
Abstract
Objective
To evaluate the clinical and economical impact of a fast-track anaesthesia protocol in the management of primary varicose vein (VV) surgery.
Methods
Over a 10-month period (from 1 December 2009 to 30 September 2011), all patients eligible for open VV surgery (N = 176) were enrolled in a fast-track clinical pathway including titrated analgo-sedation combined with local anaesthesia. This fast-track cohort was compared with a historical cohort undergoing similar procedures and receiving general anaesthesia (GA) or spinal anaesthesia (SA) (between 1 December 2009 to 30 September 2011, N = 200). The length of stay in the operating facilities and postoperative recovery areas were reported and hospital costs were estimated. In addition, the occurrence of adverse events and unplanned hospital admission were compared between the two consecutive periods.
Results
Patients characteristics and surgical procedure were not different in the two cohorts. After implementation of the fast-track pathway, the incidence of postoperative adverse events decreased from 41% to 2.3%, with no need for overnight hospital stay (0% versus 7%). The reduction in anaesthesia-controlled time (-47%) and in postoperative recovery time (-61%) were associated with an increased operating capacity (1 extra case per day) and with substantial cost-savings (mean reduction of €312 per case, P < 0.001).
Conclusions
Implementation of a fast-track pathway for outpatient VV surgery was successful, safe and efficient. Analgo-sedation combined with infiltrative anaesthesia (instead of GA or SA) contributed to increase the operating capacity and to reduce the workload of nursing personnel.
Introduction
Despite the development of endovenous laser ablation, the evidence-based standard treatment of varicose vein (VV) remains the high ligation and stripping of saphenofemoral with concomitant avulsion of varicosities remains.1–3 A French survey revealed that these open surgical procedures were most frequently performed under general anaesthesia (GA) (83.9%) followed by spinal or epidural anaesthesia. 4 Alternative anaesthetic techniques involve the use of regional sciatic or femoral nerve blocks which are often time consuming, operator-dependent and less effective. 5 Infiltrative anaesthesia has also been advocated in carefully selected patients. 6
Although anaesthetic costs represent a relatively small component for each surgical episode, 7 the choice of anaesthetic techniques may greatly influence the total costs of the surgical episode by modifying the utilization of health-care resources. 8 In ambulatory surgery administration of short-acting anaesthetic agents for GA and application of regional anaesthetic techniques have been shown to speed up the postoperative recovery process while improving patient comfort and operating conditions.9,10 Using fast-track protocols, Williams et al. 11 showed that patients were deemed fit to bypass the postanaesthesia recovery unit (PACU) and to be cared for in areas that are less labour-intensive. Reduction in postoperative hospital stay result in true cost-savings if work productivity can be enhanced and/or if health-care professional are reallocated to other clinical tasks.12–14
Most studies comparing different anaesthetic techniques have been focused on time to extubation and time to fulfil criteria for being discharge from the PACU. 15 Perioperative care involves sequential processes that need to be explored when assessing the downstream effects of a new surgical or anaesthetic technique.
The aims of the current study were: (a) to implement a fast-track clinical pathway including titrated analgo-sedation combined with local anaesthesia (AS-LA) that allowed patient to bypass the PACU after open VV surgery; (b) to compare the duration of perioperative care processes and the incidence of postoperative adverse events over two consecutive periods, before and after shifting from a standard clinical pathway incorporating GA or spinal anaesthesia, to the fast-track clinical pathway including AS-LA.
Methods
Study subjects and settings
Prospective data were collected from all open VV treatment (saphenofemoral ligation, venous stripping and/or extensive phlebectomies) performed on an outpatient basis in adult patients (>18 years). We received approval from the institutional review board at the University Hospital of Geneva to examine the institutional database. Informed patient consent was waived given the retrospective analysis of an anonymized database.
Patient general management
On the day of surgery, fasted patients were admitted to the ambulatory surgical unit (ASU) and no premedication was given preoperatively. In the operating theater, a peripheral intravenous access was established and a 500 mL crystalloid infusion was commenced. Standard monitoring equipment included a three-lead electrocardiogram, non-invasive blood pressure, pulse oximetry and expired CO2 (via nasal sponge). One board-certified vascular surgeon carried out all surgical procedures and the same team of anesthesiologists (3 staff specialists supervising 8 rotating residents) delivered anaesthesia and perioperative care.
