
Abstract
Introduction:
Lymphatic complication (LC) after varicose veins (Ws) surgery is an annoying event with a variable frequency in the literature.
Method:
Retrospective study reviewing all surgeries carried out for VVs from January 2000 to October 2010. Postoperative LC we reported: lymphatic fistula, lymphocele including the minor ones and lymphoedema.
Results
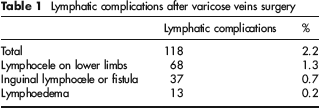
During the period studied, 5407 surgical procedures for VVs were performed in 3407 patients (74.7% women) with a mean age of 53.4 years. A postoperative LC occurred in 118 cases (2.2%): lymphocele on limb in 1.3%, inguinal LC (fistula or lymphocele) in 0.7% and a lymphoedema in 0.2%. The population with a LC was older (59.6 vs. 53.3 years, P < 0.05), had a higher frequency of C4–C6 (22.0% vs. 6.5%, P < 0.05), a higher incidence of obesity (31.4% vs. 5.4%, P < 0.05) and was more often treated by a redo surgery or a crossectomy stripping (48.3% vs. 13.4% and 38.1% vs. 21.8%, respectively, P < 0.05). We have observed a dramatic decrease in incidence of LC after January 2004 (1.3% vs. 5.3%, P < 0.05) corresponding to a new surgical practice for the treatment of VVs: stripping, crossectomy and redo surgery at the groin were less frequent (74.6% vs. 7.7%, 74.6% vs. 0.2% and 11.3% vs. 0.1%, respectively, P < 0.05), while isolated phlebectomy was more often performed during this period (78.4% vs. 8.4%, P < 0.05).
Conclusion:
LC after VVs surgery is not rare but frequently limited to lymphocele on limbs. Older age, more advanced clinical stage and obesity were associated with a higher frequency of LC. A mini-invasive and selective surgery has significantly reduced the occurrence of LC.
Keywords
Background
The lymphatic complications (LC) such as lymphocele, lymphatic fistula or lymphoedema are some of the most frequent complications after surgery for varicose veins (VVs). 1 However, its frequency is variable in the literature and the risk of long-lasting complication is rather low (<0.5%) after primary VVs surgery. 1 Some risk factors for LC are clearly identified: lymphatic insufficiency, 1 redo surgery for VVs especially at the groin 2 4 and special locations such as the dorsal part of the foot or the front of the shin.1,5 Other risk factors including obesity have not been reported so far.
To evaluate the presence and the frequency of risk factors for LC after surgery of VVs and therefore to try to avoid it, we reviewed our experience over 10 years.
Method
We conducted a retrospective study on all surgeries carried out for VVs in our centre from January 2000 to October 2010. We reviewed the traditional preoperative data (demographics, signs, symptoms, body mass index [BMI]), the preoperative venous haemodynamics (presence and location of venous reflux), the surgical technique performed and the postoperative LC reported (lymphatic fistula, lymphocele including the minor ones and lymphoedema).
Results
During the period studied 5407 surgical procedures for VVs were performed on 5050 lower limbs (LLs) in 3407 patients (74.7% women). The mean age of the population was 53.4 years. The preoperative frequency of CEAP (clinical, aetiological, anatomical and pathological elements) class C classification was the following: 0% C0–C1, 83.4% C2, 7.9% C3 and 7.3% C4–C6. Symptoms such as pain, heaviness, a swelling sensation, pruritus, night cramps, restlessness, tingling and heat were present in 63.8% of the cases. The average BMI was 24.02. All patients had a preoperative ultrasound duplex assessment which showed a reflux on the great saphenous vein in 56.7%, on the short saphenous vein in 6.4% and a competent saphenous vein (SV) in 30.1% and it was a recurrent reflux after stripping in 13.9%. The surgical procedure carried out was a stripping of the SV in 22% of the cases, an isolated phlebectomy in 63.8% and a redo surgery after stripping in 14.2%.
Lymphatic complications after varicose veins surgery
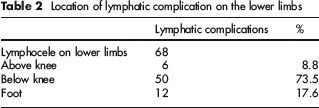
Location of lymphatic complication on the lower limbs
Comparison of population with and without a lymphatic complication after varicose veins surgery
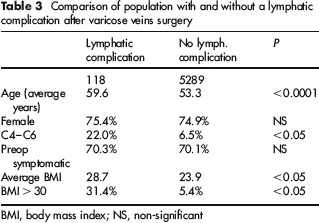
BMI, body mass index; NS, non-significant
Comparison of the frequency of different types of lymphatic complication in obese (BMI > 30) and non-obese patients (BMI<30)

