
Abstract
Objectives
The venous clinical severity score (VCSS) and the Aberdeen varicose vein questionnaire (AVVQ) improve after treating chronic venous insufficiency (CVI). The aim was to examine how and why they improve by evaluating the change in each individual question.
Methods
This was an analysis on prospectively collected data from a clinical study on 100 patients (58% female) with CVI (C2 = 34, C3 = 14, C4a = 29, C4b = 9, C5 = 7, C6 = 7) who were randomized to endovenous laser ablation (n = 50) or foam sclerotherapy (n = 50). The change scores (performance) of each question of the VCSS (questions 1–10) and the AVVQ (questions 1–13) were calculated by subtracting the score at three weeks, and three months, from the pre-treatment score.
Results
Both the median, interquartile range (IQR), VCSS and the AVVQ scores improved from 6 (4) and 21.4 (15.1) at baseline to 3 (4) and 18.6 (12.1) at three weeks (P < 0.0005, P = 0.031) to 2 (3) and 8.8 (13.6) at three months, (P < 0.0005, P < 0.0005), respectively. The performance of the first three questions of the VCSS (pain, extent of varicosities, oedema) were the most contributory to the overall score. Questions 5, 7, 8, 9 on ulceration improved the most individually but did not contribute significantly to the overall score. Questions 5, 9 of the AVVQ on stocking use and ulceration failed to contribute statistically to the overall improvement at three months.
Conclusion
The majority of the individual questions of the VCSS and AVVQ responded to change. However, the cause of a poor response was multifactorial with statistical dilution playing a significant role. Stratification of patients according to ulceration may allow better comparisons.
Keywords
Introduction
The venous clinical severity score (VCSS) and the Aberdeen varicose vein questionnaire (AVVQ) are dynamic scoring tools used to quantify the effects of treatment on superficial venous insufficiency (SVI). Their use is recommended in studies which assess the efficacy of endovenous treatments. 1
The VCSS was introduced in 2000 2 (Appendix A) and has been extensively validated and revised as a physician-recorded outcome measure on venous severity.3–8 The AVVQ was introduced in 1993 9 (Appendix B) and has since been validated and revised as a disease-specific patient-reported quality-of-life (QoL) outcome measure.10–12 Both the VCSS and the AVVQ respond overall to treatment as illustrated in a representative recent prospective randomized controlled trial. 13 This is the usual way in which these questionnaires are used. However, it is not clear which individual questions are the most responsive to change and the relationship of this change to clinical severity using the C part of the CEAP (clinical, aetiological, anatomical and pathological elements) classification.14–16 The aim of this study was to evaluate the change in each question following endovenous treatment and to assess the contribution of each question to the total scores. This information may be useful for clinical researchers in improving the dynamic nature of these assessment tools and for questionnaire revision committees.
Methods
Study design
This was a data analysis study to evaluate changes in answers to survey questions over time. The data were collected from a prospective clinical study comparing two different procedures. The study has been published as a randomized controlled trial of 100 patients who were treated with either endo-venous laser ablation with concurrent phlebectomies (EVLA, n = 50) or ultrasound-guided foam sclerotherapy (n = 50). 17 The C part of CEAP was recorded and for the purposes of this analysis remained static throughout the treatment course (disease ‘stage’). This was irrespective of whether the dynamic elements of this classification improved. Patients were assessed at baseline, three weeks and three months using the VCSS and the AVVQ.
Colour duplex was used to confirm eligibility with reflux in the great saphenous vein >0.5 second but without deep venous reflux >1 second The venous filling index (VFI) using air plethysmography (APG-1000® apparatus, ACI Medical LLC, San Marcos, CA, USA) was recorded after an elevation-dependency manoeuvre in order to provide a haemodynamic assessment. 18 Informed consent had been obtained from participating patients.