Ligations of the saphenofemoral confluence together with all tributary veins were performed through a small groin incision (1-2 cm). A stripper was inserted in the great saphenous vein and the vein stripped top down, either to just below the knee (in most cases) or to the ankle level (small skin incision, 4 mm), as deemed necessary. Phlebectomies of marked varicose branches and ligation of grossly incompetent perforators were performed simultaneously, whenever needed. The groin and distal incisions were closed by an intradermic continuous suture. Subcutaneous infiltration at each skin incision site were performed by the surgeon with a mixture of lidocaine 1% (1/3) and bupivacaine 0.5% (2/3), without dilution.
In the PACU and ASU, nurses evaluated pain scores using a visual analogue scale (VAS, 1-10) as well as adverse events. Besides checking vital signs and wound dressings, nursing interventions included the administration of antiemetic agents, vasopressors and morphine. Home readiness and the decision to discharge were made by the ASU nursing personnel, who were unaware of the purpose of the study.
Clinical pathways
Figure 1 shows the details of the two clinical pathways that were compared over two consecutive periods. The standard pathway had been originally designed by the vascular surgeon whereas the fast-track pathway was elaborated after preliminary feasibility tests and by a consensual discussion between the surgeons, anesthesiologists and nursing team. The surgical technique remained unchanged over the two study periods.
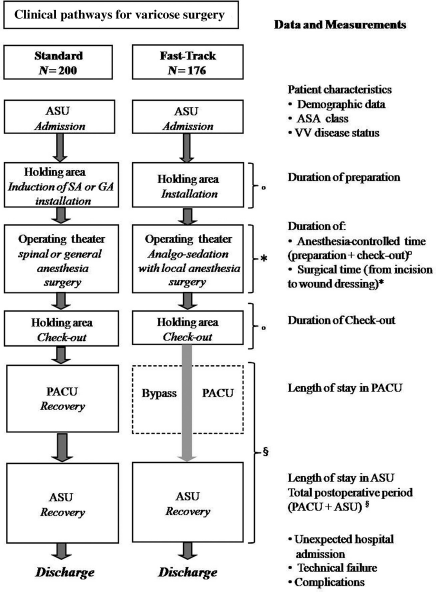
Consort flow chart describing the two clinical pathways for outpatient varicose vein surgery; PACU, postanaesthesia care unit
In the standard clinical pathway (historical cohort), surgical procedures were performed under GA or SA (depending on patient's choice) and all patients were admitted to the PACU and then transferred to the ASU step-down when they achieved a Modified Aldrete Score of ≥9 (see Table 1). For conducting GA, propofol was delivered intravenously via a target-controlled infusion (TCI) to achieve a predefined drug concentration and assisted or controlled ventilation was ensured via a laryngeal mask or an orotracheal tube. Repeated doses of sufentanil (5-10 μg per dose) were given to control nociceptive responses. In the SA, a single shot of hyperbaric bupivacaine 0.5% (7.5-12 mg) was injected intrathecally at the lumbar level.
Modified Aldrete Score
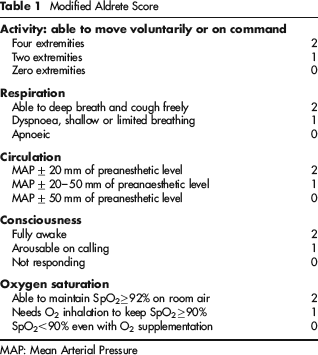
MAP: Mean Arterial Pressure
In the fast-track clinical pathway (fast-track cohort), surgical procedures were done under AS-LA. This therapeutic scheme was tested over three workday sessions and then implemented on 1, November 2009. The analgo-sedation regimen consisted in propofol and remifentanil delivered by TCI. Using two computer-driven infusion pumps, cerebral drug concentrations were targeted to achieve moderate level of sedation and to adjust analgesia according to the surgical stress while ensuring spontaneous ventilation, stable haemodynamics and satisfactory operating conditions. In addition, subcutaneous infiltration in the groin crease and island infiltration at sites of variceal avulsion were performed by the surgeon with a mixture of lidocaihe 1% (1/3) and bupivacaïne 0.5% (2/3). To achieve long-lasting analgesia, ketamine (5-10 mg) and a non-steroidal anti-inflammatory agent (ketorolac 30 mg) were co-administered intravenously before surgical incision. At the conclusion of surgery, low doses of morphine (1-2 mg) were slowly titrated if necessary to obtain VAS pain score less than 3/10. Patients achieving a Modified Aldrete Score of >9 were directly transferred from the OR (operating room) to the ASU until hospital discharge.