BMI, body mass index
Incidence of postoperative lymphatic complication depending on the type of surgical procedure

Comparison of postoperative lymphatic complications and procedures carried out before and after 2004 for the treatment of varicose veins

At last, a preoperative skin marking guided by ultrasounds was performed in 82.4% after January 2004 and only in 20.9% before.
Discussion
Our study showed that an LC after surgery for Ws was not rare, occurring in 2.2% after the surgical procedures. Nevertheless, in the wide majority of the cases the LC was minor, represented by a lymphocele located at the LLs, while more serious complications such as lymphatic fistula or lymphoedema were infrequent (0.7% and 0.2%, respectively), in accordance with the literature. 1 We observed that the redo surgery for recurrent VVs had a much higher frequency of LC (7.5% vs. 2.2%) as it has been reported by other authors. 2 4 In accordance with the literature, we observed that a lymphatic insufficiency was a risk factor for an LC since five out of 13 patients with a postoperative lymphoedema have had a preoperative primary lymphoedema. We also found in this study other risk factors increasing the incidence of postoperative LC, such as older age and presence of chronic venous disease with skin damage (C4–C6). Above all, obesity was found in this study to be a strong risk factor for LC: the presence of a BMI > 30 increased the frequency of lymphocele on LLs by 1.6, the frequency of lymphatic inguinal complication by 7.5 and the frequency of lymphoedema by 14.7.
We observed a significant difference for the rate of LC according to the period studied: 5.3% before January 2004 while it dramatically decreased to 1.3% after January 2004. Actually we accomplished a major evolution in our surgical approach after 2004 towards a less invasive technique, especially for the treatment of Ws recurrence with the near-abandonment of redo surgery at the groin (0.1% vs. 11.4%), but also for the treatment of primary VVs. Indeed after January 2004, the traditional high ligation and stripping was quasi-replaced by isolated phlebectomy (ASVAL) and mini-invasive saphenous ablation. The interest of avoiding a surgery at the groin is cited,6,7 as well as the benefit of the preservation of the saphenous junction during stripping8,9 for the reduction of postoperative complications after surgery, with good results in terms of signs and symptoms. The endovenous treatments by laser and radiofrequency, as well as foam sclerotherapy, are in the same trend of mini-invasiveness for the treatment of VVs, leading to a reduction of complications, including LC. 10 13
This evolution of our surgical technique was accompanied with a more frequent preoperative skin marking guided by ultrasounds (82.4% vs. 20.9%), and therefore a more precise surgical gesture. The importance of a precise preoperative duplex ultrasounds assessment for the safety of the procedure and quality of the result is clearly reported in the literature.5,14,15
Therefore, as older age, presence of skin damage and obesity are identified as risks for an LC after surgery for VVs, it is mandatory to use less aggressive approaches by mini-invasive surgery, thermoablation or foam sclerotherapy, guided by pre- and/or perioperative guidance by ultrasound especially for these patients.
Conclusion
LC after VVs surgery are not rare but are frequently limited to lymphocele on limbs. Our study confirmed that redo surgery, especially at the groin, is a risk factor for LC especially at the groin. Older age, chronic venous disease with skin changes and obesity were also found to be risk factors for LC after VVs surgery. In our experience, a mini-invasive surgical approach avoiding redo surgery at the groin or high ligation, and guided by preoperative skin marking, has reduced the frequency of postoperative LC.