
Abstract
Objectives:
To review the current literature on the outcomes of pharmacomechanical thrombectomy (PMT) for early thrombus removal in patients with venous thromboembolism (VTE).
Methods:
We searched the MEDLINE database and performed a manual search of the references of selected articles to select reports reporting the outcomes of PMT alone and PMT compared to catheter-direct thrombolysis (CDT). Outcomes of interest included clot lysis rate, incidence of pulmonary embolism, major bleeding, recurrent deep vein thrombosis, number of venograms needed and amount of lytic utilized.
Results
We found nine articles that reported outcomes of PMT. Three devices were utilized for PMT, the Angiojet, Trellis and Helix. Different thrombolytics were used to facilitate thrombus removal including urokinase, reteplase, tecneteplase, and tissue plasminogen activator (t-PA). Complete and partial thrombus removal were achieved in up to 84% and 64% and 81% and 59% of the limbs treated with PMT and CDT alone, respectively. Data on PE and bleeding risk after PMT compared to CDT are scarce. The duration of the thrombolysis process, amount of lytics and number of venograms were substantially reduced in the patients who had PMT compared to those who underwent CDT alone. Two articles evaluated the obstacles that limit the indication of PMT in patients with VTE.
Conclusion:
VTE is a prevalent burden in Western societies. The rationale of early thrombus is to reduce valvular damage and improve venous patency in order to reduce the risk of PTS. PMT is a feasible, safe and faster alternative to expedite the thrombolysis process in patients with VTE.
Introduction
Venous thromboembolism (VTE) causes an enormous negative impact in modern societies. Distinct forms of VTE presentation in the acute phase include deep vein thrombosis (DVT) and pulmonary embolism (PE). 1 Natural history after an episode of VTE includes thrombus propagation, recanalization and/or recurrence with post-thrombotic syndrome (PTS) following DVT occurring in up to 30–40% of patients and resulting in a significant socioeconomic burden to society. 2
Complete resolution of clot following venous thrombosis with anticoagulation is seen in only one-third of patients. 3 Affected venous segments may develop destroyed valve apparatus and result in reflux, obstruction or a combination of both. 4 The highest risk of developing PTS has been demonstrated in limbs that have a combination of reflux and obstruction.4,5 The location and extent of venous thrombosis also play a significant role. An extensive proximal DVT such as iliocaval or iliofemoral occlusions has unquestionably worse prognosis when compared with patients with infrainguinal or calf vein thrombosis6,7 and may be related to the fact that recanalization rate differs according to the location of thrombosis. More proximal segments with a larger luminal diameter and thus higher thrombus load often have insufficient thrombus resolution with anticoagulation alone rendering the affected sites more prone to developing residual obstruction. 5 In addition, it increases the rate of recurrent proximal DVT that poses a very important risk of PE and not least an important risk of developing PTS. 8
Early thrombus removal especially in high-risk patients with iliofemoral DVT should be considered to reduce thrombus load, re-establish venous flow, minimize endothelium and valve injury, the ultimate goal being lower rates of PTS and improvement in patients’ quality of life.
Endovenous interventions for DVT
An understanding of the different treatment modalities of DVT and their long-term impact on outcomes is critical. Anticoagulation remains the most common treatment either by using low-molecular-weight heparin or unfractionated heparin and bridging over to Coumadin. This prevents propagation of thrombus and embolization but has little impact on thrombus resolution. In a review of 13 studies a total or partial resolution of venous thrombosis was found in only 4% and 14% of patients who were treated with anticoagulation. 9
Both surgical and percutaneous interventions have been used to treat DVT and allow early thrombus removal. In the past, open venous thrombectomy was performed in extreme cases of extensive DVT with impending venous gangrene aiming for limb salvage.10,11 This was associated with marginal results, re-thrombosis and significant postoperative complications. Contemporary indication for surgical thrombectomy is limited to patients with extensive proximal (iliofemoral) DVT and contraindication for thrombolytic agents. 12
Currently, the modality of choice to treat extensive proximal DVT has been changing with the advent of catheter-directed thrombolysis (CDT) and pharmacomechanical thrombectomy (PMT). Promising results have been achieved using CDT or PMT techniques. 13 The purpose of CDT was to achieve early thrombus removal using a minimally invasive, percutaneous technique with local delivery of thrombolytics and, therefore, decrease the surgical morbidity. However, the major drawback of the technique is the prolonged treatment time, large thrombolytic doses and prolonged intensive care unit and hospital stay.
