
Abstract
Objectives
To determine the rate of superficial venous thrombosis in patients undergoing great saphenous vein (GSV) harvesting for coronary artery bypass surgery (CABG).
Methods
Post-CABG patients with suspected lower-extremity thrombosis underwent duplex scanning. Thrombus in the saphenofemoral junction stump was noted, and thrombus extension and associated complications collected.
Results
Out of 2335 patients who underwent CABG in five years, 98 patients presented with signs and symptoms of lower-extremity thrombosis. Thrombosis was present in 19 (19.4%) of these patients, 15 of which had a thrombus in the GSV. Five patients had significant signs and symptoms of pulmonary embolism (PE). On objective diagnostic imaging, three of them had a PE.
Conclusion
Patients undergoing great saphenous vein harvesting for CABG are at an increased risk of developing superficial vein thrombosis especially at the saphenous stump. Given the increased risk of deep vein thrombosis and PE, further studies investigating this topic are warranted.
Introduction
There has been a growing interest in superficial thrombophlebitis of the lower extremities in the past few years. This is largely due to a growing body of evidence suggesting a correlation between superficial venous thrombosis (SVT) and deep venous thrombosis (DVT).1–3 Furthermore, it has been reported that up to 44% of patients with SVT (especially if located in the saphenous main trunk) end up developing a DVT, up to 33% end up with an asymptomatic pulmonary embolism (PE) and shockingly, up to 13% develop a symptomatic PE.1–3 Given the clinical importance of SVT located in the main saphenous trunk, patients undergoing saphenous vein harvest for coronary artery bypass graft (CABG) represent a unique population of patients to study. These patients were left with a stump of the great saphenous vein (GSV) at risk of containing a thrombus. Complications of these thrombi and patient outcomes are studied in this paper, with an emphasis on screening and treatment.
Methods
A retrospective review of prospectively collected data spanning five consecutive years of all patients undergoing CABG alone was performed. All patients who underwent harvesting of their GSV as part of their CABG procedure and now presenting with signs and symptoms of venous thromboembolism (VTE) in the ipsilateral leg were included in the study. Patients with thrombosis in the contralateral limb or in any veins other than the GSV stump and common femoral vein were reviewed, but excluded from the main analysis. All lower-extremity veins from the groin to ankle were examined by colour flow duplex scanning as previously described. 4 The criteria used to detect thrombosis were non-compressibility of the vein by B-mode scanning and/or a filling defect during color flow imaging. If asymmetry was seen in the signal between the two common femoral veins, the pelvic veins were scanned. Color flow duplex scanning was performed 2 to 16 days after CABG. The stump of the GSV and its tributaries in the saphenofemoral junction (SFJ) were examined in detail. The thrombus length and its association with the common femoral vein were recorded. VTE rate in the CABG patients was compared with patients with chronic venous disease that underwent endovenous thermal ablation (EVA) or ligation and stripping of the great saphenous vein. Patients from these comparative groups were randomly selected from our prospective database. Those patients that underwent stripping and ligation were done earlier when the endovascular techniques were not as popular.
Statistical analysis
Descriptive statistics were used to report the data as mean +/– SD and as percentages for categorical variables. Continuous variables (i.e. age) were compared using the independent sample Student's f-test. Categorical variables were compared using the Fisher's exact test even when the expect value in any of the cell was more than 5. A two-tailed comparison was performed in all the analysis, and an alpha of 0.05 was used for significance. The data were analysed using SPSS 19 (Chicago, IL, USA).
Results
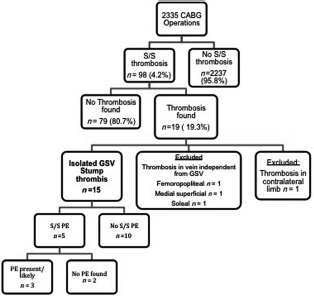
In the last five years, 2335 CABG procedures with GSV harvesting were performed. Ninety-eight (4.2%) of these patients were referred to the vascular laboratory with signs and symptoms of VTE mostly during hospital stay or shortly after discharge. Thrombosis was present in nineteen patients (19.3%). One of the patients had a protein C deficiency. Four patients were excluded from the analysis because thrombosis was found in either the contralateral limb (n = 1, popliteal vein), or in the ipsilateral limb in veins independent of the GSV stump (n = 3, one femoropopliteal, one medial superficial vein tributary below the knee and one soleal vein). The remaining fifteen patients (15%) had thrombus only in the GSV stump. There were nine females and six males with a mean age of 68 ± 5 years. There were four additional patients with superficial vein thrombosis away from the SFJ stump. In two, the thrombus was found in the remaining GSV in the distal calf and in the other two in GSV tributaries. None of the four patients developed any complications related to this thrombosis, and their symptoms resolved within a month. The length of the GSV stump ranged from 1.5 to 5 cm. The length of the thrombus ranged from 1 to 4 cm. The length of the stump and the thrombus were not associated with the clinical presentation, thrombus propagation or the development of PE. However, the sample size was too small to perform valid statistical comparisons.
