
Abstract
Pulmonary embolism is the first presentation in 70–80% in patients with aneurysm of popliteal vein. We present a case of young man admitted in our hospital with respiratory distress, tachycardia and D-dimer >3000 mg/dL. The observation of pulmonary embolism required the placement of a caval temporary filter before the surgical treatment. The use of temporary filter is recommended in symptomatic patients for thromboembolic phenomena, and when ultrasound detects the presence of floating thrombus.
Introduction
Aneurysms of the popliteal vein are rarely observed but may represent a source of pulmonary embolism (PE).
From literature, 1 only small series are reported up to 120 with a slight female and left-side preponderance. Their presentation varies from incidental observation during Doppler ultrasound examination or the onset of swelling in the popliteal fossa, until the acute thrombosis complicated by PE and death.
PEs is the first clinical presentation in 70–80%. 2
These aneurysms can be saccular or fusiform in shape with fibrosis and loss of smooth muscle layer or with thickening of the media, with or without inflammatory infiltrate.
There is only one case reported of a femoral vein aneurysm complicated by PE, in a patient with Churg-Strauss syndrome. 3
The present case showed histopathological features of the hypereosinophilic infiltrate, complicated by acute thrombosis followed by bilateral PE.
Case report
A 38-year-old man was admitted to the emergency room, with a 12 hours respiratory distress and tachycardia.
D-dimer was > 3000 mg/dL and arterial partial pressure of oxygen was 50.
The electrocardiogram showed sinus tachycardia with inverted T waves in V1 and the echocardiography demonstrated an acute right ventricular overload.
The lower limbs appeared normal, without swelling.
ColourDuplex sonography revealed a partially thrombosed popliteal vein aneurysm.
Computed tomography (CT) scan demonstrated signs of bilateral PE and confirmed a partially thrombosed saccular aneurysm of the right popliteal vein (Figure 1), with diameter of 40 mm and 85 in length.
Positioned temporary caval filter
The patient underwent urgent placement of temporary caval filter (Figure 2), thrombolysis with urokinase 100,000 IU into pulmonary artery and intravenous heparin (25,000 IU/day) with improvement of clinical condition in few days.
Computed tomography scan of right popliteal aneurysm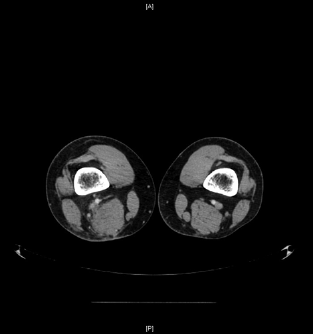
Control CT scan at one week showed slight reduction in the radiological signs of PE.
Laboratory tests revealed a mild hyperhomocys-teinemia and the MTHFR mutation in heterozygous form; negative ANCA (antineutrophil cytoplasmic antibody) associated with systemic vasculitis.
After 15 days, temporary caval filter was removed and the patient was discharged with warfarin and re-admitted after three weeks with normal respiratory parameters, but with a floating thrombus in the aneurysm sac.
The patient received another temporary caval filter and was submitted to removal of the aneurysm replaced by contralateral great saphenous vein (GSV).
Angiography in second day demonstrated a caval thrombus trapped into the filter.
Locoregional urokinase infusion (70,000 IU/hour) was protracted for 48 hours until complete lysis of thrombus, with subsequent removal of the filter and warfarin again.
Hystopathology revealed fibrous myxoid degeneration of the wall and focal calcifications, pictures of re-vascularization of the fund and luminal thrombosis, intense transmural inflammatory infiltrate of the muscular part of the vessel with abundant eosinophilic component.
Postoperative course was uneventful.
The patient discontinued warfarin after 18 months and shifted with Aspirin, re-starting active sport performances without symptoms.
Duplexscan examination at 36 months showed a regular size (8.8 mm), patency and continence of venous graft.
Discussion
Venous aneurysm is a rare clinical observation, generally asymptomatic; it occurs more frequently in women, 75% over 40 years old (7–69). Up to 70–80% of cases, the first symptom is a complication.
Grice in 1990, in a review of the literature, reported 12 cases of popliteal vein aneurysms, 11 of whom presented with pulmonary embolization.
In asymptomatic patients, their recognition is made possible through extensive use of the Duplexscan of the lower limbs. 4
Aetiology is mostly unknown and it is represented by isolated areas of dilation, not associated with arteriovenous communications or pseudo-aneurysms.
Hypereosinophilia may cause release of eosinophilic cationic proteins (ECPs, Mbps, EDN, EPO) and stimulate high platelet aggregation.
Moreover, the eosinophils stimulate high antibody response and also induce the endothelium damage and consequent venous wall expansion, reduction of the intraluminal venous pressure and slowdown in the flow, resulting in further thrombosis.
The indication for surgical treatment is widely accepted in case of PE or sac larger than 2 cm, while it is not univoque in case of asymptomatic aneurysm, without intraluminal thrombus, occasionally observed. 5
Surgical treatment usually consists of aneurysm resection and replacement with a segment of autologous GSV or poly(tetrafluoroethylene) or, more rarely aneurysmorraphy, especially in case of saccular aneurysm.
The use of temporary caval filter protection is not uniformly adopted, and indeed is reported only in four cases; it should be recommended even in symptomatic patients for thromboembolic phenomena and, as described in a few cases, even during oral anticoagulation therapy.
In the present case, the ultrasound observation of floating thrombus despite OAT (oral anticoagulation therapy) led us to relocate a new and temporary caval filter before submitting to surgery.
The finding of thrombus in the filter is the demonstration that this approach is correct in order to avoid severe complications in the perioperative.