
Abstract
Objectives
Chronic cerebrospinal venous insufficiency (CCSVI) is a malformative condition characterized by several anomalies of the azygos and/or internal jugular veins (IJVs). Recommended diagnosis of CCSVI is performed with colour-Doppler (CD) sonography. Though catheter venography (CV) is considered as the gold standard for determining vascular anatomy, its uniplanar point of view does not allow an overall evaluation of endoluminal structures. This limit could be addressed by intravascular ultrasound (IVUS). The aim of this report is to evaluate, in patients with multiple sclerosis (MS), the accuracy of CD sonography and CV versus IVUS in estimating the diameter and the cross-sectional area (CSA) of the IJVs and in detecting jugular endoluminal malformations (JEM).
Method
Forty-five MS patients with CCSVI, diagnosed by CD sonography, were submitted to CV during IJVs angioplasty. Twenty-five subjects were also examined with IVUS. The IJVs maximum diameter (MAXD) and CSA were estimated. CD and CV data were compared with IVUS data with the Bland-Altman method.
Results
The mean difference in IJV MAXD recorded by CD and IVUS was —0.5 mm. The mean difference in IJV MAXD recorded by CV and IVUS was 3.36 mm. The mean difference in IJV CSA recorded by CD and IVUS was —11.2 mm2. JEM recorded by IVUS were detected by CD sonography and CV with 88% and 32% accuracy, respectively.
Conclusions
CV was significantly inferior to CD sonography and IVUS in detecting JEM. Differences between IVUS and CD sonography in detecting JEM and in quantifying jugular diameters were not significant. The IJV CSA was underestimated by CD sonography compared with IVUS. CD sonography was proven to be important in the anatomical characterization of CCSVI, providing useful information for correct intravascular treatment.
Introduction
Chronic cerebrospinal venous insufficiency (CCSVI) is a congenital vascular malformative syndrome that is prevalently characterized by valvular alterations (e.g. spur, vein web, annulus, inverted flaps or septum) involving efferent cerebral vascular districts (azygos and/or internal jugular veins [IJVs]), with preferential involvement of the proximal segments (jugular-subclavian joint, azygos-caval outlet). The obstructed normal venous output entails activation of additional circles (condylar veins, pterygoid plexus, thyroid veins and anterior and external jugular veins) as the result of increased lateral pressure along the principal drainage pathways. 1 Somehow, extracranial venous obstruction and stenosis are associated with cerebral pathophysiology, especially with venous pressure, perfusion and cerebrospinal fluid dynamics. 2 The particular feature of CCSVI-related cerebral venous blood flow disorders, along with the histology of perivenous spaces and recent findings from advanced magnetic resonance (MR) imaging techniques, underpin the hypothesis that iron deposits in multiple sclerosis (MS) are a consequence of altered cerebral venous return and chronic insufficient venous drainage. 3 Coen et al. 4 showed that extracranial vein lesions of MS patients are characterized by a ratio of collagen type I/III that is similar to that observed in fibrotic lesions but does not contain myofibroblasts, thus suggesting a local malformative pathogenesis rather than a fibrotic one; these results were confirmed by collagen type I and III immunohistochemistry Combined transcranial and extracranial colour-Doppler (CD) allows for non-invasive measurement of venous haemodynamic parameters indicative of CCSVI. 1 The five criteria are as follows: (1) the presence of reflux in the IJV and/or vertebral veins in both postures or reflux in one posture and absence of flow in the other; (2) the presence of reflux in deep cerebral veins (‘additional’ criterion); (3) high-resolution B-mode evidence of proximal IJV stenosis and/or other B-mode anomalies; (4) the absence of detectable flow in IJV and/or vertebral veins in both postures and (5) the presence of reverted postural control of the main cerebral venous outflow pathway by measuring the difference in the cross-sectional area (CSA) of the IJVs in the supine and sitting positions. Diagnosis of CCSVI requires at least two of the five criteria to be fulfilled (Table 1).1,2,5 Interest in CCSVI is surely related to its correlation with MS (mean 62.5%; N = 289), and it is much less prevalent in healthy controls (mean 22.5%; N = 163). 