Patient characteristics and stratification
Of the 100 patients (legs), 58 were female while 60 had bilateral disease, but only the worst leg was enrolled in the study. All patients had exclusive superficial chronic venous insufficiency (CVI). The C class stratification was: C2 = 34, C3 = 14, C4a = 29, C4b = 9, C5 = 7 and C6 = 7. Patients were also stratified according to haemodynamic success at three months (group A, n = 38) defined as the complete absence of saphenous reflux with normalization of the VFI (<2.5 mL/second). The rest were in group B (n = 54). This division was based on an assumption that questionnaire responsiveness may parallel haemodynamic success. Since the AVVQ does not discriminate between unilateral and bilateral disease, patients were stratified accordingly. This was based on an assumption that unilateral veins may demonstrate a greater improvement in comparison with patients with contralateral untreated veins.
Statistical analysis
Data were analyzed using the SPSS statistics version 17 (SPSS Inc., Chicago, IL, USA). The Wilcoxon signed rank test was used to test for significant change within the same question (and same patient) between two time intervals (baseline versus 3 weeks, baseline versus 3 months) and the Friedman test was used to test for significant change between three time intervals (baseline, 3 weeks and 3 months). Change scores (responsiveness) for each question were calculated by subtracting the post-treatment value from the baseline score. Significance was stratified according to three levels: not significant (P > 0.05), significant (P < 0.05–P > 0.0005) and highly significant (P < 0.0005).
Results
Overall responsiveness
The median, interquartile range (IQR), VCSS and the AVVQ scores significantly improved as a result of endovenous treatment. The VCSS decreased from 6 (4) to 3 (4) at three weeks (P < 0.0005) and to 2 (3) at three months (P < 0.0005). The AVVQ also decreased from 21.4 (15.1) to 18.6 (12.1) at three weeks (P = 0.031) and to 8.8 (13.6) at three months (P < 0.0005). The improvement in the VCSS and the AVVQ was also significant throughout the three-week and three-month time intervals, P < 0.0005 and P < 0.0005, respectively (Friedman's test) as depicted in Figure 1. While a global score is useful, a single number representing the VCSS or AVVQ is not an effective indicator as to which categories of patient respond the most to treatment. The results were therefore assessed by categorizing patients according to C class.
