
Abstract
The aim of multislice helical computed tomography venography (CTV) is to provide a precise, global and three-dimensional (3D) anatomical depiction of the venous network of the lower limbs. A multislice and multidetector spiral CT acquisition of the lower limbs with contrast injection of the dorsal foot produces about 1000 slices in 30 seconds. Dedicated volume-rendering software can compute a realistic and interactive 3D model of the venous system in realtime. This new tool furnishes an accurate 3D representation of the whole venous system of the lower limb with a realistic 3D model of the limbs, providing a road map of the varicose networks complementary to the duplex ultrasound (DUS). CTV allows a complete morphological study of the deep veins, including the detection of anatomical variations and proximal venous obstruction, not easily detectable by DUS. In the case of deep vein thrombosis, it has been shown to be a good diagnostic tool, well correlated with sonography. It also demonstrates, in some cases, haemodynamic patterns which are not available by DUS, particularly for perforator veins and congenital vascular malformations. The use of virtual reality techniques enables a complete anatomical study of both deep and superficial veins including a virtual dissection of the limbs. CTV is also a great educational tool to learn anatomy of the venous system and a powerful research tool to improve our knowledge of venous anatomy.
Introduction
The anatomy of the venous system of the lower extremity is extremely complex and variable. 1,2 This explains the need for even more global and morphologically accurate techniques for assessment of the vascular tree, especially in complex cases.
Traditional phlebography is no longer considered the gold standard for the morphofunctional examination of the venous network of the lower limbs because, in the majority of cases, duplex ultrasound (DUS) furnishes anatomical data and a complete haemodynamic evaluation.
Furthermore, DUS is essential to achieve a preoperative skin mapping, an essential guideline for the surgeon during an operation. 3
Recent advances in computer technology brought new imaging techniques for three-dimensional (3D) investigation of venous disease, based primarily on the use of computed tomography venography or CTV. 4–9 However, it gives no haemodynamical data, so an associated colour-coded duplex is mandatory.
CTV technique
Principle of spiral CT
The spiral or helical CT scan is the result of two different techniques used in combination (Figure 1).
Principle of spiral multislice computed tomography (CT). Spiral multislice helical CT is the result of two different moves combined together: 1 is a rotation of an X-ray beam linked to an X-ray tube-detector apparatus, 2 is a translation of the table where the patient is lying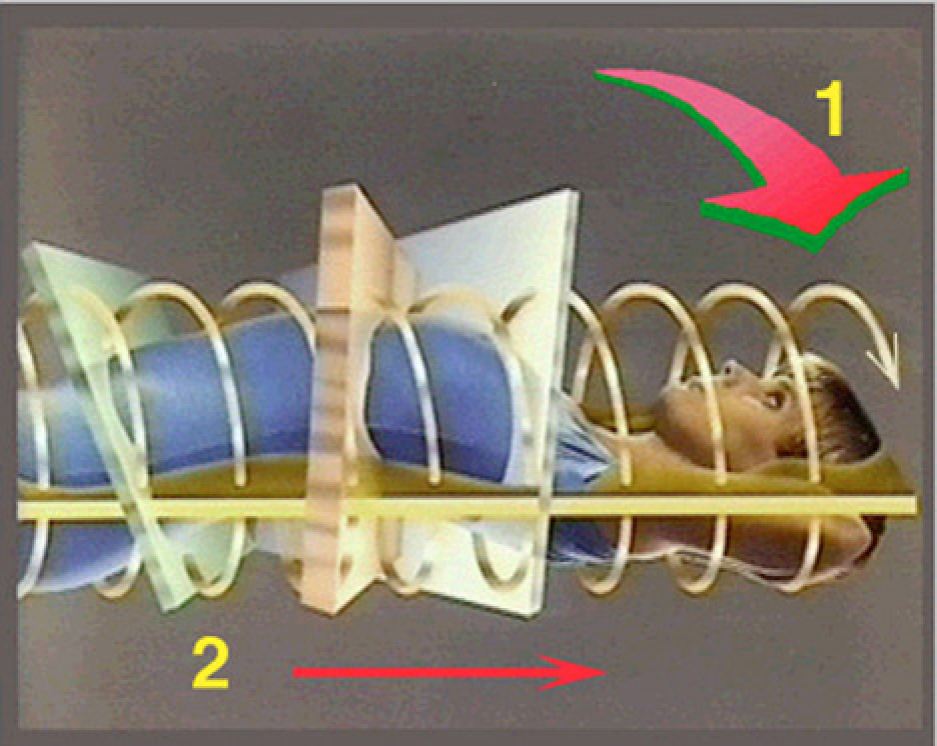
First, the rotation of an X-ray tube, attached with detectors, around the patient's bed.
Second, a continuous linear translation of the same bed. This enables the acquisition of spiral volumic data, resulting in many slices and 3D images by the use of dedicated reconstruction software.
Main steps of the computed tomography venography (CTV) technique
The three steps of the CTV investigation are data acquisition, reconstruction and postprocessing.
After treatment, reconstructed images and interactive movies are transmitted by intranet and can be seen on a notebook by the angiologist or the surgeon (Figure 2).
The three steps of the computed tomography venography technique: 1 = multislice helical computed tomography acquisition with venous injection; 2 = three-dimensional (3D) reconstruction by a dedicated volume rendering technique software on a workstation; 3 = interactive display on a notebook of 3D movies (Quicktime® virtual reality)
Data acquisition
Multislice and multidetector spiral computed tomograph protocols

CT, computed tomography; VRT, Volume rendering technique; MDCT, multidector computed tomography; MCT, multislice CT (MSCT)
The timing of injection is essential. The contrast injection should begin about 40–60 seconds before, and then has to be synchronized with the acquisition, in order that it finishes at the end of the acquisition.
The patient is lying on their back (feet first), with no contact point with the table except for the buttocks and heels. It is important to avoid any compression of the calf and posterior thigh during acquisition time. The patient has to hold perfectly still during this short time and is often asked to do a Valsalva manoeuvre.
Data reconstruction
Raw data are processed to perform slices reconstruction. See usual protocols on Table 1.
Postprocessing of the data
3D reconstruction of the venous system is performed.
The data are usually sent by intranet on a dedicated workstation for postprocessing using dedicated 3D reconstruction software.
Surface rendering technique (or surface shading rendered): There has been tremendous progress for 3D image reconstruction over the last two decades. At the beginning, a manual segmentation of the image was necessary to obtain a reconstructed 3D image using a surface shading rendered 3D model. In fact, a pixel extraction had to be done using an appropriate windowing: the maximal minimal density threshold was chosen manually in order to select the voxels corresponding to an anatomical structure. Although performed on powerful Sun or Silicon graphics workstations, this technique was time consuming and used only a part of the data.
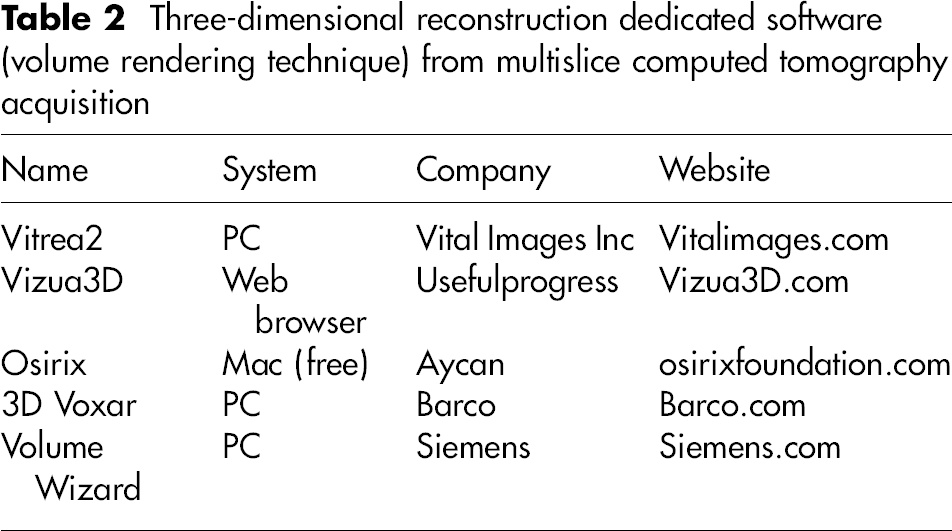
Volume rendering techniques: Today, beautiful 3D images of the venous system are quickly produced by reconstruction with volume rendering technique (VRT) with easy to use built-in protocols. This saves time and takes full advantage of the whole 3D information available in the data-set. New dedicated three-dimensional software, running on a PC with at least 2 GB of RAM, are now available for this purpose.
Main functions of VRT: Rotation, tilt, pan, zoom and use of different transparencies of the tissues in realtime. Automatic pre-sets are available to directly visualize skin, muscles or vessels. Quick and easy image capture or animation. Output functions easily transmit images to a PC.
Three-dimensional reconstruction dedicated software (volume rendering technique) from multislice computed tomography acquisition
Other technical points
Direct contrast medium injection
A direct injection of diluted contrast is preferred in order to enhance the contrast of venous network, allowing the display of it alone without the surrounding tissues (with the VRT software using automated pre-set protocols). This is also true for perforators: their course and precise connection with the deep veins are to be checked before surgery. Lastly, it is mandatory to investigate the detailed morphology of the deep system in any chronic venous disease (CVD) patient.
Venous puncture
A dorsal foot vein puncture is performed in most cases. In selected cases, the punture of a varix of the leg or thigh may be used to opacify a varicose network of the root of the limb, a pelvic varix, a pelvic origin of the reflux or to show an excluded varicose territory.
Technique of injection for varicose veins investigation
We use an automated Medrad MCT injector system. A uni-phasic injection of 20 mL of iodine contrast medium is done in 180 mL of serum, at the rate of 2–3 mL/second. The duration of injection (usually 1 minute) is synchronized with acquisition time: starting about 30 seconds before and lasting until the end of the acquisition.
Of course this timing and the site of injection depends on the investigation being conducted.
Techniques of optimization have been proposed, particularly those to reduce the amount of X-rays delivered, mainly for the investigation of deep vein thrombosis (DVT). 10–15
Optimization of the deep system assessment can be done using a bi-phasic injection (better to visualize iliac or pelvic veins). Abdelmoumene et al. 15 have also proposed wearing of elastic stockings.
The volume and perfusion rate of contrast medium are dependent on the area being investigated (more for the limb's root and pelvic areas).