Complications
At the initial presentation, three patients had a thrombus either adhered to the anterior wall (n = 1), or free floating into the common femoral vein (n = 2). Five of the 15 patients developed PE symptoms and underwent ventilation-perfusion scanning (n = 3) or spiral computed tomography (CT) (n = 2). Two of the five patients had a high probability ventilation-perfusion scanning; one had a thrombus on spiral CT; and two were normal (Figure 1). Thirteen of the 15 patients were anticoagulated with heparin and Coumadin. Nine patients were re-examined either to follow up on a thrombus extension (n = 5) or because of worsening symptoms (n = 4). Despite anticoagulation, extension of thrombosis in the common femoral vein was found in two patients. (Figure 2).
A 67-year-old male patient who presented with signs and symptoms of VTE after GSV harvesting for CABG. (a) Duplex scanning of a GSV stump thrombosis showing non-compressibility of the vein, (b) Colour imaging demonstrates absence of flow in the GSV stump. GSV is dilated with echolucent, homogenous content indicating acute vein thrombosis, (c) Computed tomographic angiography demonstrating bilateral segmental PE (arrows). VTE, venous thromboembolism; GSV, great saphenous vein; CABG, coronary artery bypass surgery; PE, pulmonary embolism Patient presentation and progression diagram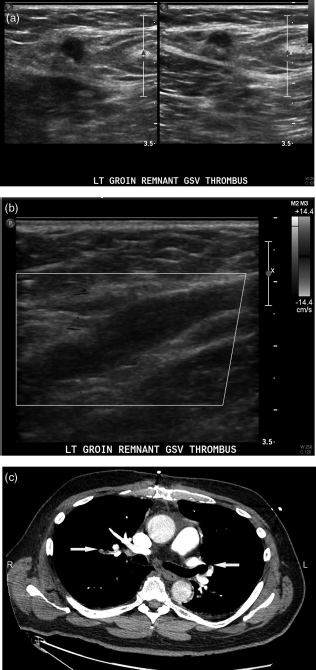
Comparative rates
The rates of DVTs in GSV harvesting compared with EVA and ligation and stripping for a different group of patients were 1.9%, 1.3% and 2.7%, respectively (Table 1). GSV harvesting patients were significantly older than the EVA and Ligation and Stripping groups. PE rates were also comparable with only one PE seen in the EVA group, none seen in the ligation and stripping group and three in the GSV harvesting group. The number of patients having thrombus in the SFJ was much higher in the GSV harvesting group (15.3%) compared with 9.3% in the EVA group and only 2.7% in the ligation and stripping group (P < 0.01 for both comparisons, Table 1).
Venous thromboembolism rates
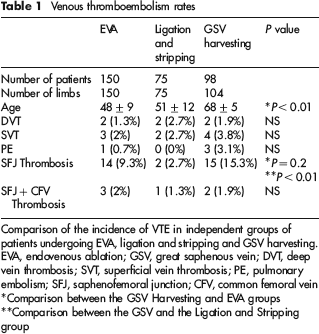
Comparison of the incidence of VTE in independent groups of patients undergoing EVA, ligation and stripping and GSV harvesting. EVA, endovenous ablation; GSV, great saphenous vein; DVT, deep vein thrombosis; SVT, superficial vein thrombosis; PE, pulmonary embolism; SFJ, saphenofemoral junction; CFV, common femoral vein
Comparison between the GSV Harvesting and EVA groups
Comparison between the GSV and the Ligation and Stripping group
Disscusion
Post cardiac surgery patients where the GSV has been harvested represent a unique challenge for DVT evaluation given common presentation of pain and swelling in the ipsilateral leg. Nonetheless, patients determined to have significant enough signs and symptoms underwent duplex scanning to rule out DVT. Although the duplex scanning was negative for DVT in every patient, 15 patients had venous thrombosis in the stump of the GSV ligated for CABG. All of the patients were treated with the conventional anticoagulation therapy of heparin and Coumadin. Five of the patients (33%) had thrombus into the CFV, three of which during the initial presentation, and the other two during follow-up. Three of the 15 patients (20%) developed non-fatal PE. Although the incidence of PE in post-CABG patients is supposedly uncommon due to strict anticoagulation regimens, rates from 0.5% to 3.9% have been documented.5–7 These percentages translate into a high proportion of postsurgery mortality rates from 19% to 34% of patients who suffered PEs.6,7 It is important to note that while 98 patients were evaluated in this series, the number of patients with asymptomatic thrombus is unknown. The identification and management of asymptomatic DVTs is not discussed in this manuscript but does represent an area with much debate and little data.
There is a significant correlation between SVT and DVT.1,2,8–14 Jorgensen et al. 10 emphasized the importance of systematically screening patients with SVT for underlying DVT involvement due to an increased risk of both DVT and associated complications in this patient group. The authors also noted that the SVT location is not prognostic of the underlying DVT site; source of the thrombus was predominantly found in either the calf or popliteal veins. Contradictory studies have shown that 70–90% of thrombi that extend into the deep veins originate in the GSV1,2 Thrombi in the superficial and deep veins can coexist without being continuous. Likewise, thrombus progression can occur from superficial to deep veins or from deep to superficial veins. SFJ is the most common route from which a thrombus extends from superficial to deep veins.1,2 In the current study, the thrombus in the stump of GSV could only progress to the common femoral vein.