The VCSS (a) and AVVQ (b) scores improve significantly three weeks and three months after endovenous intervention
Responsiveness according to C class
When patients were stratified according to increasing severity using the C of CEAP, at baseline, there was a better correlation with the VCSS (Figure 2a) than the AVVQ (Figure 3a), r = 0.584 0.326, respectively, both achieving significance. The VCSS and the AVVQ were also significantly responsive (baseline scores minus post-treatment scores at 3 months) at each stage of severity (P < 0.05, Wilcoxon). When the responsiveness of the VCSS at three months (Figure 2a) was compared against the C stage, significance was achieved (r = 0.251, P = 0.015). The high VCSS change scores from the C6 patients, ranging from a 5- to a 14-point improvement, were responsible for this correlation, which would not have been significant had this category been excluded from the analysis. In contrast, there was no relationship between the degree of improvement of AVVQ and the higher C classes (Figure 3b).
Increases in VCSS correlate significantly with worsening C class (a). The VCSS improves significantly at each stage of severity at 3 months (b), but the degree of improvement (excluding C6) appears static and is irrespective of C class. Dashed line = no change Increases in AVVQ demonstrate a weak but significant correlation with worsening C class (a). The AVVQ improves significantly at each stage of severity at three months (b), but the degree of improvement appears static, without significant correlation, and is irrespective of C class. Dashed line = no change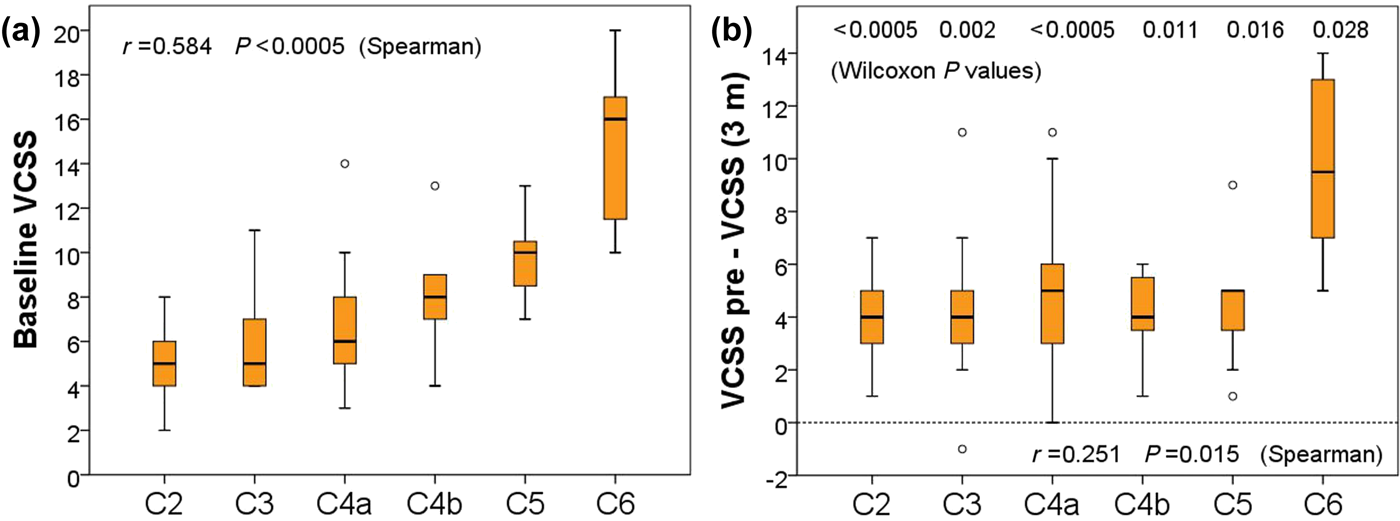
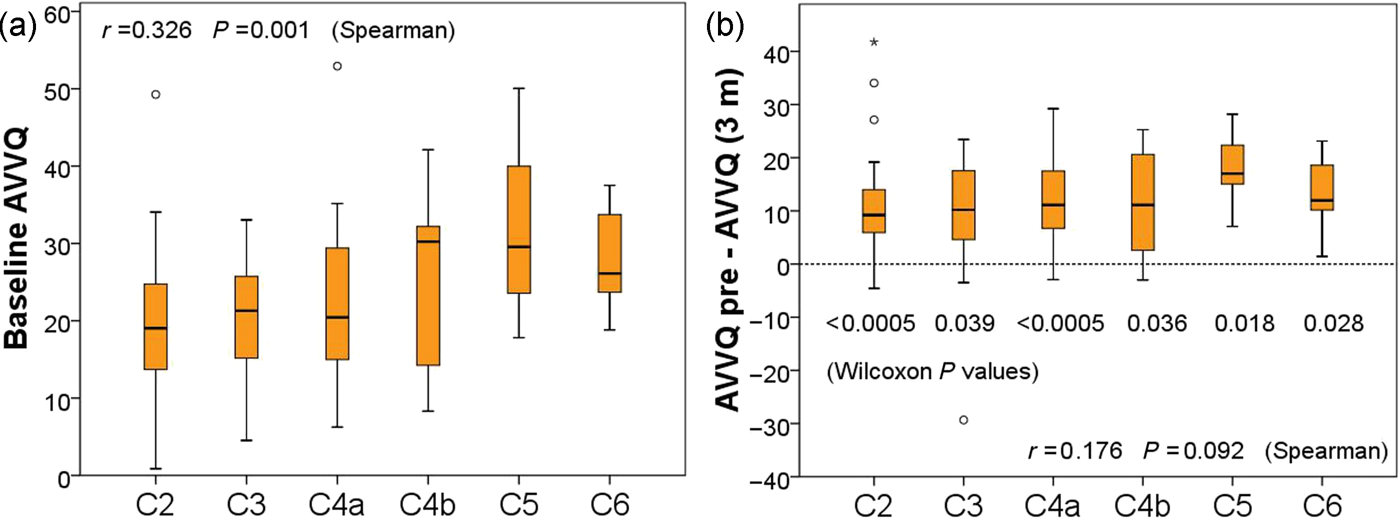
These results indicate that although there was a relationship between increasing severity and the VCSS and AVVQ, there was no relationship between the degree of improvement and increasing severity (excluding C6 VCSS patients). The extent of improvement therefore could be attributed to the proportion of patients in the study cohort with C6 disease rather than a true reflection of improvement. While subdivision according to severity is useful, it does not indicate which questions of the VCSS and the AVVQ are the most responsive to treatment.