For DVT detection it is widely agreed to obtain an indirect CTV by brachial venous injection.
However, we think that the filling of the veins and the quality of the images is much more reliable with a direct CTV with injection of the foot or leg.
Associated techniques
Associated techniques can be used to enhance the contrast. Patients are often asked to perform a Valsalva manoeuvre. A balloon placed in the supra-iliac area, inflated during acquisition, will enable better evaluation of the femoral and iliac veins.
The use of a tourniquet and its location are important, depending on the investigation to be done:
The tourniquet is usually placed at the root of the thigh when investigating the popliteal area. It should be placed above the ankle for better filling of the deep veins.
3D imaging of the venous tree can also be obtained without contrast medium injection. 16 This contrastless CTV is sufficient for the superficial network, but not suitable for the perforator veins and the deep trunks.
Methods
Transmission of 3D images to the specialist
The slices and a selection of 3D reconstructed images can be saved on a CD, but the best way to achieve data transmission between the radiologist and the angiologist is to export the movie files of a rotating 3D model using different transparencies of the tissues: skin, muscle and vessels (Figure 3). These dynamic data are easily built and exported by VRT software, as images or rotational movies.
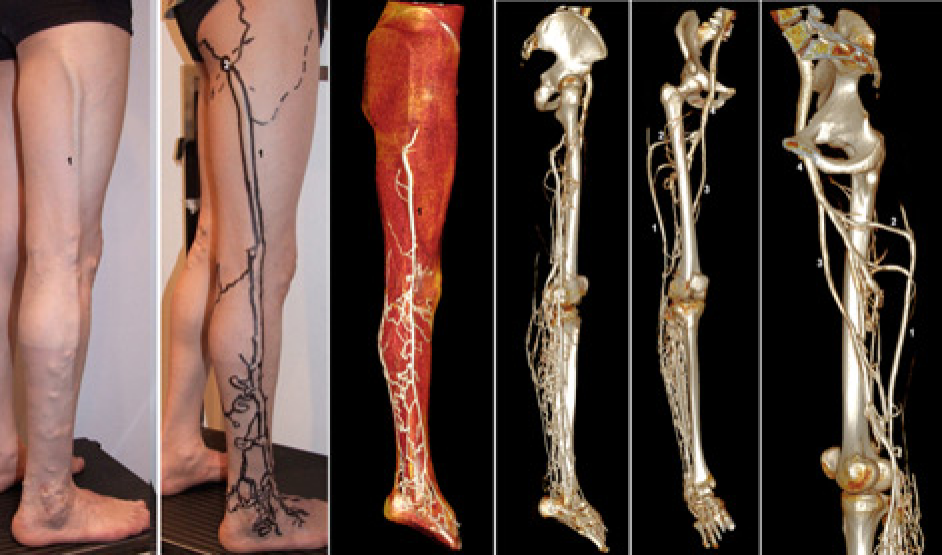
Volume rendering, different transparencies of the tissues: skin (a), muscles (b), bones and venous network (c) are available by simple modification of the threshold using automatic pre-sets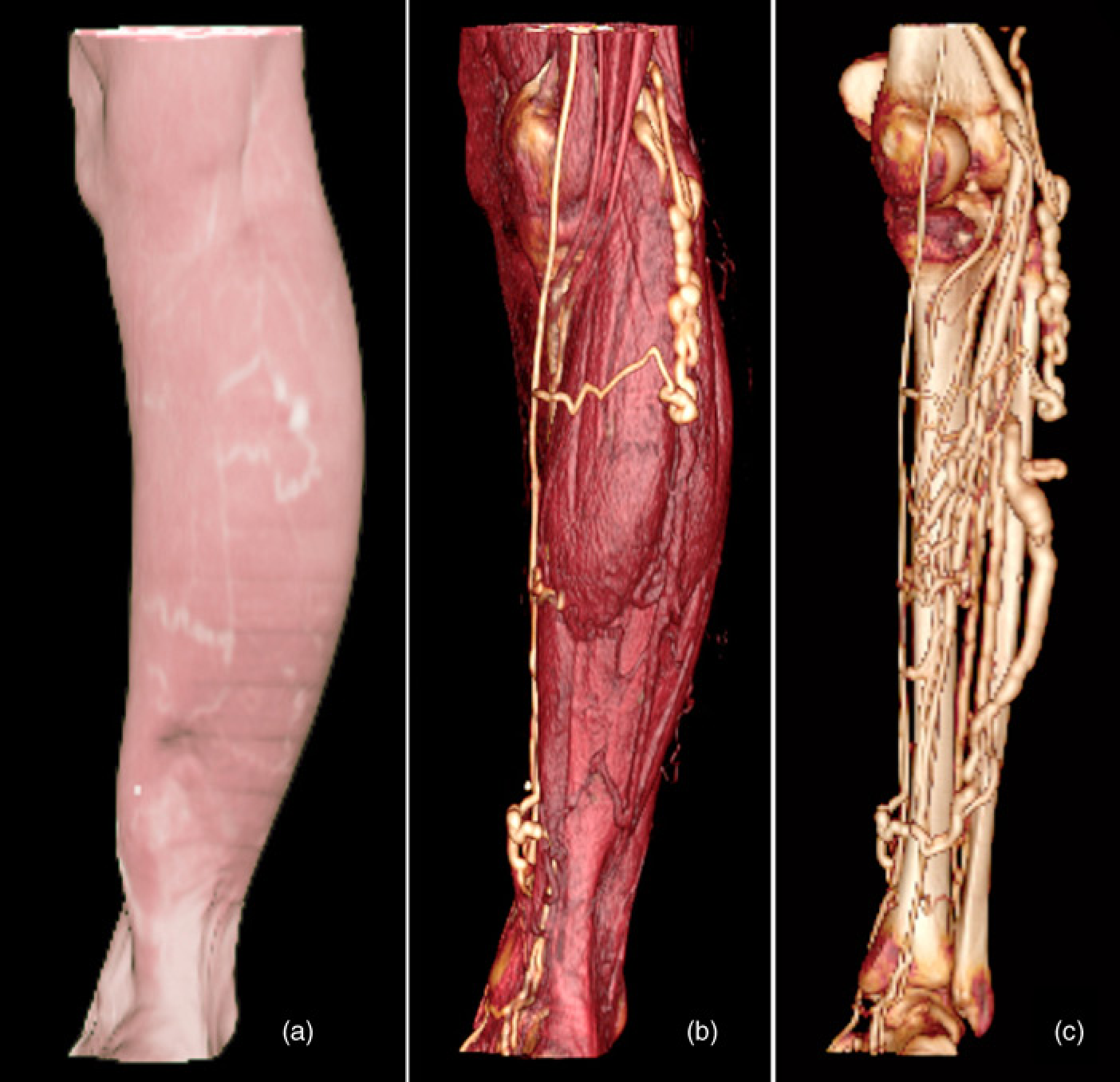
One of the best methods is to use the Osirix® software 17 to export movies of the 3D model and then to display it in the software Quicktime virtual reality from Apple®. It achieves a true interactivity with a rotation of the 3D model with horizontal movement of the mouse, and modifying tissue transparency with vertical movement of the mouse.
Another way to transmit the data is to produce a virtual trip along the venous network, which is also possible with Osirix®. Other software is also available for that function, particularly a new one working on an iCloud server, Real-scan or Vizua3D® produced by Useful Progress company, 18 45 rue des saints Pères – 75006 – Paris (University Paris Descartes).
For the investigation of varicose veins before surgery
Because of the exquisite depiction of venous anatomy it produces, VCT may help avoid the anatomical pitfalls of venous surgery. This enables better surgical strategy, and a more accurate and focused skin approach. Accordingly, it improves the aesthetic result as well as efficacy, reducing the varicose vein recurrence rate and enabling a quicker return to normal activity.
In this way, the surgeon can have the entire information from the VCT available on a laptop in the operating room, together with the data of paper cartography and of the DUS skin mapping. 3,4 These tools can be used together to create a roadmap for venous surgery.
CTV indications and results
For anatomical studies and research
Our methodology, used since 1994, includes four steps using fresh cadavers:
Injection of the venous system of the lower limb with latex mixed with minimum 1% or contrast iodine; CTV of the injected cadaver's limbs; Anatomical dissection of the limbs including coloured segmentation (painting of the veins). This is the usual technique used in the atlas book of the superficial venous network of the lower limb by Claude Gillot;
1
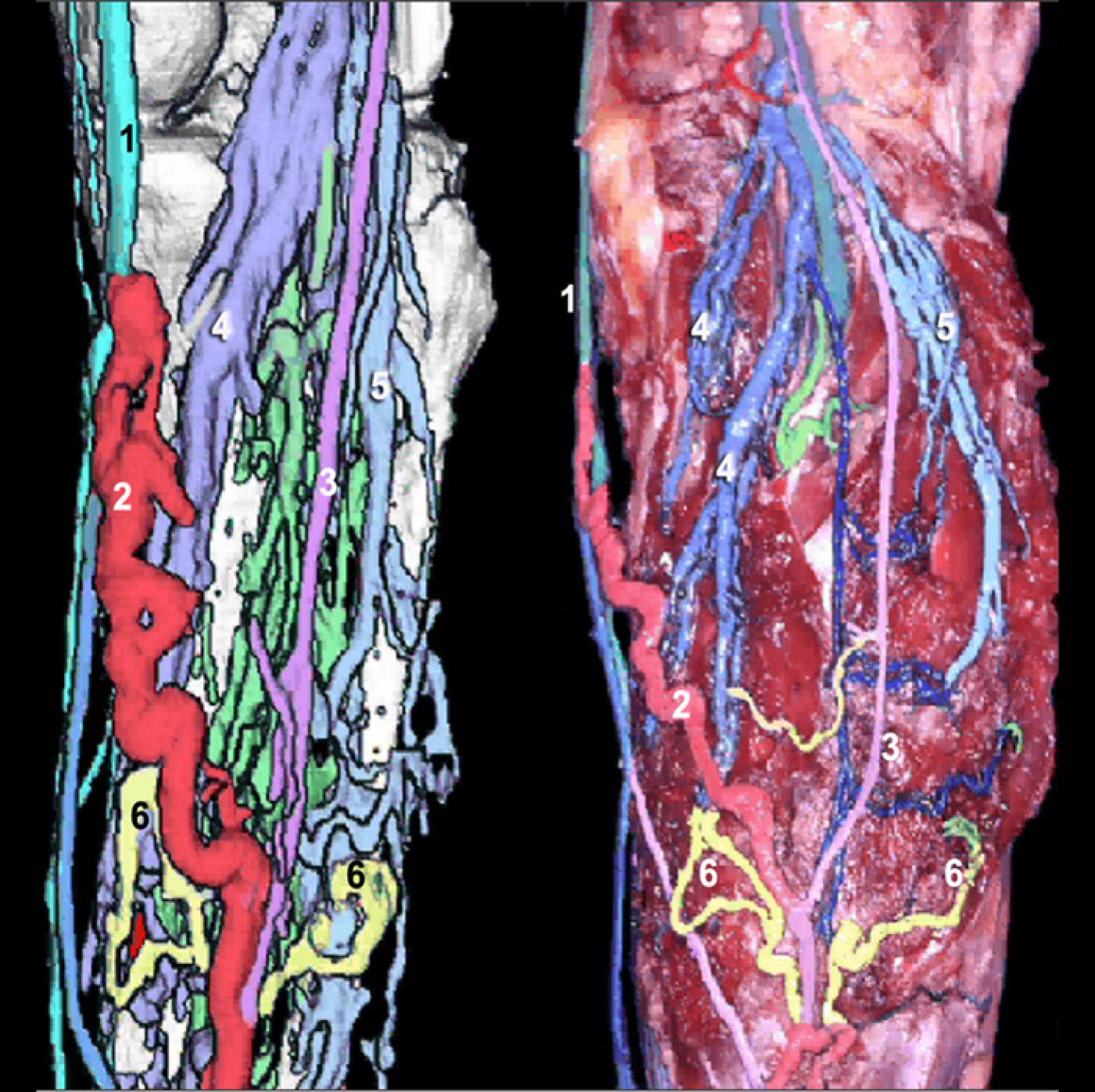
3D reconstruction using VRT technique after segmentation of the model. Comparison of the three-dimensional (3D) model with an anatomical dissection of the same leg. On the left the 3D reconstruction obtained by surface shaded rendering, on the right the coloured segmentation of the veins after dissection. In light blue (1) the great saphenous vein. In red (2) a communicating vein of the calf. In purple (3) the small saphenous vein. In blue the gastrocnemial veins medial (4) and lateral (5). In yellow (6) the perforator veins. Please notice that the connection between the perforators and the gastrocnemius veins are termino-terminal
Evaluation of the two techniques with comparison of the corresponding veins confirms good accuracy of CTV 3D models, and validates their clinical use (Figure 4).
