
Abstract

Congenital vascular malformations (CVMs) represent a group of vascular anomalies that are the result of defective development of the vascular system. Therefore, a CVM presents at birth as an inborn vascular defect arising from the various stages of embryogenesis and may involve one or more components of the peripheral circulation systems: arterial, venous, lymphatic and capillary systems. 1
Naturally, the CVM may occur at different locations, conditions, shapes, extents and severities as one independent and predominant lesion (e.g. venous malformation) or as a mixed lesion with two or three different types of CVMs (e.g. haemolymphatic malformation). Hence, the CVM is a mixture of various vascular defects with different characteristics and behaviours, and often affects more than one vascular system; capillary, arterial, venous and/or lymphatic system. 2
The CVM remains a most difficult and confusing diagnostic and therapeutic clinical entity due to the wide range of clinical presentations, degree of severity, location, unpredictable clinical course and erratic response to treatment with high recurrence due to its embryonic characteristics. To add to the confusion, around the turn of the century, most CVM conditions were initially described using name-based eponyms to describe a syndrome based on the clinical presentation (e.g. Klippel and Trenaunay syndrome; F P Weber syndrome; Servelle and Martorell syndrome; Hippel and Lindau syndrome and Sturge–Weber–Krabbe syndrome). 3
Such old nosology and terminology of CVMs without proper information on aetiology, anatomy and pathophysiology failed to describe the appropriate defining characteristics among the CVMs. This old classification was based on clinical presentation alone and therefore was unable to provide proper anatomical and pathophysiological information that is required for evaluation, diagnosis and treatment. 4
Hence, a new classification of CVMs was developed in order to adequately describe the anatomy and pathophysiology of these lesions. An initial classification of these CVM lesions was described by Malan and Puglionisi in 1964. They made the distinction between the different CVM types such as venous, arterial and other associated malformations for the first time. They also described a lesion involving the main vessel trunks and a peripheral lesion as separate entities. 5
Subsequently, the Hamburg Classification was formulated during a workshop held in Hamburg, Germany, 1988. It was further modified to improve its clinical applicability providing additional critical information taking into account the stage during which developmental failure occurred during embryogenesis (Table 1).