Measurements
Data were extracted from the hospital medical information systems and a dedicated institutional database including all open VV surgical procedure. Information was obtained regarding demographic and clinical variables, the surgical procedure, the anaesthesia-controlled time (added times of patient equipment, anaesthesia induction and awakening, end of surgery until discharge to PACU/ASU), length of stay in PACU and in ambulatory unit as well as the occurrence of any adverse events (nausea, vomiting, orthostatic hypotension, bradycardia, dizziness, hypoxemia or respiratory depression requiring intervention). Preoperatively, the status of VV was evaluated using the CEAP (clinical, aetiological, anatomical and pathological elements) classification and the VCSS. Before hospital discharge, patients in the fast-track cohort were asked if they would (or not) undergo surgery under the same anaesthetic regimen.
The hospital costing system was used to estimate the costs of each operative procedure by taking into account the salaries, drugs as well as disposable equipments. Overhead costs (e.g. administration, building operating expenses) were assumed constant in the two periods and were therefore ignored. The salaries were obtained from pay-roll information and, costs in human resources were considered being dependent on the time spent by health-care professionals at each process. Costs expressed in Swiss Francs were converted into Euros.
The primary endpoint of the study was the time from the end of surgery until achieving the eligibility criteria for hospital discharge (postoperative recovery time). Secondary outcomes included the anaesthesia-controlled time, the occurrence of any adverse event, the length of stay in the PACU and ASU, re-admission in the hospital, costs associated with each anaesthetic technique.
Statistical analysis
Based on our own data (postoperative recovery time of 8 [3.4] hours), a power calculation indicated that 134 patients per group would be needed to detect a 20% reduction of recovery time after implementation of the new clinical pathway with a power of 90% and an α-error of 5%. Taking into account 20% dropouts (incomplete data, contraindications for analogue-sedation), a minimum of 350 patient's files (175 in each group) were included.
The statistical significance of differences between the cohorts was evaluated by two-way repeated measures analysis of variance and t-test with Bonferroni correction. Otherwise the comparisons of skewed data were performed by Mann-Whitney rank sum test. Chi-squared tests and Fisher's exact probability tests were used as appropriate for comparison between the groups of categorical data. Values were expressed as mean (SD) unless otherwise stated. Statistical significance will be assumed for P < 0.05.
Results
The historical cohort included 200 patients, operated from 1 December 2009 to 30 September 2011 (100 cases under GA and 100 under SA). The fast-track cohort comprised 176 patients operated from 1 November 2010 to 30 August 2011. As shown in Table 2, the two cohorts were comparable regarding demographic variables, ASA classes, VV disease and the extent of surgery (uni- or bilateral procedure). The volume of local anaesthesia administered was 17 ± 7 mL (ranging from 6 to 30 mL) without group differences.
Demographics for patients undergoing varicose vein surgery following two different clinical pathways, standard or fast-track
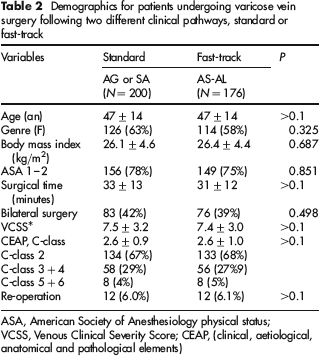
ASA, American Society of Anesthesiology physical status; VCSS, Venous Clinical Severity Score; CEAP, (clinical, aetiological, anatomical and pathological elements)
In the fast-track cohort, all procedures were successfully completed under AS-LA without need for converting to GA with tracheal intubation; manual-assisted ventilation was deemed necessary in two patients over a brief period (less than 3 minutes).