Responsiveness of VCSS questions
The first three questions of the VCSS (pain, extent of varicosities and oedema) contributed most to the global score at three months postintervention and the questions specific to ulceration (Q.5, Q.7, Q.8 and Q.9), pigmentation (Q.4) and induration (Q.6) contributed least (Figure 4a). Since only seven of 100 patients had ulcers, failure to achieve a significant impact on the global score was related to the small number because the remaining majority (n = 93) scored a zero for questions on ulceration (Figure 4b). Interestingly, Figure 4a appears to have an inverse relationship to Figure 4b. This is in direct contrast to the VCSS responsiveness when patients were categorized into C6 (Figure 2b), since it was this group that demonstrated the greatest change with an improvement ranging between 5 and 14 points (P = 0.028, Wilcoxon).
A wide variation in the mean change in VCSS scores at three months for the individual questions. The most responsive questions were Q.1, Q.2 and Q.3 (a). Small changes may be related to statistical dilution from a high proportion of patients scoring zero for Q.5–Q.9 at baseline (b)
Responsiveness of AVVQ questions
At three months, the majority of the answers to the AVVQ questions improved statistically as a result of intervention (P < 0.0005). Question 3 on the use of analgesia was also significant (P < 0.05). However, Q.5 (stocking use) and Q.9 (ulceration) did not have a significant impact upon the global score. When patients were stratified according to the C class the responsiveness of the AVVQ in C6 patients was significant (P = 0.028, Wilcoxon). The greatest mean change was demonstrated in Q.1 through a reduction in the distribution and extent of varicose veins (P < 0.0005) and in Q.10 by an improved cosmetic appearance (P < 0.0005) as depicted in Figure 5a. It is likely that the lack of impact upon the global score in the ulceration group (n = 7) is due to the small number because most patients scored a zero for Q.9 (ulceration) at baseline as shown in Figure 5b.
The mean change in AVVQ scores at three months for each question demonstrates a wide variation, with Q.1 and Q.10 responding the most (a). The proportion of patients scoring zero at baseline are also illustrated (b)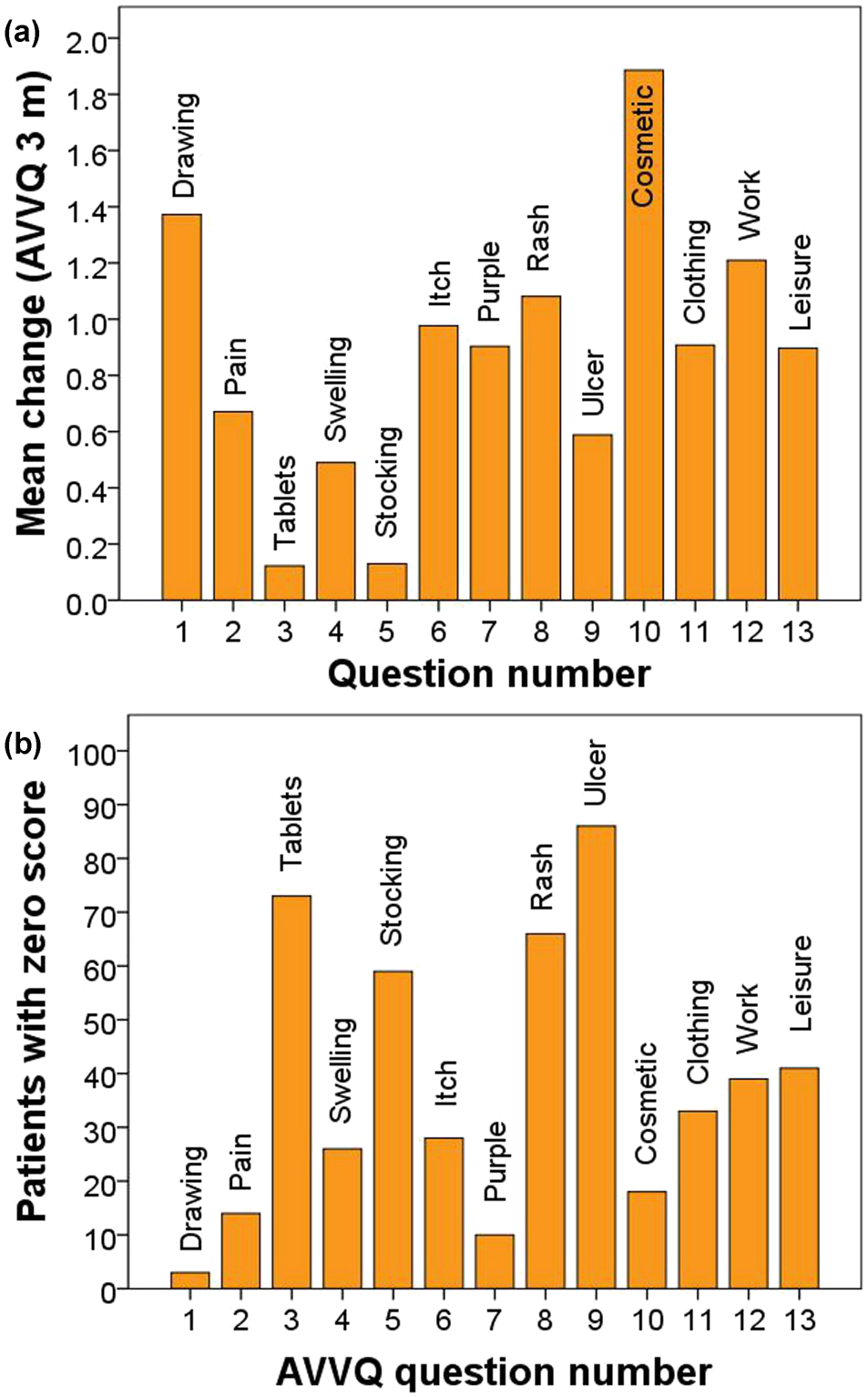
Subgroup analysis