For clinical applications: investigation of patients
Preoperative assessment of primary CVD patients
Since 1995 we have investigated complex or recurrent varicose patients.
CTV is now proposed for 10–15% of our patients before surgery.
2–6
It is particularly indicated in the following cases:
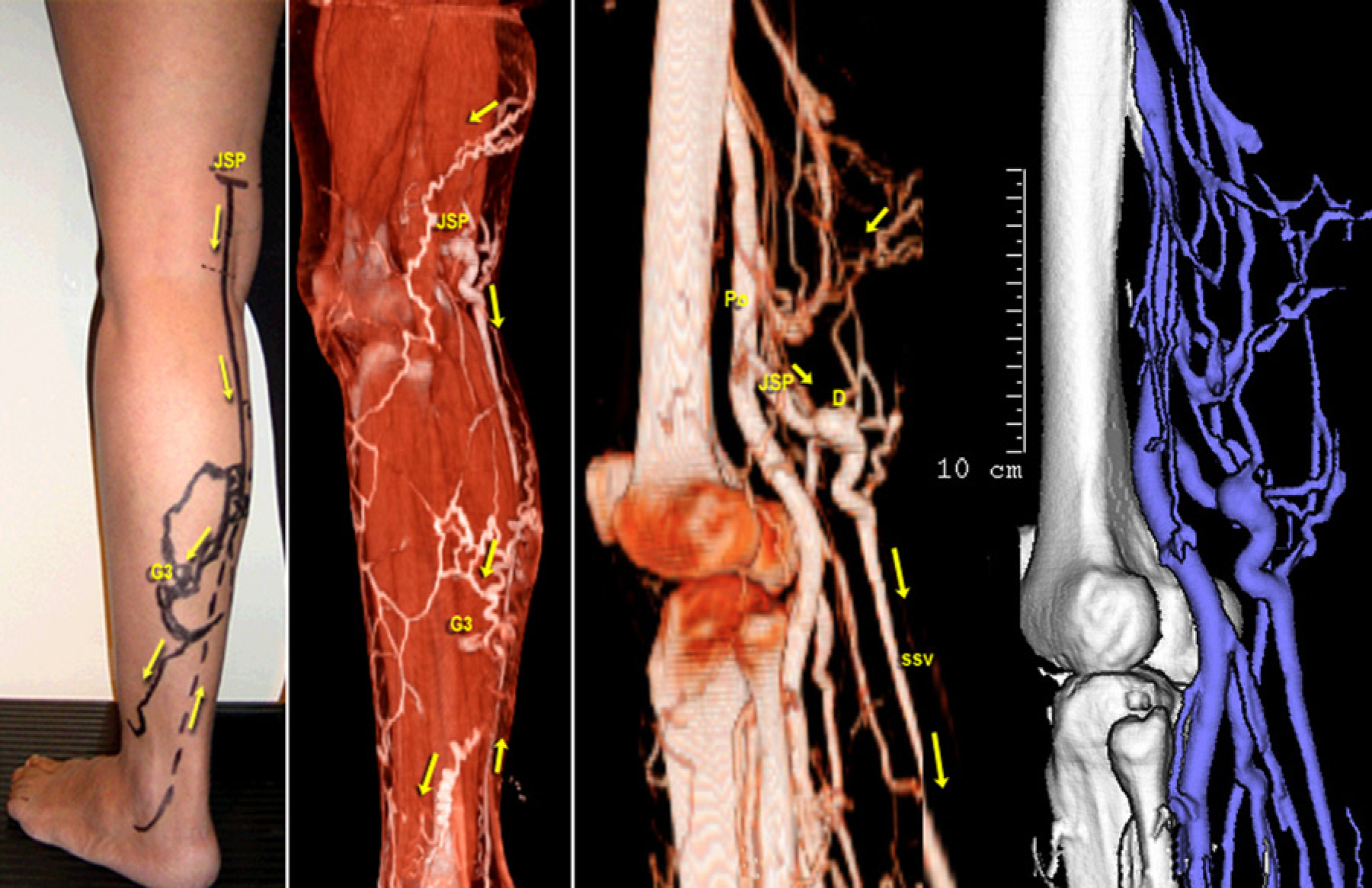
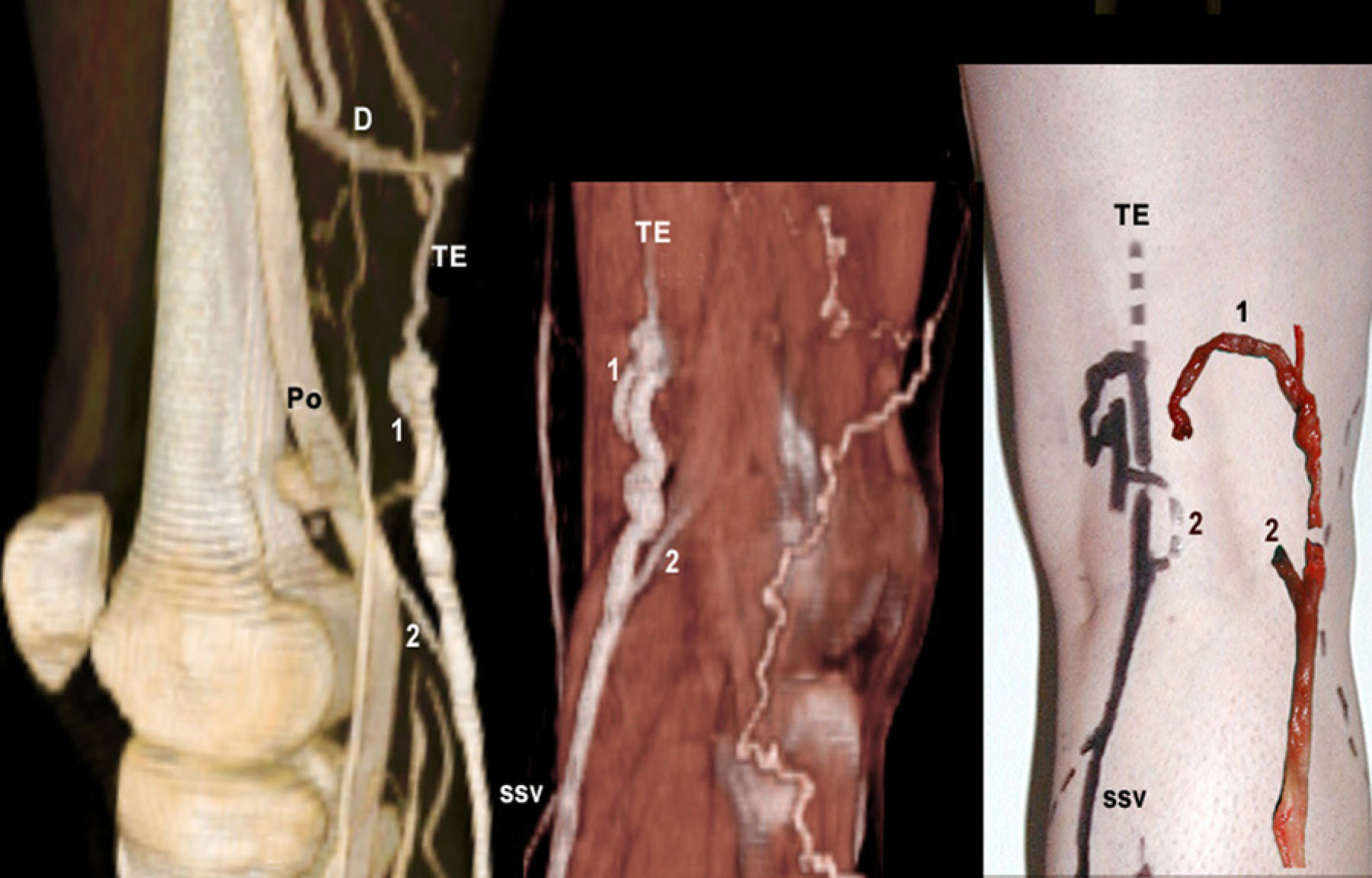
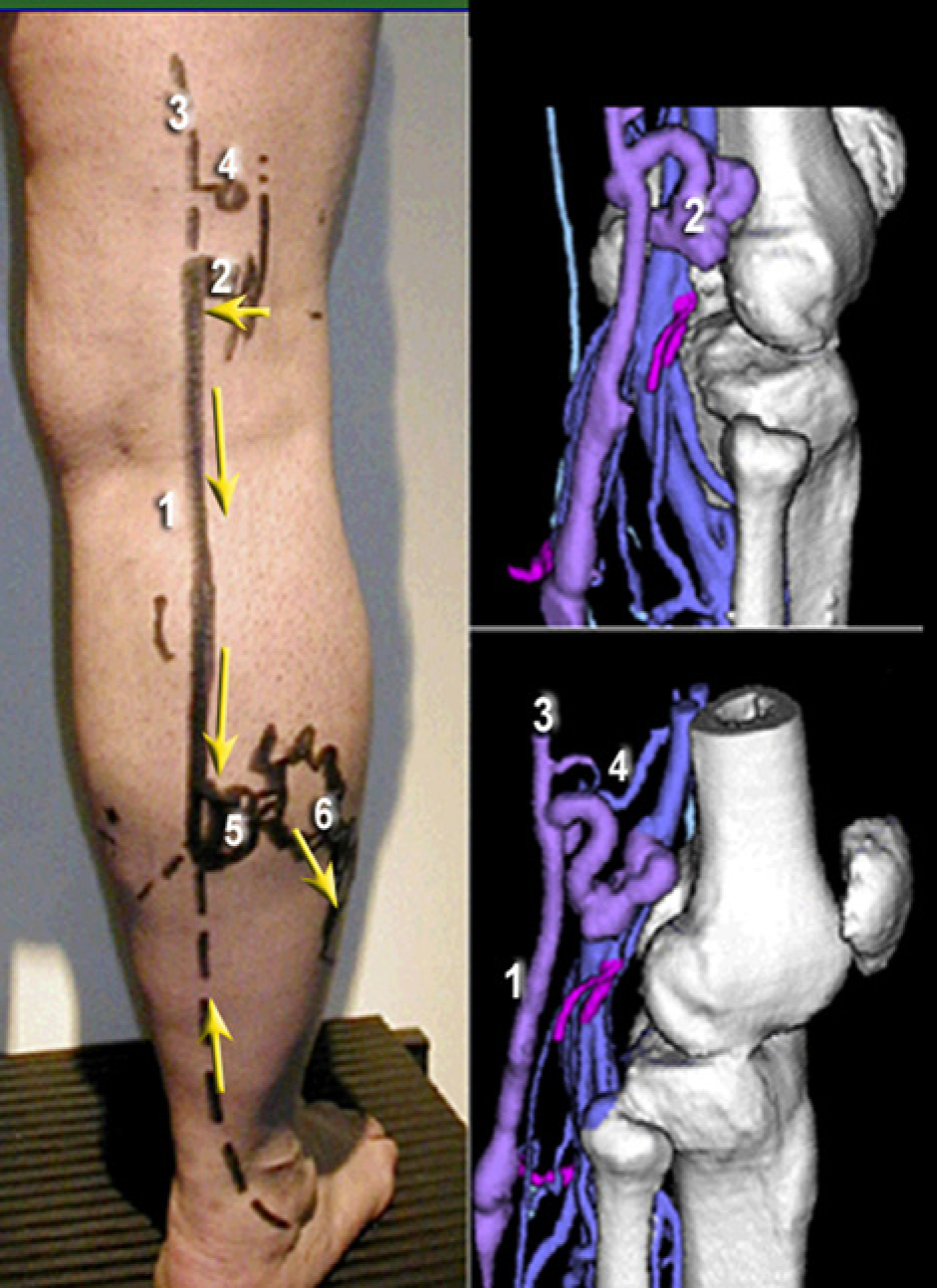
Neovascularization of the groin after great saphenous vein (GSV) surgery, or nodal dystrophic networks (Figure 5); Postoperative recurrence of the popliteal fossa (Figure 6); Perforators of the popliteal fossa (Figure 7); The small saphenous vein (SSV) should be investigated by CTV in cases of high termination (Figure 8), abnormal termination with two saphenous popliteal junctions (Figure 9) or dystrophic termination (Figure 10). Some authors recommend CTV to investigate all SSV patients prior to surgery;
19
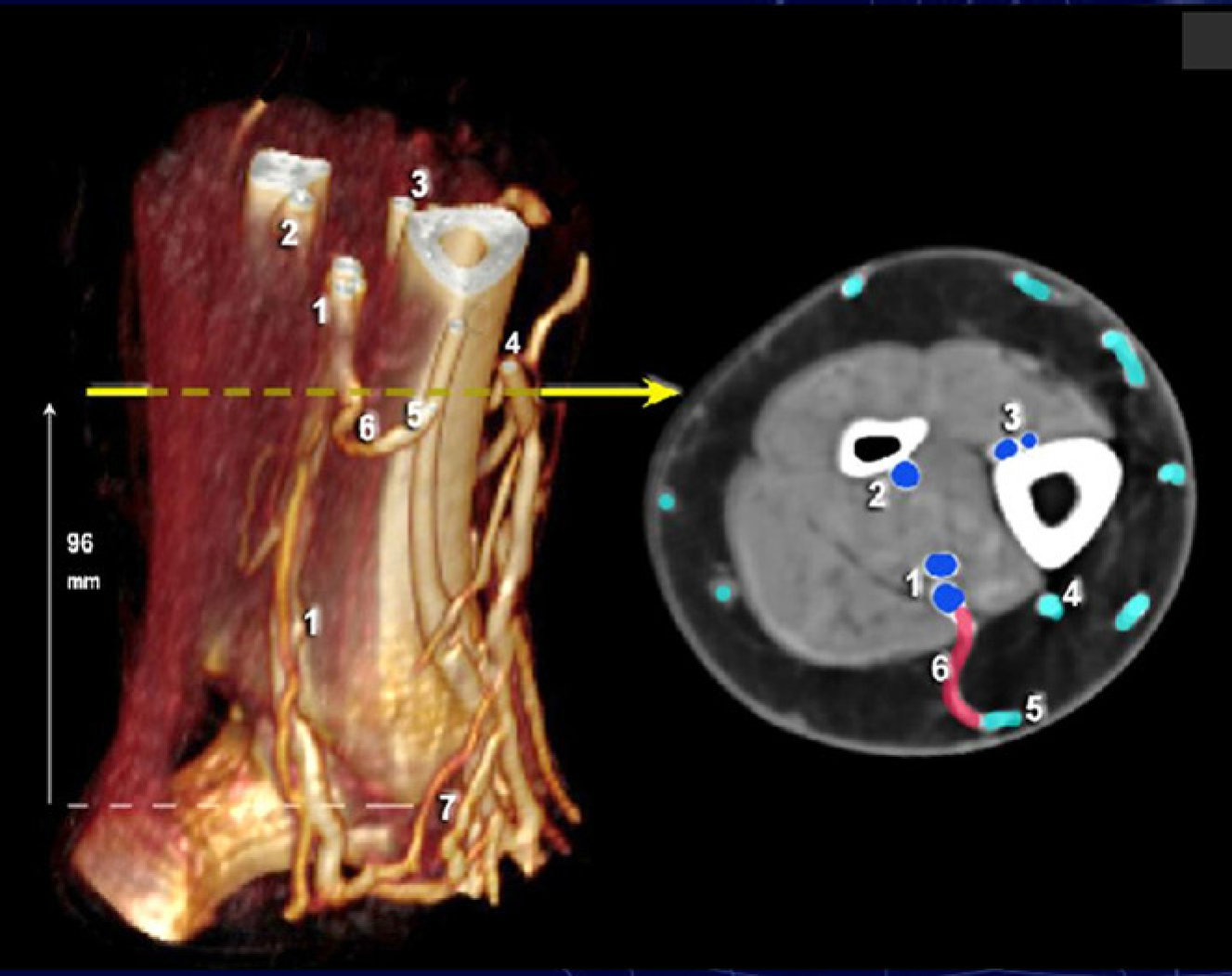
Varicose veins of the great saphenous territory fed by an ascending flux of the Giacomini vein via a saphenous popliteal reflux (Figure 11); Large and complex varicose networks of the leg and foot (Figure 12), particularly if there are skin changes, to improve venous mapping; CTV provides more precise information regarding the course of perforator veins: large perforators of the thigh (Figure 13). Perforators of the medial leg (Figure 14), and perforators of the foot and ankle not easily assessed by DUS (Figure 15). Three-dimensional reconstruction of the nodal network of the groin surrounding the termination of the great saphenous vein (GSV). The veins crossing through the nodes are easily identified. 1 = GSV; 2 = sartorius muscle; 3 = superficial epigastric vein; 4 = inguino-abdominal tributaries; 5 = anterior accessory of the GSV; 6 = femoral vein; 7 = femoral artery; G = inguinal nodes Investigation by computed tomography venography of a cavernoma of the popliteal fossa after recurrent varices after surgery (small saphenous vein surgery). (a) Three-dimensional (3D) reconstruction by surface rendering; (b) 3D reconstruction by volume rendering technique; (c) view during redo surgery; (d) skin mapping before operation. 1 = popliteal vein; 2 = cavernoma Case report of a patient with a popliteal fossa perforator vein feeding a varicose network of the calf. Please notice the small perforators (P) of the thigh not found during duplex ultrasound mapping. 1 = popliteal vein; 2 = femoral vein; 3 = popliteal fossa perforator vein; 4 = medial gastrocnemial vein; 5 = lateral gastrocnemial vein; 6 = deep femoral vein Case report of a high termination of the SSV: the saphenous popliteal junction (SPJ) is located 8 cm above the crease. SSV = small saphenous vein; D = dystrophic and dilated segment of the SSV termination; Po = popliteal vein. The arrows indicate the refluxing segments of the venous network with duplex