ISSVA classification of vascular anomalies
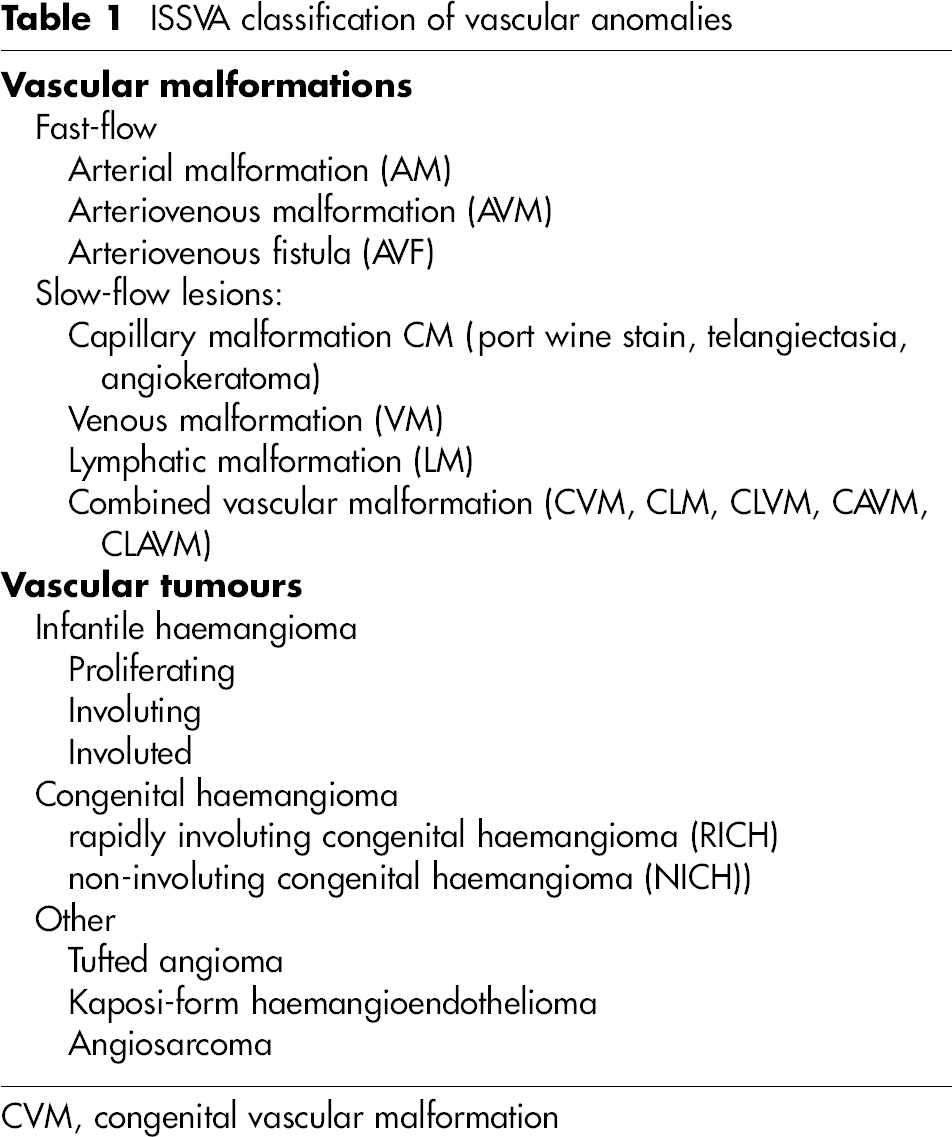
CVM, congenital vascular malformation
Meanwhile, further efforts were soon made by Mulliken et al. to differentiate two different kinds of vascular anomalies, the vascular malformation and vascular tumour (haemangioma). Both conditions are fundamentally different, not only from an anatomical, histological and pathophysiological standpoint, but also in their clinical behaviour. A haemangioma is a ‘self-limited’ vascular tumour, and vascular malformations are ‘self-perpetuating’ embryological tissue remnants. 6
Mulliken also proposed a simple classification of the vascular malformation based on the flow characteristics: fast-flow and slow-flow lesions with additional subgroups. This idea was adopted together by the ISSVA (International Society for the Study of Vascular Anomalies) and updated officially through 1996 as ISSVA Classification 7 (Table 2).
Hamburg classification*, modified
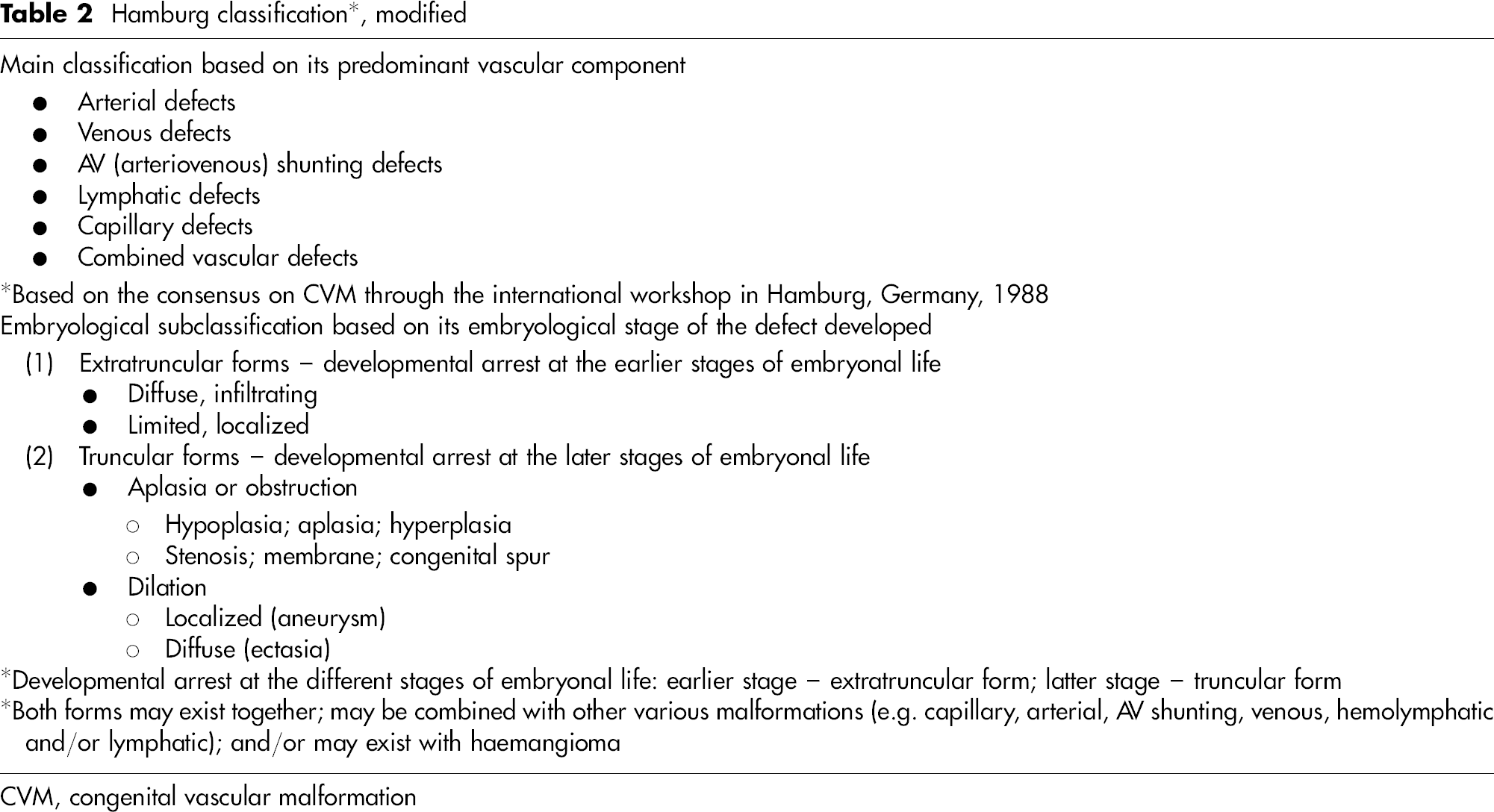
CVM, congenital vascular malformation
Up until then, the vascular malformation was often mistakenly referred to as a ‘haemangioma’, which is the most frequently misused term to describe the CVMs (e.g. ‘cavernous/capillary’ haemangioma). The haemangioma is not a CVM but a ‘vascular tumour’ of benign nature that originates from endothelial cells. It usually appears in the early neonatal period. Haemangioma has a distinctive growth cycle characterized by a proliferation phase of early rapid growth followed by an involutional phase of slow regression. Unlike CVMs, haemangiomas undergo self-limited growth followed by subsequent involution that usually occurs before the age of 5–10 years.
In contrast, the CVM is the result of a birth defect so that it continues to grow at a rate that is proportional to the growth rate of the body regardless of its type (venous, lymphatic, arterial, etc.). If the embryological defect occurred during the early stage of embryogenesis, the lesion will maintain its unique mesenchymal cell, angioblast characteristics. However, if the CVM embryological defect occurred during the later stage when the vascular trunk is formed, the lesion would no longer have its potential to grow (e.g. popliteal vein aneurysm and iliac vein stenosis). 8
Based on the potential to proliferate and grow when stimulated (e.g. menarche, female hormones, pregnancy, surgery and trauma), the group of the CVMs originating from the earlier stage of embryogensis was designated the ‘extratruncular’ type by Belov 6 in order to distinguish this type from the ‘truncular’ type of CVM lesion, that arises from the later stage of embryogensis (Table 2).