6 In addition, Bastianello et al. 7 reported a strong association between CCSVI and a particular MS phenotype (greater age and clinical severity in CCSVI-positive patients). Based on such evidence, venous angioplasty of IJVs and of the azygos vein was proposed to improve obstructed venous outflow. 8 Early reports by Zamboni et al. 8 describe high rates of clinical improvement in patients with MS after angioplasty of stenotic azygos and IJVs. The above-mentioned study underscored a significant reduction in the relapse rate during the first year after venous balloon angioplasty, and intravascular treatment significantly improved the outcome recorded for MS. Treatment of azygos and IJVs recorded a one-year patency of 95% and 70%, respectively. 8 Other recent studies have confirmed the safety and low procedural risk of the procedure, which has a 1.2% incidence of venous thrombosis. 9 Intravascular treatment also improved the quality of life among mid-term follow-up patients. 10 The venous angioplasty procedure was performed in patients with a diagnosis of CCSVI ascertained by CD sonography of efferent cerebral vessels and of deep cerebral veins. The intervention is perfected based on anatomical information of the internal jugular districts, of the correlated compensation circles and of the azygos vein, which are obtained by catheter venography (CV). However angiography provides a monodimensional view of blood vessels and thus does not allow an accurate morphological assessment of venous malformations due to the obstructed outflow. These malformations are the principal target of endovascular therapy. Recently Diaconu et al., 11 utilizing dissected cadaveric veins, showed that the anatomy of the venous system has significant variability, including a differing number of valves in different regions and variable characteristics of the valves. The average vein circumference was less than that typically reported in imaging studies of live patients. Data obtained from such investigation include a morphological luminal view of IJVs that records, if required, any reductions in the calibre of the various segments and provides only a qualitative assessment of venous outflow. The same considerations apply to MR venography, which has been shown to have poor sensitivity in identifying endoluminal structural and functional anomalies but has very good sensitivity in detecting collateral circles. 12 Hence, the decision was made to improve this limit by combining intravascular ultrasound (IVUS) and angiographic investigation for direct morphological assessment of IJVs. In fact, IVUS provides an overall assessment of the vessel section and an independent analysis of the projection angle. This translates into greater accuracy in the assessment of anatomical structures because the direct image provides a tomographic view of venous structures. Catheters currently available for intravascular sonography are able to view structures with a diameter up to 24 mm and with excellent resolution. This allows investigators to study the jugular venous district with extreme precision, also through concurrent longitudinal reconstruction of the vessel.13,14 The aim of this study was to use IVUS in order to measure the accuracy of CD sonography and catheter venography (CV) for the detection of jugular endoluminal malformations (JEM) and for the estimate of the diameter and CSA of the IJVs in MS patients with CCSVI treated by venous angioplasty.
Five Zamboni's criteria
IJV, internal jugular vein; CSA, cross-sectional area
Methods
Forty-five MS patients with CCSVI were treated by IJV angioplasty at our cardiovascular laboratory of interventional radiology and haemodynamics. Table 2 reports the clinical features of subjects. The MS-related disability status of these patients was evaluated by means of the Expanded Disability Status Scale (EDSS scale). The decision to perform the percutaneous transluminal angioplasty (PTA) was taken after the diagnosis of CCSVI, using the presence of at least two of the Zamboni's criteria at CD sonography. The site of the dilation was later confirmed by CV and, when performed, by IVUS. This was a pilot study belonging to a more ambitious multicentre, randomized, controlled study that obtained IRB approval. Written informed consent for the angioplasty procedure was obtained from all patients.