ultrasound Case report of a complex termination of the small saphenous vein (SSV): you can see a duplicated arch of the SSV: 1 = lower crosse of the SSV; 2 = higher cross of the SSV; TE = thigh extension of the SSV (or dorsal or cranial extension); D = deep femoral vein; Po = popliteal vein. On the right the skin mapping with the veins removed Case report of a dystrophic and sinuous termination of the small saphenous vein (SSV). (Arrows indicate venous reflux with duplex ultrasound.) 1 = refluxing SSV; 2 = dystrophic termination of SSV; 3 = thigh extension of the SSV; 4 = perforator vein of the popliteal fossa; 5 = gastrocnemial perforator vein; 6 = varicose network of the lateral aspect of the leg Case report of reflux of the great saphenous vein fed by the Giacomini vein via the saphenous popliteal junction. Gs = great saphenous vein; G = giacomini; S = small saphenous vein; Co = communicating vein of the calf (arrows indicate venous reflux with duplex ultrasound) Case report of a complex network of the leg in a patient with skin changes. The black arrows show the dystrophic and refluxing venous network located in the area of the skin changes of the lower leg. The white arrow shows the precise location where the great saphenous vein is leaving the saphenous compartment, becoming an epifascial vein at this point. 1 = paratibial perforator vein; 2 = posterior tibial perforator vein; 3 = ankle perforator vein; 4 = infra-malleolar perforator vein Investigation by CTV of the perforators of the thigh: three-dimensional models and the two corresponding horizontal slices (1–2) a = femoral vein; b = popliteal vein; c = first trunk of great saphenous vein (GSV); d = duplicated trunk of GSV; e = axial vein (along the sciatic nerve) f = deep femoral vein; p1 = Hunterian perforator connected to the posterior trunk of GSV; p2 = Hunterian perforator connected to the anterior trunk of GSV Investigation by computed tomography venography of the perforators of the leg: here a posterior tibial perforator vein. 1 = the two posterior tibail veins; 2 = fibular veins; 3 = anterior tibial veins; 4 = great saphenous vein (GSV); 5 = tributary of GSV; 6 = posterior tibial perforator vein; 7 = infra-malleolar perforator vein Investigation by computed tomography venography of the perforators of the foot and ankle. Medial view (virtual reality technique), perforators are coloured in red, deep veins in dark blue, Great saphenous vein (GSV) in light blue, Small saphenous vein (SSV) in purple. T = tibia bone; C = calcaneus; 1 = great saphenous vein 2 = small saphenous vein 3 = medial marginal vein 4 = perforator of the first metatarsian space 5 = cunean perforator 6 = scaphoidian perforator 7 = para-achillean perforator (Bassi) 8 = infra-malleolar perforator







In all cases, CTV provides no haemodynamical data; the association with Colour-coded duplex of the venous network is therefore mandatory.