A subgroup analysis was performed according to intervention at three weeks and three months and also according to haemodynamic success at three months (Group A = 38, Group B = 54) to determine if any of these factors changed the responsiveness of the individual questions.
There was no significant difference in the change scores (3 months) of the VCSS or the AVVQ when patients were stratified by treatment type P = 0.82 and 0.06, respectively (Mann-Whitney U test). Stratification by haemodynamic success was also not significant at P = 0.107 and 0.677, respectively (Mann-Whitney U test). Similarly, there was no difference in the change scores of the AVVQ at three months, when patients were stratified according to uni/bilateral disease, P = 0.495 (Mann-Whitney U test).
Level of significance* in the change scores of the individual VCSS† questions according to different subgroups; stratified by time, endovenous treatment and haemodynamic success (Group A and B)

Group A, haemodynamic success at three months with the absence of reflux on duplex and a venous filling index <2.5 mL/second. Group B, haemodynamic failure
*Wilcoxon signed rank test
† Venous clinical severity score
‡ Deterioration
Level of significance* in the change scores of the individual AVVQ† questions according to different subgroups; stratified by time, endovenous treatment, uni/bilateral and haemodynamic success (Group A and B)

Group A, haemodynamic success at three months with the absence of reflux on duplex and a venous filling index <2.5 mL/second. Group B, haemodynamic failure
*Wilcoxon signed rank test
†Aberdeen varicose vein questionnaire
‡Deterioration
Discussion
This study supports the use of the VCSS and AVVQ after endovenous treatment. In this study, the VCSS had a better correlation with clinical severity than the AVVQ, r = 0.584 and 0.326, respectively. The VCSS and the AVVQ significantly reduced after endovenous treatment and at each level of clinical severity. However, the degree of improvement was not related to C class, except for the improvement in the VCSS in C6 patients. Some questions failed to statistically contribute overall to the scores because of statistical dilution with many VCSS questions recording zero scores. Improvement in the VCSS, for example, may be positively influenced by the proportion of patients with active ulceration. This observation is not surprising since 12 out of the 30 possible scores are specific to the severity of ulceration.
