
Abstract
Objectives: To determine the prevalence, distribution and extent of phlebosclerosis in an outpatient population referred to vascular clinic.
Design: Prospective cohort study.
Patients and Methods: Seven hundred and forty consecutive patients, 302 (41%) men with a cohort median age of 49 (range, 18–84), were referred to the vascular clinic for detection of lower extremity acute or chronic venous disease. A total of 1000 limbs were assessed using duplex ultrasonography. Deep veins were not assessed. Characteristics of venous wall and lumen were studied. Phlebosclerosis was diagnosed based on the increased echogenicity and thickness or calcification of the venous wall. Patients with known trauma or any surgery in the lower extremities were excluded. Two control groups were used for comparison, one of consecutive patients undergoing vein mapping (n = 100) and the other of younger volunteers free of any vein disease (n = 25).
Results: Of the 1000 limbs (right: 458, left: 542) studied by duplex ultrasound, 21 limbs had intense brightness of the venous wall. Fifteen of them had also calcifications and 61 wall thickening. The prevalence of phlebosclerosis was significantly higher in the patient group when compared with control groups 1 (P = 0.019) and 2 (P = 0.011). The mean age of patients with phlebosclerosis was higher compared with the whole patient group (57 versus 49 years, P < 0.0001). Phlebosclerosis affected all superficial veins with greater prevalence in the small saphenous vein (SSV). The mean length of the phlebosclerotic lesion was 2 cm (range 1–7 cm).
Conclusion: The prevalence of phlebosclerosis in the lower extremities appears to be low with no significant sex differences. Age and chronic venous disease are important factors for its development. It may be present in the absence of thrombosis or reflux. A greater prevalence of phlebosclerotic lesions was found in the SSV.
Keywords
Phlebosclerosis constitutes a fibrous degeneration of the venous wall, predominantly the intima, with or without calcification. It was first described by Morgagni in the mid–18th century based on observations about calcified plaques found in the inferior vena cava. With the advent of microscopy, confirmation of sclerotic changes in the venous wall hinges on histological findings of abnormal deposition of collagen in areas of endophlebohypertrophy. 1
Phlebosclerosis has been described to affect almost the entire venous system including the upper and lower extremities.2,3 Nevertheless, most of the recent data stems from the field of gastroenterology with the recognition of mesenteric phlebosclerosis as a non-thrombotic venous process causing bowel ischaemia.4–6 Notably, patients who undergo arteriovenous fistula creation and lower extremity or coronary bypass surgery are also at risk of having their venous conduit affected by phlebosclerosis. 7 In regards to upper and lower extremities, it is more common in the lower extremities being described affecting both the deep and superficial venous system.
Non-varicose and varicose veins may be sclerotic with changes secondary to inflammatory reactions with leukocyte infiltration in the vein wall. 2 Frequently phlebosclerosis is found in the elderly; however, it is not restricted to older populations and there is no correlation between age and its severity. Controversy about definition, aetiology, pathogenesis and histological aspects of phlebosclerosis exists. The present study aims to determine the prevalence, distribution and extent of phlebosclerosis in the lower extremity veins.
Patients and methods
There were 740 consecutive patients who were referred to the vascular clinic for detection of lower extremity acute or chronic venous disease. Patients with known trauma or any operations previous bypass grafts, vein harvesting, dialysis access and catheter insertion in the lower extremities were excluded. Inpatients were also excluded given the potential inability to perform a full venous exam in standing position.
All patients were examined with duplex ultrasound (DU) by experienced vascular technologists (>2000 venous studies for each technologist prior to the study) who were familiar in examining the vessel wall changes through the routine vein mapping or when measuring the carotid intimamedia thickness. High resolution multifrequency linear array transducers were utilized to evaluate the veins. Other higher frequency transducers were used to accomplish better resolution when more superficial veins were investigated. Phlebosclerosis was diagnosed by the increased echogenicity of the venous wall which was measured using the external and intraluminal wall boundaries. Only patients with distinct and intense wall brightness were diagnosed to have phlebosclerosis. Wall calcification was determined by the acoustic shadow posterior to the wall. Patients with luminal occlusion and endoluminal synechiae and vein segments with varicosities or aneurysms were studied but excluded from the analysis as only patients with wall changes were included.
B-mode imaging was optimized by fine tuning the overall gain, placing the focus at the venous wall and selecting the best fit of time-gain compensation at that level. In every image the lumen was set to appear dark without any intraluminal speckles. The transducer was always positioned to have a right angle on the venous wall to maximize resolution. During imaging the vein wall was selected with high definition zoom prior to freezing the image to allow the best possible definition of the wall structure. Examples of veins with phlebosclerosis are shown in (Figure 1).