Special cases of CVD
CTV is especially interesting in the investigation of unusual causes of varicose veins. 20
Pelvic origin of varicose veins: Pelvic origin of varicose vein is not uncommon, and is responsible for specific symptoms and recurrences. 21,22
The use of colour duplex is mandatory to look for the link points inside the pelvis.
The main points are inguinal (Figure 16), perineal and obturator veins. A special type is fed by the inferior gluteal veins producing:
Case report of an inguinal pelvic reflux (point I of Franceschi)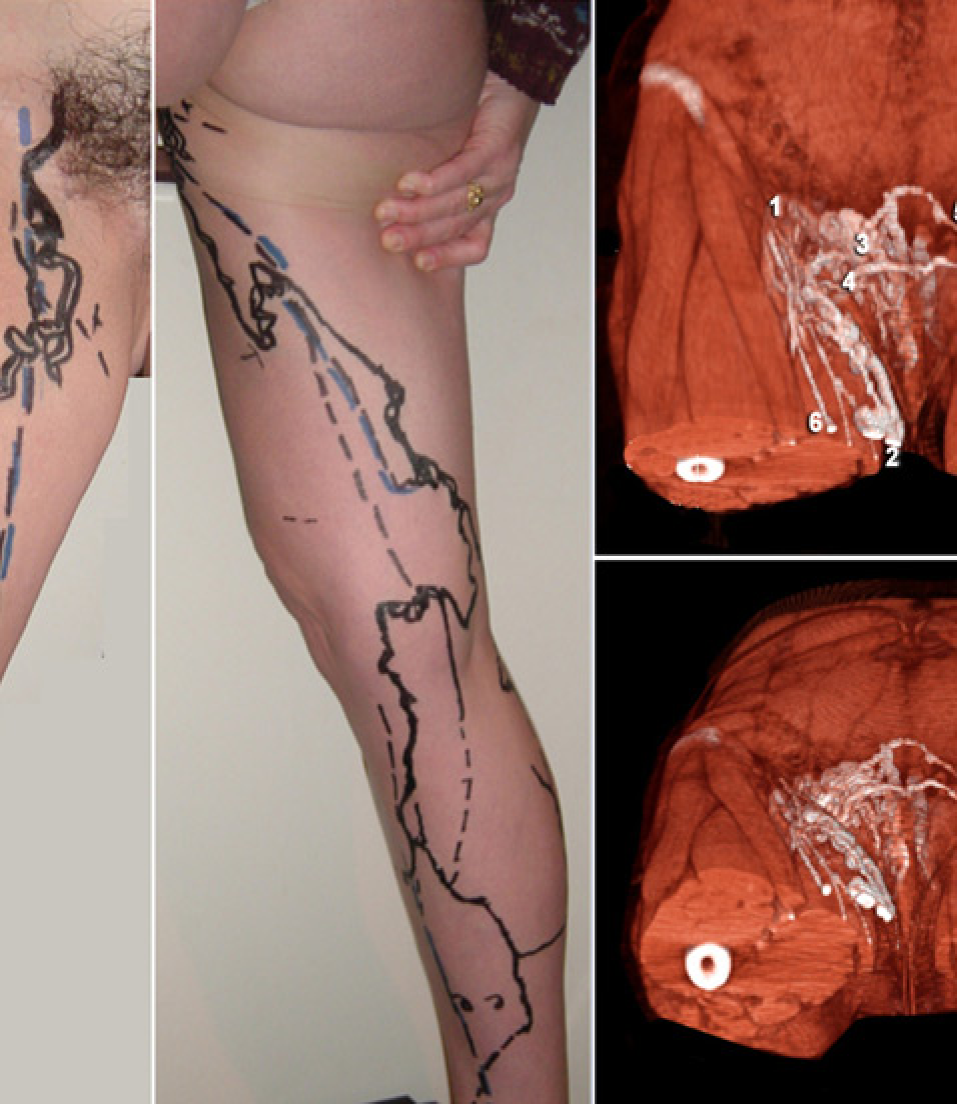
The varix of the sheet of the sciatic nerve: According to embryogenesis, sciatic nerve varices follow the route of the nerves: sciatic nerve at the thigh level, fibular nerve at the knee level and lateral saphenous nerve below.
23
CTV usually shows the deep route at the thigh along the sciatic nerve: on the 3D reconstructions as well as on the slices, the dystrophic venous network infiltrates the sheet of the nerve. It is associated here with stasis in the muscular arcades of the semimembranous muscle (Figure 17).
Computed tomography venography investigation of a varicose network of the sheet of the sciatic nerve. 1 = sciatic nerve (in yellow); 2 = varicose network surrounding the sciatic nerve. We can see on the slices that veins go inside the sheet of the nerve; 3 = dilated venous arcades of the semimembranosus muscle; 4 = femoral vein; 5 = semimembranosus muscle with several dilated veins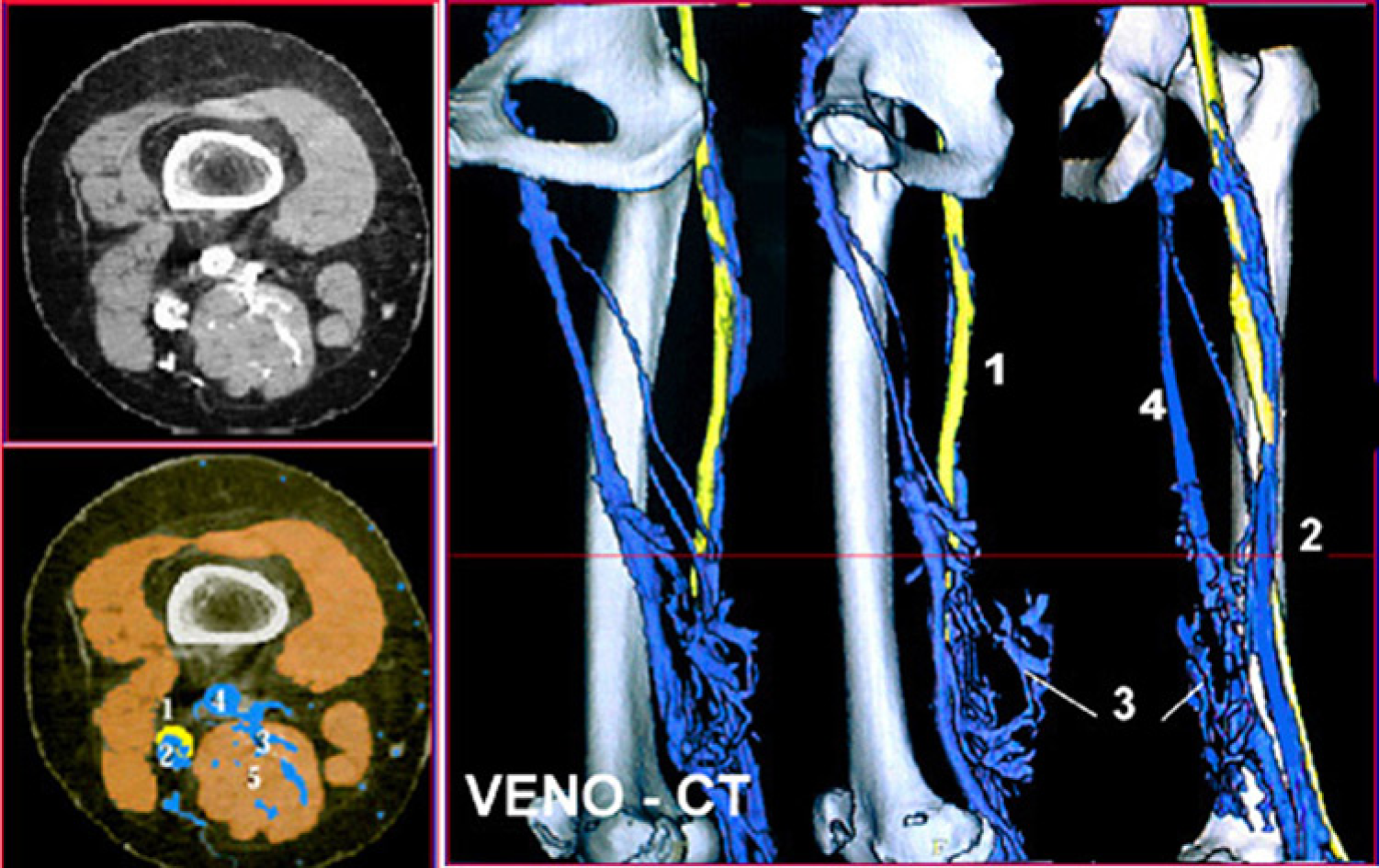
The connection with gluteal veins is often well demonstrated by CTV (Figures 18 and 19).