Extension of SVT into the common femoral vein occurs more frequently than once thought,1–3,9,10,15–18 and is linked to an increased risk of PE ranging from 0 to 33.3%.2,9,11,13,18–20 According to Lohr et al. 16 , neither symptoms, risk factors, nor physical examination are predictive of common femoral vein thrombus extension. A majority of patients lack any signs or symptoms of DVT. 16 Murgia et al. 14 found that the thrombus is always more proximal than the clinical appearance would suggest. Hence, thorough screening of patients presenting with SVT is essential.
It has been shown that a thrombus in the below-knee segment of the GSV is benign unless it extends into the above-knee segment. In a recent prospective study, 33% of patients with thrombus in the above-knee segment of GSV had a PE. However, the proximity of the thrombus to the SFJ was not associated with PE. The authors concluded that their findings warrant a larger prospective study. In our study, all patients presented with a thrombus in the SFJ – a condition that should be considered at least as dangerous as a thrombus in the above-knee segment of GSV. Although one could argue that the length of thrombus is longer when the GSV is intact, many studies in patients with proximal DVT find no association between the length of the thrombus and the incidence of PE. In this study, we tried to look at data from two different interventions to the GSV and compare the findings relating to VTE. Despite having a much older and relatively sicker patient population undergoing CABG, the rates of SVT, DVT, PE and even propagation from the SFJ to the CFV where comparable between EVA, ligation and stripping and GSV harvesting.
Currently, there are two primary modes of treatment: anticoagulation and surgical intervention. Ascer et al. followed an anticoagulation regimen that resolved 12 of 13 SFJ thromboses. They assert that this treatment competes with surgical ligation for effective treatment of thrombosis and prevention of PE. 11 However, surgical intervention seems to be favoured by most others. In a recent large prospective controlled study, it was demonstrated that although anticoagulation and surgery were good methods for treating SVT, surgery decreased the incidence of thrombus extension to the deep veins. 21 Lofgren and Lofgren 19 advocate surgical excision of the thrombosed veins with stripping of the associated varices. Pulliam et al. 15 chose surgical therapy in progressive SVT to prevent DVT. According to Lohr et al., surgical intervention is the treatment of choice when the thrombus is within 3 cm of the SFJ. Thirty-seven of the 43 patients (86%) were treated either as outpatients or were discharged home within three days of the operation, supporting the efficiency of surgery. 16 Murgia et al. 14 prefer saphenofemoral disconnection to decrease DVT progression and PE risk.
It should be mentioned that although protein C deficiency was revealed in one patient, hypercoaguable conditions were not a focal point in this study. However, Hanson et al. 21 discovered that 35% of patients with an isolated SVT have a hypercoaguable state. A review paper on SVT states that all patients with propagating superficial thrombosis should be treated. 22 It is also recommended that young patients with new or recurrent thrombosis should be examined for a hypercoaguable state.
While interesting, the topic of DVT prophylaxis after CABG surgery was not studied. The current guidelines regarding DVT prophylaxis for patients undergoing CABG remains controversial, with practices differing for different surgeons. It has been previously thought that since CABG patient receive a high heparin dosage as part of their anticoagulation during their operation they are protected from DVT occurrences afterwards, hypothetically eliminating the need for DVT prophylaxis. However, relatively recent evidence suggest that up to 13% of patients undergoing cardiac surgery develop silent DVTs despite an aggressive prophylaxis strategy. 23 This study provides a possible mechanism of how DVTs can occur in CABG patients undergoing GSV harvesting.
This is an observational retrospective study and has a number of limitations. The relatively small sample size of patients presenting with symptomatic VTE makes it difficult to control for confounders. Furthermore, unless done in a prospective manner, studying asymptomatic VTE in these patients is not possible, and therefore was not performed here. We do not have data on DVT prophylaxis practices by the different surgeons, and while most surgeons do not perform DVT prophylaxis after CABG, that data are not available. The retrospective nature of this study makes it also difficult to have a unified protocol for the clinical management for patients presenting with VTE including diagnostic testing for a suspected PE. The main strength of this study, however, is it is the first of its kind to explore the issue of GSV stump thrombosis in CABG patients providing preliminary evidence to attempt to explain the higher than expected rate of DVTs seen in cardiac surgery patients.
In conclusion, thrombosis in the GSV stump after CABG is found in 15% of patients who present with signs and symptoms of VTE. Duplex scanning is essential for objective diagnosis of GSV stump thrombosis and monitoring extension of the thrombus. Rapid and thorough treatment should be implemented in these patients due to potential for thrombus extension and PE. Furthermore, complete removal of the SFJ may help prevent thrombotic events from occurring.