Patient characteristics (n = 45)

EDSS, Expanded Disability Status Scale; VHISS, Venous Hemodynamic Insufficiency Severity Score; CCSVI, chronic cerebrospinal venous insufficiency; RRMS, relapsing remitting multiple sclerosis; SPMS, secondary progressive multiple sclerosis; PPMS, primary progressive multiple sclerosis
Venous zones are three: right internal jugular, left internal jugular and azygos. The CCSVI score ranges from 1 to 5, corresponding to the number of criteria met. The VHISS score range from 1 to 16, with higher values corresponding to more venous insufficiency
Echo-colour and transcranial colour-coded Doppler sonography examination techniques
Cerebrovenous haemodynamics was performed by an expert vascular sonographer with a colour Duplex scanning (MyLab Vinco US System, Esaote S.p.A., Florence, Italy) equipment fitted with two transducers with operating bandwidth 3-11 MHz (imaging frequencies: 3.5-5.0-6.6-10.0 MHz; Doppler frequencies: 3.3-5.0 MHz) and 1-4 MHz (imaging frequencies: 2.0-2.5-3.3 MHz; Doppler frequencies: 1.6-2.0-2.5 MHz). Morphological and functional characteristics of both IJVs and VVs were investigated in subjects placed in supine (0°) and upright sitting (90°) positions. The same positions were used to examine deep cerebral veins. CCSVI was diagnosed based on two of five positive Zamboni's criteria (CCSVI score). A proper electro-mechanical tilting chair was used to maintain resting conditions of the subject as much as possible (without voluntary muscle movements and contractions) when changing position. Adequate hydration of the subject during the 12 hours prior to the examination was recommended. A proper head support was used to ensure that the neck was neither hypo-extended nor hyper-extended and to prevent it from turning either to the left or to the right side. A pillow was placed on the subject's thorax for the sonographer to lean his elbow on; this feature was particularly useful when the subject was in a sitting position. Maximum diameter (MAXD – mm) of the IJV lower segment near the jugular-subclavian joint (J1) and CSA of the IJV middle segment viewing the thyroid gland sideways (J2) were computed for all supine patients. Continuous trace method (mm2) was used for the computation of CSA, referring to the greatest ellipse calculated at the end of the expiration phase.
Catheter venography
Procedures were performed in an angiographic suite (GE Innova 2100). Patients were positioned supine with a pillow under the head to prevent rotation of the neck. Patient monitoring included continuous electrocardiogram recording, and pulse oximetry and arterial pressure were measured in the arm (at 5-minute intervals). All procedures were performed under local anaesthesia, and no adrenaline was added. The contrast dye used was Iodixanolum (Visipaque 300w, Amserham Health As, Oslo, Norway), and injections were mechanically administered with the ACIST™ injection system. Angiographic access was achieved through the left or right common femoral vein. Catheterization with a 5 Fr sheath (Terumo) was performed and replaced with a 9 Fr sheath prior to PTA. A 5 Fr vertebral angiographic catheter (Terumo) was placed at the origin of the IJV, and the first injection (10 mL-5 mL/second) was performed to assess the anatomy and possible activation of collateral pathways for intracranial or extracranial drainage. The catheter was pulled back into the jugular bulb, and a second injection was administered (10 mL-5 mL/second, ipsilateral oblique projection 30-45°) to assess junction anatomy, valve morphology and the presence of anomalies. If required, selective catheterization of collateral veins was performed (e.g. external jugular vein, common facial vein and thyroid vein) to clarify anatomical and drainage patterns. Maximum IJV diameter was assessed in all patients at point J1 with the measurement software GE Innova 2100. The CV was performed by an interventional cardiologist informed only on the positivity of Zamboni criteria of CCSVI and on the side of jugular vein affected by flow alterations.
Intravascular ultrasound
Twenty-five patients enroled in this study (55.5%) were also examined with the IVUS method (Vision PV electronic catheters 3.4 Fr – Volcano Corporation, CA, USA) both before and after angioplasty. IVUS was proposed to patients with milder disabilities and who were more likely to accept a longer examination. Intravascular images were obtained by manually pulling back the IJVs from points J3 (upper segment above the carotid bifurcation) to J1 (lower segment near the jugular-subclavian joint), referring to the relevant venograms. The CSA of IJVs in point J2 and the maximum diameter in point J1 were thus measured. CD data were compared with IVUS by simplifying morphological analysis to the following jugular alterations: malformed valve (dysdynamic or fibrous valve), septum (thin linear echogenic structure that extends from the endothelial lining of the vein wall and is attached to it at both ends), membrane (membranous structure almost occluding the entire diameter of the vein), flap (thin linear echogenic structure extending from the endothelial lining of the vein wall), annular stenosis (CSA <3 mm2) and web veins (multiple septa and flaps located in a cluster).