Three-dimensional reconstruction (left) and maximum intensity projection (right) of a varicose network of the sheet of the sciatic nerve. (Courtesy of Dr Kennedy Pacheco from Brazil.) We can see here the thin network of dystrophic branches (white arrows) surrounding the nerve. The reflux is mainly coming from the superior ischiatic vein (2). It is also connected to the femoral vein (5) and the deep femoral vein (6). 1 = common iliac vein; 3 = femoral vein; 4 = poplital vein Case report of another varicose network of the sheet of the sciatic nerve, showing the same path coming from the ischiatic vein of the pelvis (Courtesy of Dr Kennedy Pacheco from Brazil)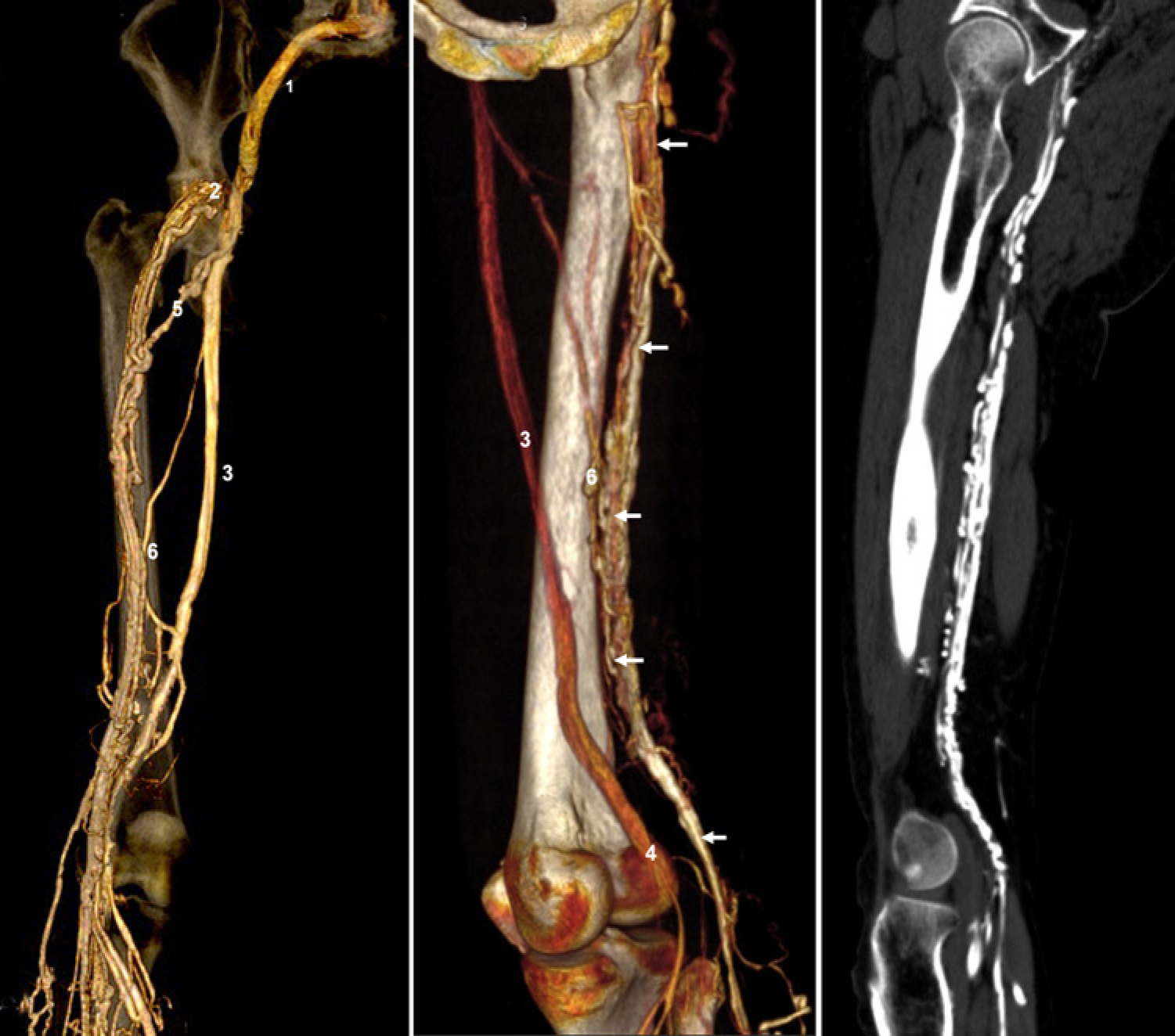

The superior gluteal leak point can also be responsible for a varix of the buttock extending to the posterior aspect of the thigh (Figure 20).
Case report of a varicose network of the buttock fed by the superior gluteal vein. 1 = superior glutheal vein; 2 = perineal network connected to the P point; 3 = Giacomini vein; 4 = normal great saphenous vein (GSV); 5 = refluxing GSV below the connection of the varix; 6 = communication vein of the calf feeding the small saphenous vein (SSV); 7 = SSV refluxing in the lower segment
CTV can also evaluate the reflux routes and anatomical connections of the pelvic venous networks. Another common cause of reflux is an incompetent left ovarian vein. This could be due to compression of the left renal vein between the aorta and the superior mesenteric artery or May Thurner syndrome. 24 But this is not easily investigated by CTV, and it is often necessary to perform a selective angiography for a full depiction of the pelvic venous network.
Nutcracker syndrome: Nutcracker syndrome compression of the left common iliac vein between the aorta and the right iliac artery is another possible cause of left ovarian vein reflux. 25 Although CTV could be useful, a direct selective angiography is more reliable and enables measurement of the pressure gradient between the vena cava and renal vein.
Investigation of congenital venous malformations (associated with colour duplex)
CTV can investigate congenital venous malformations, particularly the persistent marginal vein (Figures 21 and 22) with or without Klippel Trenaunay syndrome.
26
In those cases, it is important to check for possible abnormalities of the deep system, and the origin of the marginal vein, usually a perforator at the thigh level connected to the deep femoral vein (type 3 of Volmar).
Case report and computed tomography venography of an 11-year-old child with a persistant marginal vein and Klippel-Trenaunay syndrome. 1 = persistant marginal vein; 2 = deep femoral vein; 3 = perforator of the postero lateral thigh feeding the marginal vein; 4 = associated venous malformation of the Trochanter area; 5 = anterior accessory of the great saphenous vein; 6 = varicose network of the lateral knee Case report and three-dimensional reconstruction of a persistant marginal vein in an adult. 1 = persistant marginal vein; 2 = perforator of the postero lateral thigh connected to the deep femoral vein; 3 = femoral vein; 4 = common femoral vein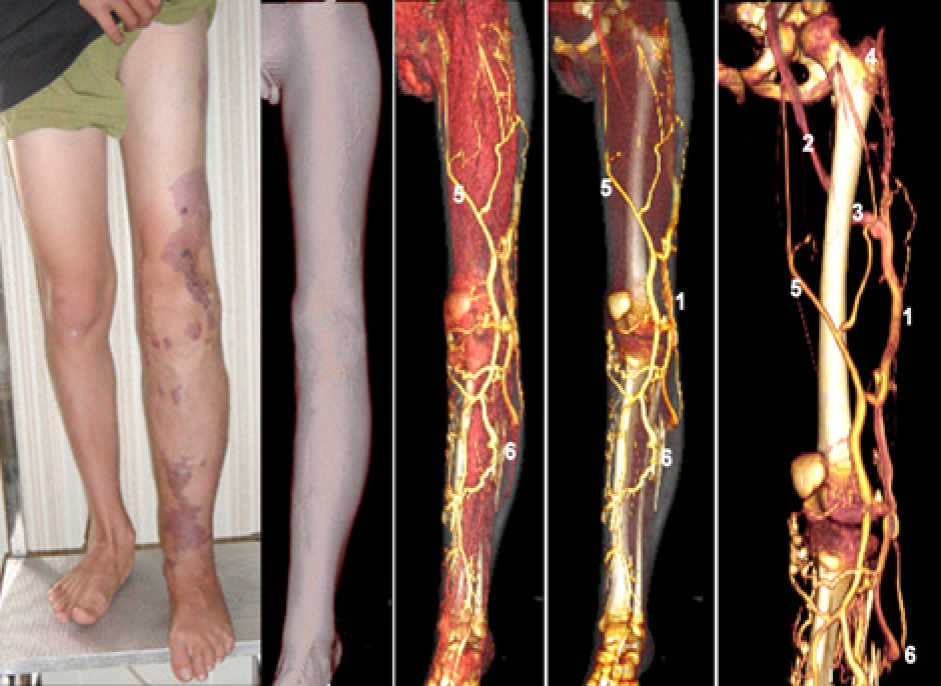
Rarely CTV may discover other congenital venous malformations such as IVC duplication or caval congenital atresia ….
Obstructive syndrome of Hunter's canal
A case report is shown (Figure 23).
27
Case report of a REVAS after small saphenous vein (SSV) surgery, due to compression of the femoral vein in the Hunter's canal. The big arrows indicate the level of the tourniquet. The small arrows are of the compression of the femoral vein in the Hunter's canal. The dilated venous arcades of the semimembranosus muscle are clearly visible, connected to the popliteal vein (P), by a lower arcade (a) and to the cavernoma of the residual SSV thumb (c). They are drained upwards by two higher arcades (a) into the deep femoral vein (d)
Compression of the popliteal vein … .
See ref. 28
Investigation of acute DVT
Diagnostic value of computed tomography venography for deep vein thrombosis of the lower limbs

VTE, venous thromboembolism; PPV, positive predictive value; NPV, negative predictive value; LR, likelihood ratio
According to Goodman et al. 29 with the PIOPED2 study, there is a 95.5% concordance between CTV and sonography for the diagnosis or exclusion of DVT; the kappa statistic is 0.809. The sensitivity and specificity of combined CTA and CTV are equivalent to those of combined CTA and sonography.
Coche et al. 30 demonstrated that a combined CTV with dual-slice scanning is an accurate method to diagnose DVT with a sensitivity of 93% and a specificity of 97% (κ = 0.88).