All patients in the fast-track cohort were transferred from the OR directly to the ASU and the postoperative recovery time was significantly shorter than in the historical cohort, the mean difference was 364 minutes (Figure 2). Although surgical duration was similar in the two groups, the anaesthesia-controlled time was significantly reduced in the fast-tracked cohort (mean – 22 minutes per case, compared with standard group) and allowed one additional procedure to be planned within an allotted eight-hour OR session.
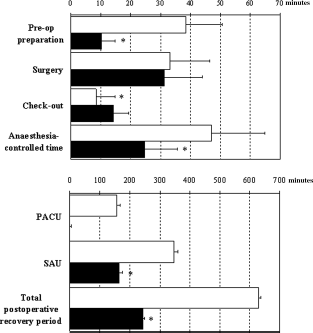
Durations of intraoperative (upper graph) and postoperative (lower graph) processes are compared between the historical (□) and fast-track (▪) cohorts. Anaesthesia-controlled time represents the sum of preoperative preparation and check-out times; data are expressed as mean (standard deviation); *P< 0.05 between historical and fast-track cohorts
As shown in Figure 3, the incidence of postoperative adverse events decreased from 41% in the standard cohort to 4.4% in the fast-track group (P < 0.01). The need for complementary analgesic treatment in the ASU also decreased from 26% in the standard cohort to 2.3% in the fast-track cohort. All patients, except one, were satisfied regarding the anaesthetic management and declared that they would accept the same anaesthetic plan for future surgical procedures.

Incidence of early postoperative complications related to anaesthesia (upper graph) and to surgery (lower graph). *P < 0.05 between the two clinical pathways historical (□) and fast-track (▪) cohorts. *P < 0.05 between historical and fast-track cohorts
Fourteen patients in the standard cohort (7%) did not fulfil the criteria for being discharged from the ASU and required overnight hospital admission (9 with nausea/vomiting and dizziness, 3 with headaches and 1 with orthostatic hypotension). In contrast, all fast-tracked patients could be discharged home on the day of surgery. The incidence of surgical complications was similar in the two cohorts.
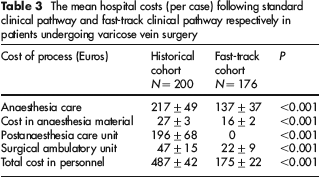
The mean hospital costs (per case) in the fast-track cohort was €312 lower than in the standard group (P < 0.001; Table 3).
The mean hospital costs (per case) following standard clinical pathway and fast-track clinical pathway respectively in patients undergoing varicose vein surgery
Discussion
In this observational study implementation of AS-LA instead of standard anaesthetic techniques (GA or SA) allowed all patients to safely bypass the PACU after open VV surgery. This fast-track clinical pathway resulted in shorter postoperative recovery time (– 61%), fewer anaesthetic-related adverse events with no need for overnight hospital admission and important cost-savings (– €312 per case).
Currently, open VV surgery can be safely performed as a day case procedure as far as suitable anaesthetic techniques providing pain relief with minimal side-effects are applied.16,17 Moderate pain after ambulatory procedures has been reported in up to 25% of patients in ambulatory surgery 18 Besides unsatisfactory pain relief, excessive sedation, nausea and vomiting (10-30%) after GA or orthostatic hypotension (5-10%) and urinary retention after SA may complicate the postanaesthetic recovery period, resulting in prolonged stay in recovery areas and even unplanned overnight stay.19–21
In fast-tracked patients, intraoperative analgo-sedation entailed the dual titration of intravenous propofol and remifentanil using an automated delivery system allowing the anaesthetist to target a cerebral drug concentration corresponding to a predetermined hypnotic or analgesic effect. Among short-acting hypnotic and anaesthetic agents, propofol has emerged as a drug of choice for managing sedation given its excellent safety profile, rapid onset and offset of action as well as anxiolytic and antiemetic effects. 22 Likewise, remifentanil, an ultra-fast opiate is best suited to control intraoperative noxious stimuli while providing faster recovery with the least impact on respiratory control, compared with fentanyl or sufentanyl. 23 With the TCI delivery system, better prediction of drug effects was achieved since the administration of propofol and remifentanil was driven by microprocessor-controlled algorithms based on well-validated pharmacokinetics models. 24
In addition to remifentanil, perioperative pain was successfully control by infiltration anaesthesia and co-administration of a nonsteroidal anti-inflammatory drug and ketamine, a N-methyl-
Providing a safe environment and the best medical care are top priorities in OR management. Caring for all scheduled patients and maximizing OR efficiency is also important goals guiding OR operational decisions. 28 Implementation of the AS-LA protocol was associated with better clinical care as reflected by patient satisfaction and fewer anaesthetic-related side-effects. Moreover, the fast-tracking strategy induced two positive economic consequences: (1) increased OR turnover owing to reduced anaesthetic-controlled time, (2) cost-savings related to reduced utilization of nursing personnel in the postoperative period.
