hand was determined to be from the end of the finger length measurement (the third metacarpal-phalangeal joint) to the end of the hand length measurement (the ulnar styloid). In contrast to the BIS measurements, volume measurements included the thumb.
Statistical analysis
Control participants
Control participants’ characteristics, impedance and volume data are presented as mean ± standard deviation.
The recorded impedance data files were uploaded to a computer and processed using the software supplied by the manufacturer (Bioimp v 5.2.4.0, Impedimed Ltd). Data were analysed in a manner analogous to that used for the assessment of unilateral arm lymphoedema. 11 For the control group, the impedance at zero frequency for the dominant side was expressed as a ratio relative to the non-dominant side. 12
To determine whether the BIS ratio differed significantly from the hand volume ratio, a two-way repeated measures analysis of variance (ANOVA) was undertaken with the within-subject variables of device (perometer versus BIS) and position (position 1 versus position 2). In addition, separate two-way repeated measures ANOVA were undertaken to assess the effect of position (horizontal, vertical) on each hand (dominant, non-dominant) for both impedance and volume. When significant interactions were identified, post hoc analyses were used to further explore where the significance lay.
To determine the extent to which the volume and BIS measurements were related, the volume of each hand was correlated with the impedance from that hand using Pearson's correlation. The agreement between the interhand ratios in position 1 was determined using limits of agreement analysis. 12
Reliability of the perometry and BIS measurements were examined by comparing the two measurement occasions of the stationary right hand using intraclass correlation analysis (ICC(2,1)). Finally, the bioimpedance and volume ratios in the horizontal position were compared with age, height, weight and BMI using regression analysis.
Lymphoedema group
The bioimpedance and volume data for the participants with lymphoedema are presented as median (interquartile range). The impedance and volume ratios were determined by comparing the affected to the unaffected hand as is done with whole-limb lymphoedema. 13 This was compared with the interhand ratios from the control group. As half of the lymphoedema group was found to have swelling in their non-dominant side, an interhand ratio for both the dominant and non-dominant side was determined for the controls.
Data were analysed using SPSS for Windows (version 19, IBM, Chicago, IL, USA), and Microsoft Excel (2007) (Redmond Washington).
Results
Controls
Two-way repeated measures ANOVA of the interhand bioimpedance and volume ratios revealed that while there was no significant difference between measurement devices (F = 0.46; P = 0.499), position was found to have a significant effect (F = 29.3; P < 0.001) and there was an interaction between the device and position (F = 23.9; P < .001). Further analysis revealed that the interhand impedance ratio (1.022 ± 0.072) was not significantly different from the interhand volume ratio when both hands were in the horizontal position (1.048 ± 0.079; t = −1.714; P = 0.09). With elevation of the left hand, however, the bioimpedance ratio (1.090 ± 0.072) was significantly different from the volume ratios (1.049 ± 0.073; t = 3.709; P < 0.001).
Two-way repeated measures ANOVA of the raw impedance values revealed that there was a significant difference for hand (F = 44.439; P < 0.001), position (F = 5.746; P = 0.020) and an interaction between hand and position (F = 38.099; P < 0.001). The impedance measurements significantly increased by 6.0 ± 9.4 Ω as a consequence of moving the left hand from the horizontal position to the elevated position (t = −4.647; P < 0.001). In contrast, the impedance for stationary right hand remained unchanged (−1.3 ± 6.8 Ω) between the two positions (t = 1.727; P = 0.09). Similar analysis for the raw volume measurements revealed a significant difference for hand only (F = 17.952; P < 0.001; position F = 3.572, P < 0.065; interaction F = 0.056, P < 0.814). Neither the left or right hand volume measurements significantly changed with the position change (right, t = 1.045; P = 0.301; t = 1.346; P = 0.184). The change in volume as a consequence of elevating the left hand was −1.3 ± 7.3 mL whereas it was −1.0 ± 6.9 mL for the stationary right hand.
Strong correlations were found between the impedance and volume measures for both the right and left hand in the horizontal position (r = − 0.794; r = −0.711, respectively; Figure 3). The interhand ratio determined by perometry was 0.03 (2.7%) larger than that determined from impedance measurements with limits of agreement of −0.24 to 0.18 (20.6%).
Correlation between the impedance and volume measurements for the control group. Open circles and dashed regression line represent dominant hand. Filled circles and unbroken line represent non-dominant hand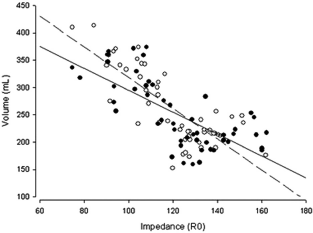
The stationary position of the right hand for both measurements allowed for the intrarater reliability of BIS and hand volume measures to be determined. The ICC(2, i) of the volume and impedance values for the right hand were very high, with those for the volume being slightly better (ICC(2,1) = 0.993, 95% confidence interval [CI]: 0.988–0.996 P < 0.001) than for the impedance measurements (right hand ICC(2,1) = 0.942, 95% CI: 0.900–0.967; P < 0.001).