Garg et al. 31 demonstrated that 68 patients (97%) had a satisfactory or good quality CTV examination. Two CTV studies had false-positive findings due to flow artefacts. Both CTV and sonography had positive findings for DVT in five patients, and both had negative findings in 63 patients (100% sensitivity, 97% specificity, 100% negative predictive value and 71% positive predictive value). CTV was better and more efficacious than sonography in 25 patients (36%). CTV was equivalent to sonography in 26 patients (37%), and sonography was better than CTV in 19 patients (27%).
Compared with sonography, CTV in addition to CT pulmonary angiography is a relatively accurate method for evaluation of femoropopliteal venous thrombosis. Combined CT pulmonary angiography and CTV may be more effective than sonography or two separate examinations in selected patients.
Duwe et al. 32 found that CTV, compared with sonography, had a 93% accuracy in identifying DVT. However, the positive predictive value of only 67% for CTV suggests that sonography should be used to confirm the presence of isolated DVT before anticoagulation is initiated.
Combined with pulmonary angiography, CTV is reliable for DVT diagnosis, particularly at the ilio-femoral level. 27 Indirect CTV can detect DVT without pulmonary embolism with accuracy comparable to that of US and thus could have a significant effect on patient care. 20
Begeman et al. 33 found CTV to have a sensitivity of 100%, a specificity of 96.6% and a positive and negative predictive value of 91.7% and 100%, respectively. The median cumulative effective dose for CTV was 8.26 mSv with a gonadal dose of 3.87 mSv. Changing the CTV protocol to a collimation of 4 × 5 mm with a 25 mm table feed could reduce the dose by approximately 11% (P < 0.05) to 7.25 mSv and 3.35 mSv, respectively. They conclude that CTV is a safe and quick diagnostic tool for detecting DVT in patients with suspected pulmonary embolism (PE).
Peterson et al. 34 showed that the sensitivity and specificity of CTV was 71% and 93%, respectively. The positive predictive value, negative predictive value and accuracy rates of CTV were 53%, 97% and 90%, respectively. DVT localization was the same in eight of 10 cases in which the results of both DUS and CTV were positive. CTV costs and charges per study were greater than those of DUS by $46.88 and $602.00, respectively.
Lim 35 found CTV to be as accurate as sonography for the diagnosis of femoropopliteal DVT.
Please notice that all these authors use indirect CTV for the investigation of DVT. 36–40
According to our experience, this provides lower quality images than the direct technique with injection of the lower limb.
Yoshida et al. 41 also recommend this indirect technique, with injection of an arm vein, in cases of oedema.
Investigation of secondary CVD and PTS
In cases of postthrombotic occlusion of the left iliac vein, CTV can investigate the derivative routes of the iliac obstruction before treatment of varicose veins (Figures 24–26).
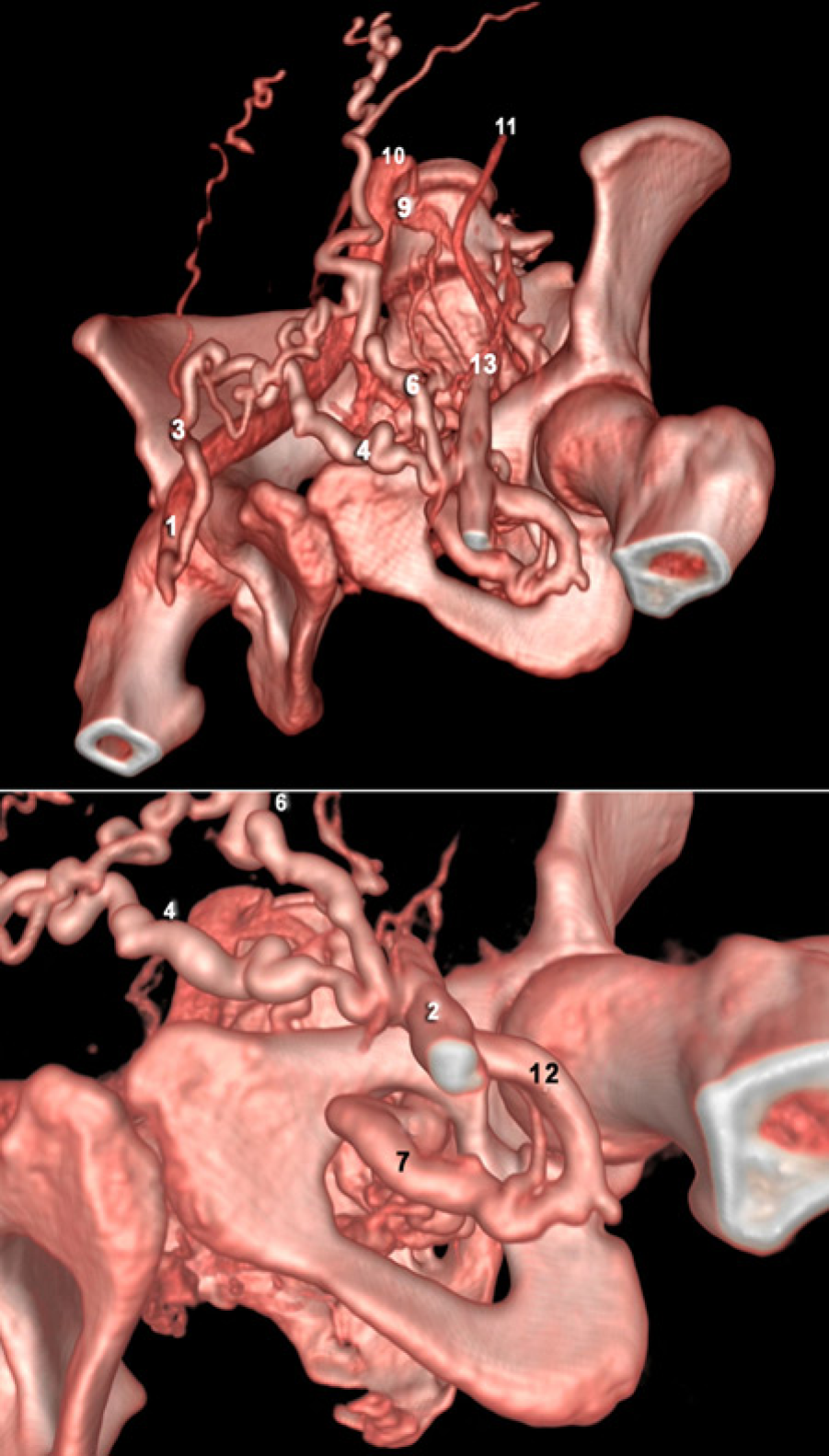
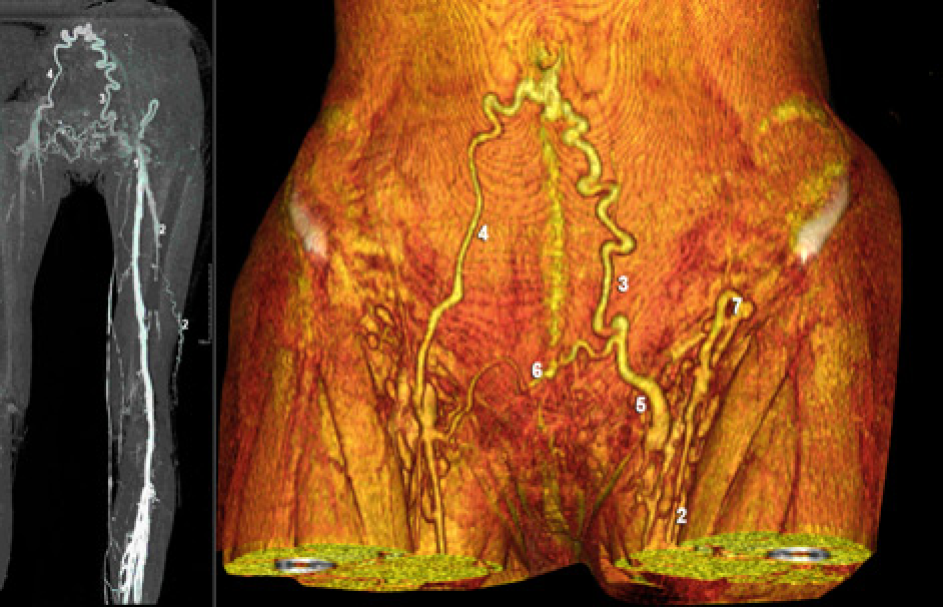
Three-dimensional reconstruction by volume rendering technique of a post-thrombotic syndrome by left iliac occlusion. Derivation routes are left pudendal (4), left (6) and right superficial epigastric (5) and obturator (7) veins. 1 = right femoral vein; 2 = left femoral vein; 3 = right pudendal vein;7 = obturator vein; 8 = right common iliac vein; 9 = compression of the termination of the left common iliac vein (May–Thurner syndrome); 10 = inferior vena cava; 11 = left ovarian vein CTV, three-dimensional reconstruction by volume rendering technique: inferior view of the same case. 12 = posterior circumflex vein, tributary of the great saphenous vein 13 = thumb of the occluded left iliac vein Three-dimensional reconstruction by volume rendering technique of a post-thrombotic syndrome due to left iliac occlusion. Derivation routes of the left femoral vein (1) are left pudendal (5), left (3) and right superficial epigastric (4). Please notice the varix of the anterior accessory of the great saphenous vein (2) with a dilation of the inguino-abdominal tributary (7)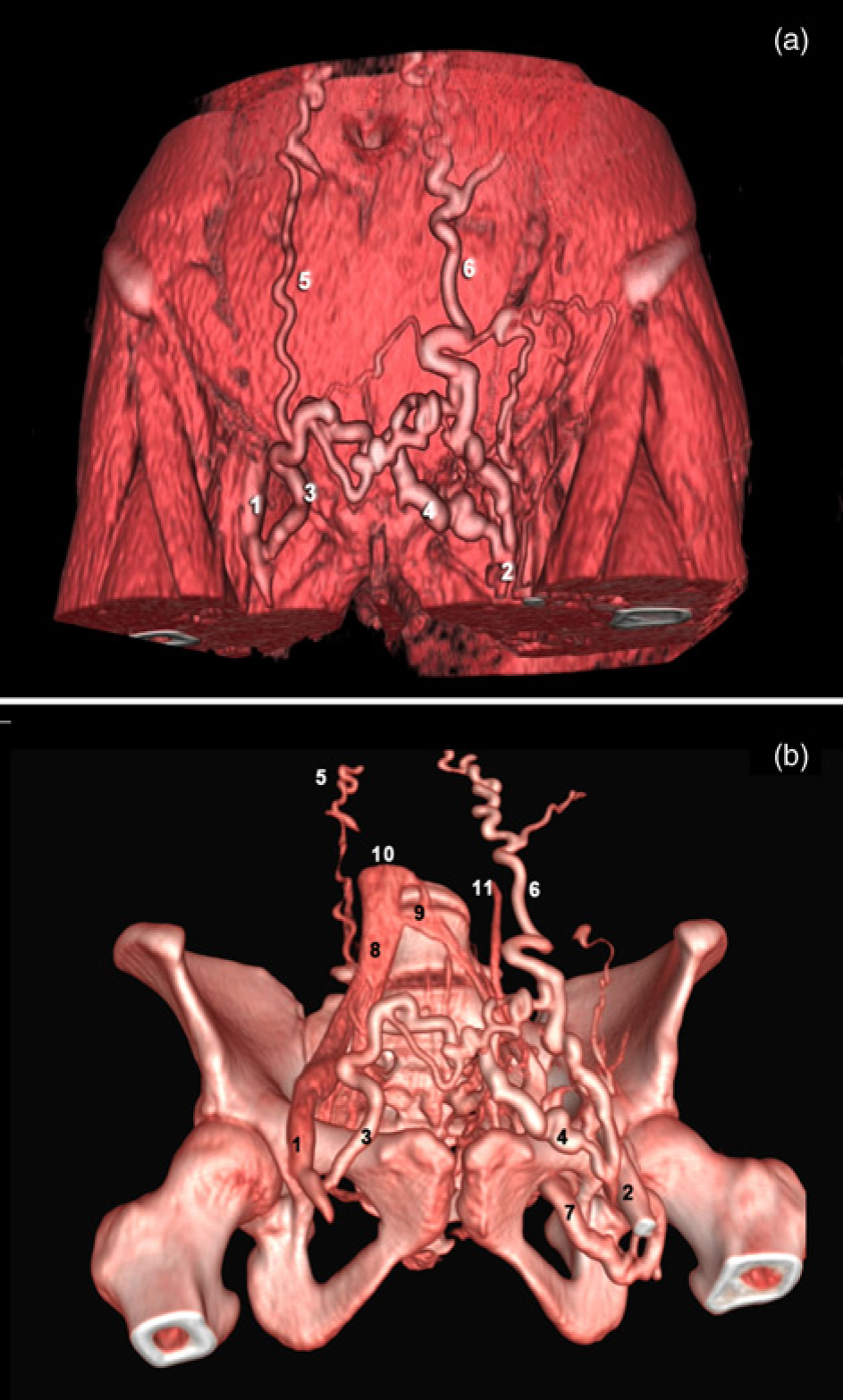
In some cases, an ilio-femoral occlusion could be related to a femoral catheter used after birth (Figure 27).