Questions 1, 2 and 3 of the VCSS and questions 1 and 10 of the AVVQ demonstrated the greatest mean change (responsiveness) at three months after treatment. Very few patients scored a zero for these questions at baseline, which indicated that the changes are likely to be representative of the study group. Stratifying patients by treatment type, postprocedural assessment time or haemodynamic effectiveness did not significantly alter these results.
The AVVQ was designed as a postal questionnaire 9 with some questions left unanswered: Q.1 for example, where patients are requested to draw their veins, rather than tick a box. Lack of patient response may also include questions which are usually given zero scores (Q.9 on ulceration) as well as questions which attract points (Q.1 vein drawings on legs). The significance of an unanswered question will therefore differ according to clinical severity. If an ulcer patient leaves out Q.9 it would be of greater significance than a C2 patient who would inevitably score zero for this question. Patients should therefore be encouraged to fill in every question. It was part of the methodology of this study for patients to complete the AVVQ in a hospital environment. Furthermore, knowledge of the likelihood of an unanswered question being zero may result in a revision of the scoring adjustment policy which states: ‘If a question is omitted by a patient the total score is calculated after removing the score for that question from the denominator’. 9 The alternative of filling in omitted questions on behalf of the patient is not advised as it would be contrary to the principle of the AVVQ as a patient-reported outcome measure. 19 Stratifying patients by C class and ensuring each question is answered may therefore improve the performance of the AVVQ.
The observation that the scores of Q.10 of the VCSS and Q.5 of the AVVQ significantly deteriorated at three weeks interrogates the relationship between the use of compression and the severity of the disease. It is known that stockings are uncomfortable and that there is a trade-off between the symptom relief gained with stockings against their discomfort, difficulty in application, erratic prescribing and high cost.20,21 There is also the patients’ expectation that they may be free of compression following treatment which may artificially reduce the severity. However, the most likely explanation for deterioration was that patients were told to wear compression following intervention. Three weeks may be too early to assess severity when the benefits of treatment are off-set with recovery. A limited review performed by Darvall et al. 11 noted that the AVVQ appeared to worsen in the early weeks after surgery and EVLA, before improving by 4–6 weeks. The questions which relate to stocking use (VCSS Q.10, AVVQ Q.5) have been shown in our study to hamper responsiveness if the AVVQ is used at 3 weeks.
Contrary to expectation, stratification of patients into haemodynamic success and failure (groups A and B, respectively) did not affect the responsiveness of the questions in the VCSS or the AVVQ. Haemodynamic parameters usually show poor correlation with clinical severity, so this result would be in keeping with similar studies which examine venous haemodynamics.22–24 Explanations for this include the lead times for the haemodynamic insult and its correction to become clinically noticeable.
When patients were stratified into uni/bilateral disease the majority of the AVVQ questions, except Q.3, Q.5 and Q.9 (analgesia use, stocking use and ulceration) were responsive. It came as a surprise that the change in nearly all the questions in patients with bilateral disease were in the higher level of significance (P < 0.0005) with the responsiveness in the patients with unilateral disease at a lower level (P > 0.0005). This may be because patients with bilateral disease record severity in the contra-lateral leg before intervention but focusing their response on the treated leg after intervention. Whatever the reason, these results indicate that the responsiveness of the AVVQ may have more meaning if assessed in relationship to uni/bilateral disease.
The results on this study were assessed at three weeks and three months. Three weeks may be considered too soon to expect improvement in some of the less responsive questions. Analgesia use, gaitor induration, postinflammatory hyperpigmentation and stocking use may be an effect of treatment, rather than an index of severity. Furthermore, it may take much longer than three months for the baseline pigmentation and induration to reduce to a degree that will be detected on questionnaires.