Immediate and mid-term endovascular treatment evaluation
The immediate success post-venoplasty was angiographically assessed by a qualitative assessment of the increase in the outflow of the treated jugular vein and, in patients who underwent IVUS, with the measurement of the CSA post-PTA. The evaluation of CCSVI and Venous Hemodynamic Insufficiency Severity Scores (VHISS) was performed at one, three and six months using CD sonography. Data from these assessments will be presented in a forthcoming publication.
Statistical analysis
Continuous variables are described as means and standard deviations (SD), while counts and percentages are used to describe qualitative variables. Measurements obtained with the three different methods were compared with the Bland-Altman method 15 to assess the bias (mean difference) and variability (SD of the differences) of CD sonography and CV compared with IVUS. To do the Bland-Altman plot, we have computed the differences and the means between the measurements obtained with two diagnostic methods. The difference of the paired two measurements is plotted against the mean of the two measurements. When the differences were not constant (Figure 2), i.e. with a non-random arrangement of the points, the absolute differences have been converted into percent differences of the averages, but the figure with actual values in mm on the y-axis has been supplied for comparison. The mean difference, also called bias, represents the mean error, namely the average quantity that the second measurement adds to or subtracts from the first one. The diagnostic accuracy of CD sonography and CV compared with IVUS for the detection of JEM was expressed as sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and accuracy. Precision of the diagnostic parameters was presented using a 95% confidence interval. P values below 0.05 were considered significant. The statistical analyses were performed using SPSS software (version 14.0, SPSS Inc., Chicago, IL, USA).
Results
From December 2010 to March 2011, 45 MS patients with CCSVI were treated with venous angioplasty after IJV CD sonography and CV investigations. The disease course was relapsing-remitting in 19 patients (42.2%), secondary progressive in 20 patients (44.4%) and primary progressive in six patients (13.3%). The mean EDSS score was 5.4 (range, 1-9). The patients’ features are summarized in Table 2. Twenty-five patients were also examined with IVUS. MAXD and CSA (means ± SD) of IJVs are reported in Table 3. No perioperative treatment-related complications were observed. There was a good degree of agreement between the measurements obtained with the three different methods. The mean difference in the measurement of the IJV diameter between CD sonography and IVUS was -0.56 mm (95% CI from -0.854 to – 0.266 mm) (Figure 1). The mean difference in the measurement of the IJV diameter between CV and IVUS was 3.36 mm (95% CI from 2.754 to 3.966 mm) (Figure 2). The mean difference in the measurement of the IJV area between CD and IVUS was -11.2 mm2 (95% IC from -13.19 to -9.21 mm2) (Figure 3). Endoluminal malformations detected with IVUS were revealed by CD sonography with 88% accuracy (SENS 94%; SPEC 78%, PPV 88%, NPV 88%) and by CV with 32% accuracy (SENS 6%, SPEC 78%, PPV 33%, NPV 32%) (Table 4).
Quantitative analysis of IJVs (n = 25)

CSA, cross-sectional area; IJV, internal jugular vein; IVUS, intravascular ultrasound. The table contains mean values and SD. It can be noted a good concordance between CD and IVUS especially for diameter
Detection of valvular malformations by IVUS (n = 25)

TP, true positive; TN, true negative; FP, false-positive; FN, false-negative; between brackets: 95% CI; CD, colour-Doppler; CV, catheter venography; IVUS, intravascular ultrasound. IVUS is assumed as the gold standard
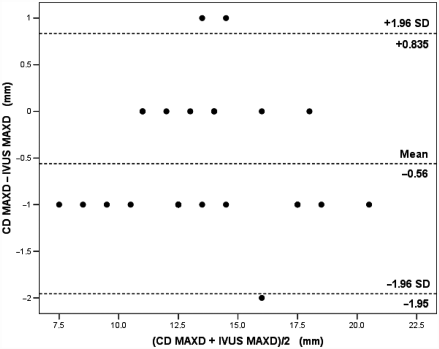
Bland-Altman plot of maximum IJV diameter recorded by CD (CD MAXD) and maximum IJV diameter recorded by IVUS (IVUS MAXD). IJV, internal jugular vein; IVUS, intravascular ultrasound; CD, colour-Doppler

Bland-Altman plot of maximum IJV diameter recorded by CV (CV MAXD) and maximum IJV diameter recorded by IVUS (IVUS MAXD). IJV, internal jugular vein; IVUS, intravascular ultrasound; CV, catheter venography
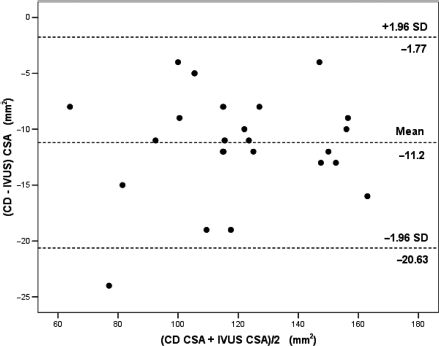
Bland-Altman plot of measurements of the IJV cross-sectional area recorded by CD (CD CSA) and by IVUS (IVUS CSA). IJV, internal jugular vein; IVUS, intravascular ultrasound; CD, colour-Doppler