Case report and three-dimensional reconstruction by volume rendering technique of an occlusion of the femoral vein due to catheterization after birth (shown between the arrows). Derivation routes of the left femoral vein are obturator vein (3) left pudendal (5), bladder plexus (4). The great saphenous vein (GSV) is marked as 1 and the anterior accessory of the GSV as 2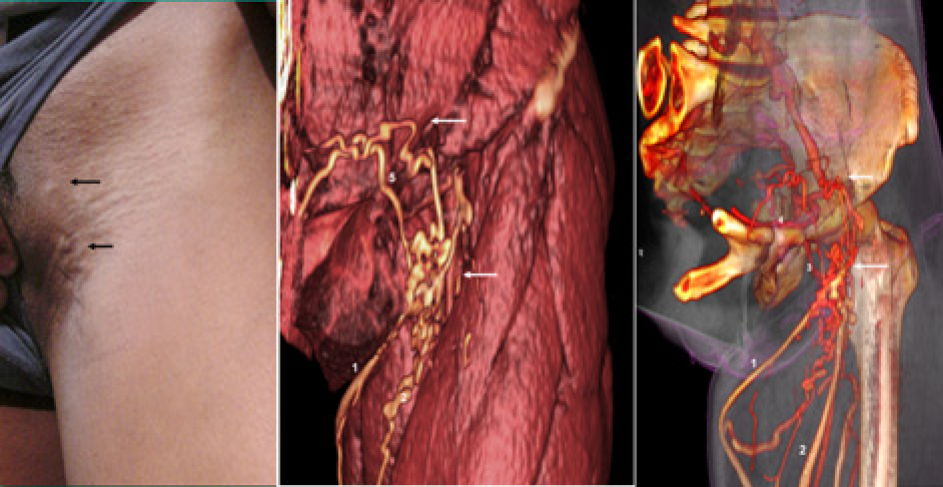
In summary, for investigation of CVD patients in the future, we think the main interest of CTV will be for a systematic and global investigation of the deep system, as recently suggested by Gaweesh et al. The discovery of underlying deep venous abnormalities in patients with chronic venous disease could be very common, 42–44 and the role of a proximal obstructive syndrome is often underestimated. 45–47
Congenital malformations of the vena cava or iliac veins could be discovered by CTV in DVT patients with no obvious cause. 48,49
Discussion validation, limits, pitfalls and drawbacks of CTV
Validation by comparison to DUS
For the investigation of CVD, the validation of this technique has been evaluated by comparison 26,28–31,39 to duplex sonography by Lee et al. 50 They showed among 100 consecutive CVD patients that the visualization of varicose veins was excellent in 76% of patients, fair in 21% and poor in 3%. However, no reproducibility study was performed.
The entire length of the GSV was visualized with CT venography in 99.5% of 200 GSVs.
The quality of 3D volume-rendered images was better when a thick subcutaneous layer, no skin changes and no subcutaneous oedema were present. The size of the GSV determined at CTV and DUS correlated well, the linear regression coefficient being 0.72.
At CTV, the mean diameter of GSVs exhibiting insufficiency on DUS was 7.0 mm, and the mean diameter of GSV's exhibiting competence was 4.9 mm (P < 0.001). Prediction of GSV insufficiency with CT venography had a sensitivity of 98.2% and a specificity of 83.3%.
Limits
Technical problems: Venous puncture was rarely impossible (3–4% of the limbs). Even in such cases, CTV without injection is possible, providing detailed anatomical information on the reconstructed 3D model, but restricted to the superficial network.
The main limit is that CTV provides very little haemodynamic data, mainly because it can only be performed with subjects in the supine position. This means that DUS examination (in the standing position) is mandatory in addition to CTV for the investigation of the superficial network as well as the deep system. This is particularly true for the patients with DVT.
Only Duplex provides a complete map of the superficial venous network and perforators with anatomical and haemodynamic data. In addition, a preoperative skin marking is mandatory, 3 to be used as a road map by the surgeon during surgery, together with the anatomical data provided by CTV.
Pitfalls
The main problem of CTV is the possible lack of injection of some veins, to be differentiated from a venous thrombosis. It may be due to competent valves, venous congenital agenesis or hypoplasia, or inappropriate compression points, usually the calf, by the table. 51
An exclusion area is also possible in cases of huge or high-located varicose veins.
If the territory is not filled by the foot injection, good visualization can be obtained by making a direct puncture of the varix. This is the case for pelvic varix visualization. A direct puncture of a thigh or perineal vein is preferred (but not the easiest) in order to get a fine injection of these complex networks.
Frequently, the reason for this lack of injection of a territory is an improper bolus timing of contrast material; usually a too short injection time whereby the contrast material did not have sufficient time to reach the anatomy of interest. In order to avoid this problem, one can use a tourniquet and/or a Valsalva manoeuvre. This is particularly true for popliteal fossa investigation: here the tourniquet of the root of the limb increases the quality of contrast and avoids an examination failure.
Pitfalls could also be related to beam-hardening artefacts: streak or beam-hardening artefacts resulting in hypodense or hyperdense streaks in the neighbouring structures are commonly encountered and may be generated by orthopaedic material, bone or vascular calcifications.
Anyway, in case of difficulty, we have to keep in mind that 3D reconstructions are not fully reliable. These smart postprocessing routines could in some instances create images that do not actually exist, and do not enable reliable measurement of the distances.
Hence, to avoid a misunderstanding or a false diagnosis with the use of the 3D images, do not hesitate:
To go back to the original slices; To use multiplanar reconstruction making a quantification possible; And to complement with other investigations (DUS).
Drawbacks
Radiation exposition to X-rays is the main criticism of CTV.
Another problem is the venous puncture.
A pure venogram could be obtained by other ‘radiation-free’ and less invasive techniques, but they provide a lower quality of images: magnetic resonance venography without gadolinium injection using protocols that incorporate 2D time of flight acquisition. Fraser et al. 10 proposed a new MR venography technique called venous enhanced subtracted peak arterial with gadolinium injection, using spatial subtraction that eliminates the need to cannulate a foot vein. It has also been proposed to reduce radiation. 11–13
But a good solution is to use low-dose X-ray irradiation, as can be done with the GE General Electric Company (Chalfont St. Giles – UK) Healthcare CT 750 HD or better, and with the sterEOS system ultra low dose technique of G Charpak. 52
Conclusion
The aim of spiral CTV is to provide a precise 3D anatomical depiction of the venous network. A multislice and multidetector spiral CT acquisition of the lower limb with contrast injection now produces 600–1000 anatomical slices. Dedicated volume-rendering software computes 3D images of the venous system as well as interactive movies and virtual travels.
For varicose veins, CTV is a powerful new tool to investigate patients, always associated with colour-coded DUS, which provides haemodynamical data. It is particularly indicated in the case of a recurrence of the popliteal fossa or for complex networks. It truly provides a 3D roadmap for surgical planning.
This is most important in special cases, such as the presence of a pelvic origin of varicose veins and the varix of the sheet of the sciatic nerve.
For congenital vascular malformations, CTV is mandatory due to the complex anatomy and necessity to have a precise depiction of the whole venous system. It is often associated with magnetic resonance imaging to detect intramuscular lesions.
For the diagnosis of acute DVT of the lower limbs, CTV is specific, but has a lower sensitivity and positive predictive value compared with DUS.
Finally, besides the patient's assessment, the CTV make us enter in the virtual reality world. By that way, it is a tool of the highest interest for a better understanding of venous disease, and to teach and learn the venous anatomy, and for research in the field of vascular diseases.