In 2000, Rutherford et al. 2 proposed the VCSS as an adjunct to venous outcome assessment. This study has examined the performance of the VCSS when used as adjunct to the C part of the CEAP classification, rather than a global score, irrespective of the clinical stage of disease. Since the VCSS is an ordinal scale based on the attributes of severity, rather than severity itself, it may be more meaningful if the VCSS was recorded for each stage of C. This research therefore reflects the original intention of the American Venous Forum Ad Hoc Committee on Venous Outcomes Assessment to use the VCSS on patients with similar degrees of clinical severity. 2
Significant correlations between baseline VCSS and the C of CEAP have been described previously by our group 5 and others, 3 and are in keeping with the correlations in this study. The correlation between the VCSS and the C of CEAP was better than between the AVVQ and CEAP, which is not surprising since the VCSS was developed in relation to CEAP.
The C part of CEAP is the only widespread acknowledged classification that is able to stratify patients according to categories of severity based on the progression of CVI. Therefore, the proposal of improving the responsiveness of the VCSS and AVVQ according to CEAP seems valid. However, this could only be achieved provided the C of CEAP is used as a static scoring system for the purposes of studies, and provided each C stage can be precisely defined and interpreted with good inter-observer reproducibility.25,26 Since this study has demonstrated a lack of a relationship between increasing responsiveness with increasing C class (excluding C6) it may be valid to categorize patients into two groups based on the presence or absence of ulceration: C2–5 and C6. This may allow the VCSS to reflect a better improvement by eliminating the type and percentage of venous disease in the cohort as a confounding variable.
Conclusion
The majority of the VCSS and the AVVQ questions are responsive to endovenous treatment. However, the causes of a poor response are multifactorial: statistical dilution, the timing of a question (stocking use and not fully recovered from treatment at 3 weeks), question omission (patients are often reluctant to draw in their veins), uni/bilateral disease (with the AVVQ) and genuine unresponsiveness (it may take more than 3 months for pigmentation or induration to improve) are factors requiring closer examination by revision committees. Stratification by C class, especially C6, may rectify some of these causes and could result in further improvements.
Footnotes
Acknowledgements
We acknowledge the help of Dr Michael A Vasquez (Venous Institute, Buffalo, NY 14120, USA) for his moderation and critical revision in parts of this manuscript.
Appendix A
Venous clinical severity score summarized as an aide memoire. Readers are advised to consult the full paper for a detailed explanation of the scoring.
2
Attribute
Absent = 0
Mild = 1
Moderate = 2
Severe = 3
Pain
None
Occasional
Analgesia
Limiting
Varicose veins
None
Few
Calf or thigh
Thigh and calf
Venous edema
None
Evening ankle
Afternoon leg
Morning leg
Pigmentation
None/tan only
Limited
<1/3 leg
>1/3 leg
Inflammation
None
Ulcer margin
<1/3 leg
>1/3 leg
Induration
None
<5 cm
<1/3 leg
>1/3 leg
Ulcers (n)
None
1
2
>2
Ulcer duration
None
<3 months
>3 months
>1 year
Ulcer size
None
<2 cm diameter
2–6 cm diameter
>6 cm diameter
Compression
None
Intermittent
Most days
Full compliance
Appendix B
The individual questions of the Aberdeen varicose vein questionnaire from which patients are requested to tick one box for each leg. Readers are advised to consult the full paper for a detailed explanation of the scoring system.
9
Q.1
Please draw in your varicose veins in the diagram(s) below:
Q.2
In the last 2 weeks, for how many days did your varicose veins cause you pain or ache?
Q.3
During the last 2 weeks, on how many days did you take painkilling tablets for your varicose veins?
Q.4
In the last 2 weeks, how much ankle swelling have you had?
Q.5
In the last 2 weeks, have you worn support stockings or tights?
Q.6
In the last 2 weeks, have you had any itching in association with your varicose veins?
Q.7
Do you have purple discolouration caused by tiny blood vessels in the skin, in association with your varicose veins?
Q.8
Do you have a rash or eczema in the area of your ankle?
Q.9
Do you have a skin ulcer associated with your varicose veins?
Q.10
Does the appearance of your varicose veins cause you concern?
Q.11
Does the appearance of your varicose veins influence your choice of clothing including tights?
Q.12
During the last 2 weeks, have your varicose veins interfered with your work/housework or other daily activities?
Q.13
During the last 2 weeks, have your varicose veins interfered with your leisure activities (including sport, hobbies and social life)?