Discussion
The recent use of angioplasty to treat IJVs in patients with CCSVI has revealed a complicated and varied disease. 16 Preliminary CD sonography provides a large amount of morphological and haemodynamic information about jugular veins for accurate operative planning. CD scanning extracts essential data for planning angioplasty in patients with a CCSVI diagnosis based on the five criteria of Zamboni, namely IJV diameter at the J1 (lower segment near the jugular-subclavian joint), J2 (middle segment with the thyroid gland viewed sideways) and J3 (upper segment above the carotid bifurcation) levels, the cross-sectional area of IJV at point J2, and the CSA variability between supine and sitting positions. There remains an open discussion on the ability of CD sonography to identify JEM because the ultrasound investigation of intracranial and cervical veins is highly operator dependent due to the wide anatomic and physiological variability of these vessels. 17 To address the problem of standardization Zamboni et al. have proposed a consensus document with some recommendations for a common protocol to apply to CD sonography that should reduce the variability of results obtained from different study centres. 18 Recognition of jugular sizes, anatomical site and the type and extent of lesions allows for the detection of the exact sites of dilation to choose the correct size of dilation catheters. Hence, the operator will have an overall anatomical view to be taken into account during the procedure. Therefore, angioplasty will be executed by selection without causing inappropriate mechanical stress to normal venous segments, thus reducing potential PTA-related involvements. This study compares the information obtained with CD sonography with information obtained with CV during venous angioplasty also using IVUS in 55.5% of cases, to improve the anatomical assessment of the jugular district, which was the site of percutaneous treatment. Data analysis underscored the fact that CV significantly underestimates the IJV diameter compared with CD and IVUS, as could be extensively predicted based on the known limits of the method. 19 CD sonography instead, provides a very precise measurement of the IJV diameter, with a mean underestimation of 0.56 mm compared with IVUS. This minor difference has no effect on endovascular therapy in terms of choice of dilation catheters. With CD sonography the possibility of having a reliable measure of the diameter of the jugular vein at multiple locations allows the exclusion of forms of hypoplasia of the jugular vein that if treated with PTA can more frequently result in thrombotic occlusion on the one hand, and on the other hand, allows the clinician to choose the correct diameter of the dilator catheter, which is the first and most important step of the PTA procedure. The ease and rapidity of measurement of the diameters of the jugular veins obtained with CD sonography allows its use on the operating table before and during the PTA. CD sonography underestimates IJV CSA compared with IVUS (mean difference: 11.2 mm2). These data are clinically important because evaluation of the IJV luminal area both before and after angioplasty could be the only objective way of assessing the efficacy of treatment. These results underline the CD value for a preoperative computation of IJV diameter (e.g. choice of dilation catheters) and confirm that IVUS is the best intraoperative solution for a precise assessment of CSA changes after venous dilation. Differences in IJV evaluation between CD and IVUS could be due to excessive probe pressure on the examined neck, with a subsequent change in vessel shape and dimension. This problem can often be overcome with a new transjugular approach that improves jugular-subclavian junction (J-SJ) exploration with a better view of valvular planes. This new approach often allows correct visualization of valvular planes instead of the laterocervical approach, which at times produces a confusing image. 