It is extremely crucial for clinicians to be aware of the potential for growth and proliferation of extratruncular CVM lesions in order to minimize the risk of recurrence and subsequent morbidity, in addition to its haemodynamic characteristics affecting each involved vascular component: arterial–venous–lymphatic system. Therefore, identification and confirmation of this embryological subtype is the first step towards the proper management of every CVM lesion. 9
Extratruncular type lesions have the potential to proliferate and grow when stimulated, resulting in recurrence!
All CVMs are not all same; arteriovenous malformation, venous malformation and lymphatic malformation are all significantly different from each other. They have entirely different clinical behaviour and prognosis. Subsequently, the management principle and strategy of each malformation lesion should be fundamentally different. 10 Therefore, the CVM is a vascular disorder of extreme variety with the stigma of ‘totally unpredictable’ behaviour. Recurrence has been a trademark of the CVMs and is often viewed as an enigma among the vascular disorders and has remained a significant challenge to clinicians throughout the last century.
Nevertheless, some have not yet accepted this embryological subclassification of the CVMs, raising doubt regarding its value, mostly based on their unfamiliarity with this new term: ‘extratruncular’ in particular. Although there is no objection of the concept itself, many people are not used to this terminology, especially the term ‘extratruncular,’ and are still more familiar with the old classification.
The main issue is not the pathology that produces the truncular or extratruncular CVM, but the morphology of the lesion and its clinical behaviour. Extratruncular lesions have a high tendency to progress/worsen or recur after treatment, while truncular lesions do not. According to the embryological concept, the worsening of the CVM lesions would depend on the type of endothelial cells present as remnants of the primitive capillary network that maintains the ability to proliferate and grow.
However, the growth tendency of extratruncular CVM can also be explained by the most recent genetic theory, based on gene mutations within the tissues. Identification of the causative genes in several defects has permitted more precise diagnosis. Further studies are necessary to better understand these mechanisms.