Ultrasound images of phlebosclerosis in the lower extremities. A. Calcification is seen in the posterior wall of the small saphenous (cross-sectional view) in the upper calf of a female patient. Part of the anterior wall is echogenic without shadowing indicating the presence of fibrous tissue without heavy calcification. B. Calcification of the great saphenous vein (long view) in the calf of a male patient. Wall thickening is seen both proximal and distal to calcification in the posterior wall. The presence of heavy calcification in both patients is evident by the marked acoustic shadowing deeper and in continuity with the posterior wall.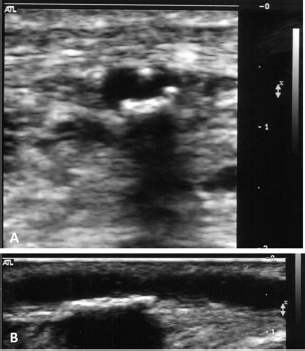
Two control groups were utilized for comparison. The control group 1 consisted of patients referred for venous mapping prior to bypass surgery with no signs or symptoms of venous disease in the lower extremities. This control group included 100 patients (200 limbs) with a median age of 64 (range, 41–79). From group 1, 34 additional patients were excluded due to luminal occlusion, intraluminal synechiae, trauma or previous surgery. The control group 2 was formed by 25 younger, healthy volunteers without any signs and symptoms of chronic venous disease. They were 14 men and 11 women with mean age of 24 (range, 19–28). Four additional volunteers were excluded as three had reticular or varicose veins and one had previous lower limb trauma.
Statistical analysis
Descriptive statistics were used to analyse the patients and control groups. Continuous variables were reported as mean value and range, and categorical variables as percentages. The prevalence of phlebosclerosis in the groups was compared using a two-tailed χ 2 test while the age was compared with a two-tailed t-test. All statistical analyses were performed by SPSS v14 (IBM Corp, Minneapolis, MN, USA).
Results
Cohort description and prevalence
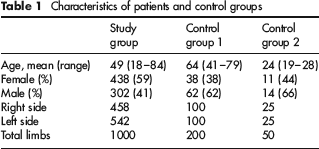
Seven hundred and forty consecutive patients were included in this study group being 302 men and 438 women with a median age of 49 years (range 18–84). A total of 458 right limbs and 542 left limbs were evaluated using DU (Table 1). In the study group, sclerotic changes were demonstrated in 21 limbs confirmed by increased brightness in the vein wall. Of those 21 limbs, eight belonged to men and 13 to women. Another 15 limbs (6 men) had wall calcification and 61 had increased wall thickness (24 men). The prevalence of phlebosclerosis for intense wall brightness and calcification was 3.6% and when the increase wall thickness is included it was 9.7%.
Characteristics of patients and control groups
Control group specifics and location of phlebosclerosis
There were nine limbs with wall changes in the control group 1 (4.5%). None of the limbs studied in the control group 2 had any wall changes. The prevalence of phlebosclerosis was significantly higher in the patient group when compared with control groups 1 (P = 0.019) and 2 (P = 0.011). Evidence of reflux in the area of the intense brightness or calcification was demonstrated in eight limbs and possible thrombosis in six (4 of these limbs had reflux as well) in the patients group and in three of the control group 1 (Table 2). In the patients group of the 61 limbs with increased wall thickening 38 had reflux in the affected area while 14 had reflux in adjacent vein segments and nine had no venous reflux.
Type of wall change and vein location
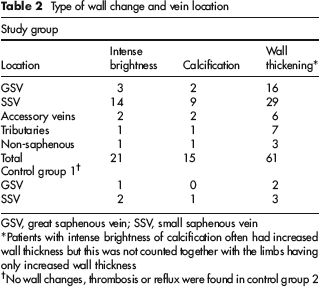
GSV, great saphenous vein; SSV, small saphenous vein
Patients with intense brightness of calcification often had increased wall thickness but this was not counted together with the limbs having only increased wall thickness
No wall changes, thrombosis or reflux were found in control group 2
The most common location of phlebosclerotic changes was the small saphenous vein (SSV). The great saphenous and accessory veins, other tributaries and non-saphenous veins were also affected. The distribution of the phlebosclerotic lesions based upon the anatomical location is listed in Table 2. The presence of reflux or thrombosis in the corresponding vein segments was also noted. The mean length of the phlebosclerotic lesions was 2 cm varying from 1 to 7 cm. The control group 1 was significantly older (P < 0.0001) and the control group 2 was significantly younger than the patients (P < 0.0001). The mean age of patients affected by phlebosclerosis was 57 years, which is higher than the mean age of the whole group (P < 0.0001). In the control group 1 the mean age was 67 years which was comparable to the mean age of this group overall (P = 0.2).
Discussion
Phlebosclerosis is a rare entity affecting the venous wall that has gained little attention since its discovery more than 300 years ago. 8 The exact cause of sclerotic changes in the vein wall is unknown; however, prolonged venous hypertension found in patients bearing other flow disturbances such as congestive heart failure has been found to be involved in its pathogenesis.9,10 Fibrotic changes in the venous wall have also been demonstrated in patients with varicose veins. The venous wall compliance is reduced in veins with sclerotic changes. In addition, it has been speculated that stiff veins have reduced capacitance aggravating venous insufficiency.