Regression analysis revealed that weight, BMI and sex were related to the right hand volume (adjusted r2 = 0.859). In contrast, weight, BMI and age were all found to relate to the impedance of the right hand (adjusted r2 = 0.628).
Lymphoedema group
As the data for the lymphoedema group were not normally distributed, non-parametric analyses were used. The median (interquartile range) impedance ratio was 1.290 (1.116–1.642), whereas the median volume ratio was 1.125 (1.100–1.282). The bioimpedance and volume interhand ratios of the lymphoedema group were compared with the ratios determined for both the dominant and non-dominant hands of the controls (Figures 4a and b). Of the five participants with lymphoedema in their dominant hand, four were found to have bioimpedance ratios that were higher than the control group but only two for the volume measurements (Figure 4a). Of the five women with lymphoedema on their non-dominant side, four had bioimpedance ratios that were above the cut-off and all were above the control group for the volume measures (Figure 4b).
Comparison of interhand ratios between the lymphoedema participants (letters) to mean of female control groups (filled circles), (a) Dominant hand affected, (b) Non-dominant hand affected
Discussion
The aim of this study was to determine whether impedance, commonly used in the diagnosis of limb lymphoedema, is a better tool than perometry for measurement of hand lymphoedema. We found that while both BIS and perometry were able to similarly quantify interhand volume ratios in healthy participants when the hands were maintained in a resting horizontal position, BIS was more sensitive towards small changes in hand volume introduced by a postural change. As the reliability of both tools was shown to be high, we can be confident that the changes detected in the impedance measures were as a result of the shift in fluid from the postural change. In detection of lymphoedema, a tool that is able to detect small changes in fluid, particularly ECF, enables clinicians to diagnose sooner and therefore commence treatments before gross changes occur. This may reduce the impact on dexterity and quality of life which is often found with hand swelling. 2
Previous research has compared perometry and bioimpedance measurements in the upper limb. A strong correlation was found 14 but the relationship was not as strong as between other tools which both measure total limb volume. 15 This is to be expected as perometry and BIS are measurements of different components of limb volume and may explain the differences seen in the regression analysis. BIS measures ECF only whereas perometry measures total limb volume. To increase our understanding of the relationships between the tools, studies have used the theoretical assumptions behind bioimpedance measurements to extrapolate the bioimpedance results into volumes for both in the arm 16 and in the hand. 10 These studies have found remarkably close agreement between the impedance-derived and directly measured volume measurements for the total limb volume and palmar volumes.10,16 This relationship needs to be viewed with some caution, however, as a number of assumptions on the resistivity values are needed to complete the calculation from bioimpedance to calculated absolute volumes. To avoid these assumptions, the use of bioimpedance ratios is preferred.
Differences were seen between the impedance and volume measurements in the lymphoedema group. Overall, an impedance ratio above that of the controls was seen in eight of the women with hand lymphoedema, compared with seven for the volume measurement. Importantly, the interhand impedance ratios showed greater ability to discriminate than the volume measures which were mainly clustered above the upper end of the control group's results. Neither BIS nor perometry detected differences in the ‘at risk’ hand of one woman despite previous diagnosis and treatment for lymphoedema. This may reflect an incorrect diagnosis of lymphoedema based on transient swelling which has since resolved as has been previously reported.1,17,18 This use of BIS for hand measures will enable clinicians to detect changes in the dorsum of the hand that may not identified with measures of hand volumes.
Bioimpedance provides a novel way to diagnose and monitor lymphoedema of the hand as it is sensitive to small changes in fluid volume and has been shown to be reliable. While the changes from a baseline measure can be used to identify worsening or improvement of swelling, the cut-offs for confirmation of swelling, when baseline measures are not available, have yet to be determined. A three standard deviation above a control population's mean interlimb impedance cut-off has been adopted for upper limb lymphoedema13,19 and could also be considered for the hand. As the mean and variability of the interhand ratio of the control group were different from published means for the upper limb,13,19,20 currently used upper limb cut-offs are not appropriate. In development of new cut-offs specific to the hand, dominance as well as possibly age need to be considered as there was a significant difference in impedance between the dominant and non-dominant hand and age was found to be a significant factor in the regression analysis.
BIS was used to measure fluid in the palmar region of the hand. However, measurements of hand volume have typically included the fingers and thumb.3,5–7 For the majority of women with lymphoedema in this study, the palm was the region they reported to be affected with swelling. However, for women with swelling predominantly in the digits, this approach with BIS would not be appropriate. Exploration with BIS using narrowband electrodes of only a few millimetre widths may overcome this inability to measure the fingers.
Conclusion
In conclusion, the innovative use of BIS to assess swelling in the dorsum of the hand was found to be reliable, efficient and sensitive to small changes. Determination of cut-offs for diagnosis can now be developed taking into account limb dominance.
Conflict of interest: LW has consulted to ImpediMed Ltd. ImpediMed Ltd had no involvement in the conception and execution of this study or in the preparation of the manuscript.
Footnotes
Acknowledgements
ESD was supported by a biomedical postgraduate scholarship from National Health and Medical Research Council (Australia). SLK was supported by a career fellowship from the National Breast Cancer Foundation (Australia). We thank Mi-Joung Lee for comments on the manuscript and also thank all the participants who assisted with this research.