This study included a homogeneous group of short-lasting procedures (mean duration of 32 minutes) with small variability in operator controlled time (SD 13 minutes). Consecutive VV cases were scheduled in a single OR suite (eight hours workday) by a coordinating manager and fixed staffing of anaesthesia and nursing personnel was allocated to the OR suite. Accordingly, activity-based costs were expected to decrease if the OR turnover increased while staffing remained similar. In the fast-track clinical pathway decreasing the anaesthesia-controlled time by 22 minutes enabled the OR manager to schedule one extra case per session (7 or 8 cases instead of 6 or 7). Indeed, the AS-LA protocol led to simplification of the anaesthetic processes that were entirely and rapidly performed in the OR. In contrast, with the standard anaesthetic techniques, additional time was needed for anaesthesia induction and emergence, airway instrumentation, adjustment of ventilatory support, as well as for dural puncture and checking the adequacy of spinal anaesthetic blockade.
Finally, the adoption of the AS-LA protocol decreased the postoperative nursing workload and accelerated the discharge time. Although the time saved in the ASU and in the PACU were almost equivalent (mean reduction of 182 minutes versus 157 minutes), labour cost-savings in the fast-track clinical pathway were predominantly attributed to bypassing the PACU. Indeed, costs related to PACU stay are almost similar to that in the intensive care unit, given the high density of human resources necessary for managing patients recovering from anaesthesia over a short period of time. Despite bypassing PACU, all AS-LA patients required fewer postoperative nursing interventions in the ASU for treating pain or anaesthetic related side-effects and none of them required to stay overnight.
If we extrapolate estimates of these individual cost-savings to an annual rounded number of 300 outpatient VV procedures, global cost-savings in our institution would approximate €133,600 after converting our anaesthetic practice from GA/SA to AS-LA. Additional cost reduction would be expected by avoiding unplanned hospital admission (€22-28,000 per year). Similar cost-savings have been reported in patients undergoing cruciate ligament reconstruction after implementation of regional analgesia in knee surgery that resulted in faster anaesthesia emergence and better pain control allowing most patients to bypass the PACU. 29
We acknowledge several limitations in this study. First, this study was conducted in a single teaching hospital, thereby limiting its applicability in community hospitals, office-based practices or ambulatory surgical centres. Second, bypassing the PACU could have been achieved in some patients in the standard cohort. However, we adopted the American Society of Anaesthesiology standards that recommend that all patients receiving anaesthesia care (GA or regional blockade) should be admitted to a PACU. 30 Third, although a randomized blinded trial may provide stronger scientific evidence to assess specific intervention or drug effect, comparison of two clinical pathways involving multimodality processes would have been difficult to set up in the constraints of our ambulatory surgical unit. Fourth, the improved profitability incurred by the fast-track clinical pathway was not addressed since salaries of physicians and nurses were fixed rather than time dependent and the reimbursement policy was based on a flat fee (capitation) and did not reflect the real expenses of perioperative care.
Our data demonstrate the potential for reducing workload and labour costs, maximizing work efficiency in the OR and improving quality of care by de-emphasizing the use of standard anaesthetic techniques and adopting instead innovative protocols such as titrated analgo-sedation combined with infiltrative anaesthesia. A team approach to educational and clinical interventions along with providing feedback to clinicians regarding patient and process outcomes were key factors for successful implementation of a paradigm of perioperative care practice.