Recently, ultrasound has been utilized to evaluate the quality of superficial veins that are intent to be used as vein conduits prior to coronary and vascular surgery bypass procedures or in haemodialysis access creation. 11 The actual importance of knowing whether phlebosclerosis is present in a bypass conduit or outflow in an arteriovenous fistula is its potential implication on patency rates.11,12 A study of 513 infrainguinal vein bypasses showed that 30-month patency was 32% in patients who received a vein conduit with thickened and sclerotic wall changes compared with 73% patency rate in veins with no detectable wall changes by duplex ultrasound. 13 In another study analysing 91 vein remnants of infrainguinal bypasses vein conduits with thicker walls had significant lesions compared with normally functioning grafts. 14 The thickening of intima was the most important factor involved in vein conduit lesions. 14 All veins utilized in this study were preoperatively classified as satisfactory by ultrasound. 14 Nonetheless, those studies were published in the early 1990s.13,14 At that time, vein mapping was more limited to identify phlebosclerosis. Currently, a higher-definition of ultrasound imaging technology is available allowing better detailed visualization of the vein wall.
Varicosities in the main trunk of the saphenous veins are rare. 15 When they are present are of short distance. The varicosities in the extremities are found in the tributaries. Therefore, the saphenous vein could be used for bypass in a significant number of patients who present with varicose veins in the lower extremities. It is not known if a refluxing vein would have worst outcome than a normal vein. However, the former would be preferred over a prosthetic graft.
The distribution and clinical impact of phlebosclerosis was reviewed by Tzogias et al. 16 The inflammatory aetiology of the disease resembles the chronic vein wall changes secondary to deep vein thrombosis or varicose veins. 16 Interestingly, calcium deposits are commonly found in arteries; however, calcification is very rarely present in vein wall. Recently, Caggiati and Franceschini 17 reported a cartilaginous metaplasia likely originating from thrombus in a patient who previously had an episode of thrombophlebitis. Often, calcification of the vein wall is found in mesenteric veins. The authors speculate if similar findings of inflammation, leucocyte infiltration and expression of growth factors would be amplified promoting a more intense reaction causing vein wall calcification. 17
Affected veins can be found in the mesenterium, portal vein and in the extremities. 16 Frequently, the clinical presentation of mesenteric phleboscleroris is abdominal pain, nausea, vomiting or even bowel wall ischaemia leading to perforation. 18 Idiopathic portal vein hypertension and other similar disease such as non-cirrhotic portal vein fibrosis or haepatoportal sclerosis are known to cause portal vein phlebosclerosis. The promoters of sclerotic portal vein wall changes are not clear but its impact on morbidity and mortality in orthotropic liver transplant patients has also been reported. 19 The incidence and clinical significance of phlebosclerosis in lower extremity is unknown. In addition, the fact that not all refluxing veins have fibrotic wall changes despite the severity and duration of reflux pose some question why some veins are more prone to become sclerotic than others.
We were able to investigate prospectively vein wall sclerosis in 1000 limbs and compare them to healthy individuals and patients with chronic venous disease (CVD). Our study showed that sclerotic changes in the venous wall were found in all superficial veins but with greater incidence in the SSV. Nonetheless, the exact causes for a potential predilection of SSV to fibrous degeneration remain elusive. There are several implications of knowing that all superficial veins may be affected by phlebosclerosis because not only the saphenous veins are utilized for bypass surgery. Other superficial veins are also important such as the cephalic and basilic veins that are the main outflow for haemodialysis access in the upper extremity.
The distribution of sclerotic veins between men and women was similar in our study. This finding suggests that sclerotic changes in the vein wall may not be related to hormonal changes as seen in varicose veins but may be multi-factorial. In a recent study analysing 78 toe/leg amputation specimens in patients with diabetes or ischaemic ulcers demonstrated that the risk of developing phlebosclerosis was associated with development of atherosclerosis and end-stage renal disease. 20 Nevertheless, a correlation between advanced atherosclerosis disease and extent of phlebosclerosis including vein wall calcification as severe phlebosclerosis could not be demonstrated. The role of vein wall calcification remains unknown; however, reports of mesenteric vein wall calcification predisposing episodes of venous rupture have been described.
It seems that age and venous reflux are important factors as both the patients and the control group 1 were affected by phlebosclerosis but not the control group 2. Wall fibrosis is known to affect both arteries and veins with increasing age. Also venous hypertension has been shown in humans and animal studies to cause sclerosis in the vein wall. Therefore, our findings confirm histological work and open a window to identify such changes with high resolution DU.
To our knowledge, this study is the only contemporary work assessing the prevalence, distribution and extent of phlebosclerosis utilizing current DU technology. Previous studies were based on surgical and autopsy material, and old DU devices which somehow limits the evaluation of the vein wall. We found that the prevalence of phlebosclerosis in the lower extremities appears overall to be low in patients with venous disease or in healthy volunteers. Further investigation is still warranted in order to elucidate the clinical impact of this entity in the general population.
This study is limited by the absence of histological data. However, only patients with overt changes were included and in this regard the prevalence of phlebosclerosis has been underestimated.
Conclusion
The prevalence of phlebosclerosis in the lower extremities appears to be low with no significant sex differences. Thrombosis or reflux is not present in all cases of phlebosclerosis; however, older age and CVD are important for its development. The SSV is the most common site affected by phlebosclerosis in the lower extremities but all other superficial veins may be affected.