20 However, the intravenous catheter could alter normal valvular kinesis by distorting the lateral pressure of the vessel. An additional problem regarding IJV angioplasty is its absolute dependence on the analysis of intravenous morphological defects that cause the change in flow.12,21 CD sonography correctly identified vascular malformations (e.g. spur, vein web, annulus, inverted flaps or septum) in most patients with CCSVI.12,21 In our study by providing a mo-nodimensional image of the vessel, CV presented very low accuracy (32%) in identifying endoluminal anomalies and, especially very low sensitivity (6%). For example, it is extremely difficult to differentiate between venous stenosis associated with the presence of annular narrowing from venous stenosis related to an inverted valve or a rigid septum. A proposal was recently made to draft an initial classification of jugular endoluminal anomalies located in the lower part of the jugular vein (J1 level). 21 Five hundred fifty-six venograms analysed in 278 MS patients with CCSVI detected the following four main patterns of anomalies: jugular stenosis without severe structural abnormality (annulus, fused leaflets and transverse leaflets), abnormal valve leaflets (accessory leaflets, ectopic leaflets and long leaflets), septum or membranous obstruction, and a severely malformed valve (inverted valve, sigmoid valve, double valve). 21 However, this study did not compare the results with those of the ultrasound imaging method to confirm the presence of malformations related to the vessel lumen. In contrast, CD sonography was remarkably accurate (88%) in identifying venous anomalies with 93.8% sensitivity and 77.8% specificity. In fact, longitudinal and transversal ultrasound scanning enables the clinician to establish the type of anomaly and to analyse its functional conduct with regard to blood flow. The venous stenosis may be quantitatively defined in terms of reduction of the CSA for the presence of an endoluminal malformation using the IVUS method (intraoperative baseline evaluation and immediate success after PTA). Preoperatively the same result can be obtained with the CD through the use of the ECST (European Carotid Surgery Trial) and NASCET (North American Symptomatic Carotid Endarterectomy Trial) methods in a longitudinal scan.22,23 This allows accurate comparison of these morphological changes and a more accurate representation of the inter-patient variability for the purposes of statistical analysis. Rather, with current technological equipment it seems difficult to quantify the degree of haemodynamic changes produced by such alterations. The presence of anomalies was confirmed by the IVUS study both on tomographic images and on longitudinal reconstructions. Above all, supplementary IVUS information compared malformations and the vessel lumen and yielded useful quantitative data for the instant assessment of changes during angioplasty both in terms of efficacy and potential complications (CSA variations, adjustment or improvement of intravenous malformations, parietal haematoma or fissures). 19 Literature has indicated the superiority of CD sonography in identifying JEM compared with MR 12 and CV. 24 These two methods are important for a precise assessment of collateral veins and anatomical parts of the neck. These data confirm the low capability of MR and CV to correctly identify outflow point anomalies in IJVs. Such conditions underestimate the actual incidence of CCSVI.25,26 Recently Lugli et al. 14 noticed a considerable difference between preoperative ultrasound assessment and venographic findings in patients with CCSVI studied by venography, CD and IVUS.
In conclusion, CD sonography correctly identified JEM that cause a change in cerebral outflow. The maximum diameter and CSA of IJVs are underestimated by CD sonography compared with IVUS (MAXD: mean difference -0.56 mm; CSA: mean difference -11.2 mm2). In our opinion, the role of venography should be solely limited to investigating IJVs and collateral drainage pathways and to the qualitative assessment of venous outflow before and after angioplasty. In fact, CV does not provide reliable quantitative information to plan dilation and take efficacy into account. Hence, we are convinced that IJV angioplasty should be guided and planned by a preliminary CD assessment. Likewise, IVUS should be used during venous dilation to assess its immediate results. This procedure, which is usually employed in selected patients, should be used more frequently because of its remarkable contribution towards accurately detecting endoluminal anomalies in IJVs. Actually, its use reduces the intraoperative risk associated with guidance solely by angiography.
Footnotes
Acknowledgements
We thank Dr Roberto Bergamaschi for his neurological consulting regarding multiple sclerosis and for his revision of the manuscript.