PMT utilizing devices that macerate the thrombus coupled with simultaneous infusion of thrombolytic medications. The mechanical maceration of clot increases the surface area to allow thrombolytics to have a more effective and faster lysis. Single-session therapy can be achieved with PMT in patients with not as extensive thrombus and very early thrombosis. The limitation of currently available devices is the requirement of adjunctive CDT in patients with extensive thrombus load and/or sub-acute clot in a significant number of patients.
Patient selection, contraindications and complications
Eligibility criteria for PMT follow the same as those recommended for CDT. Routine candidates for PMT include patients with an extensive acute proximal (ileofemoral) DVT with less than 14 days from onset of symptoms or acute findings on duplex ultrasound, life-expectancy >1 year with good functional status and low risk of bleeding are candidates.12,14 Variations of the established indications above are treatment of femoropopliteal DVT and thrombus >14 days. In addition, patients with relative contraindications for CDT due to higher risk of bleeding may be candidates for PMT because of lower doses of thrombolytics. Some devices even allow segmental therapy by utilizing proximal and distal balloons to isolate the segment to be treated and thus minimize systemic delivery of drugs. Potential complications of the procedure include minor bleeding at the venous puncture site, haemolysis, major bleeding requiring blood transfusion (i.e. brain, retroperitoneum, muscles and gastrointestinal/genitourinary tract), re-thrombosis and PE.
PMT devices available
Endovenous therapy for DVT has evolved over the past two decades. Mechanical devices have been developed that utilize suction and vacuum, ultrasound waves or rotational impact to macerate the thrombus. Delivery of thrombolytics through these devices is also possible. The mechanical maceration of thrombus not only increases the surface area but also penetrates the thrombolytics into the thrombus. Thus, theoretically the interval spent to remove the thrombus load is decreased with smaller amount of thrombolytics delivered.
There are two PMT devices that are US Food and Drug Administration-approved for treatment of DVT, the Angiojet® Thrombectomy system (Medrad/Possis Inc., Minneapolis, MN, USA) and the Trellis™-8 Peripheral Infusion System (Covidien, Mansfield, MA, USA). 15 It is also pertinent to cite another device that can deliver low-frequency ultrasound waves to increase penetration of thrombolytics into the thrombus, the Ekos Endowave® system (Ekos Medical, Bothell, WA, USA).
The Angiojet system applies the Bernoulli–Venturi principle, which uses alternating fast water jets with low fluid pressure creating a vacuum zone at the tip of the catheter. Maceration of the thrombus occurs and the small particles are aspirated through the efferent port. Thrombolytic infusion can be added in a ‘pulse-spray’ fashion to impregnate the thrombus.
The Trellis™-8 Peripheral Infusion System utilizes a dispersion spiral wire at high spinning motion to macerate the thrombus. The treated venous segment can be impregnated with thrombolytics and isolated between a proximal and distal end balloon. Following treatment, an aspiration port allows aspiration of residual thrombolytics and thrombus. Further details on the use of the above devices are described below.
Preparing for the procedure
In the angiography or dedicated OR suite, the patient is prepped in a prone or supine position, depending on the access site. The most commonly used access site is the ipsilateral popliteal vein with the patient in the prone position. Ultrasound-guided access is then obtained using a micropuncture kit (3-Fr or 4-Fr kit). After checking for venous flow with manual contrast injection, the micropuncture catheter is exchanged over a wire to a 5-Fr sheath. Other access options include the posterior tibial vein in cases of extensive DVT involving the popliteal vein, ipsilateral femoral vein access when an isolated iliac vein thrombosis is found, contralateral femoral vein or jugular vein.
A glide wire/glide catheter system is almost always successful to get wire access in the inferior vena cava (IVC). How easy it is to cross the thrombosed segment may be indicative of how acute the thrombus is and may predict the success of lysis. Gentle venogram is then obtained to evaluate the extent of thrombus.
IVC filter placement
The use of IVC filters during PMT is controversial. The proponents of the IVC filter justify the use if a massive proximal DVT in a patient with limited cardiopulmonary reserve is encountered; thrombus extension into the IVC or extensive PE is present prior to PMT. However, data on PE secondary to PMT are scarce. The incidence of PE after PMT is reported from 0% to 17%. 16 20 Frequently, subclinical PE occurs in patients who did not have an IVC filter placed prior to the procedure. 16
Trellis™-8 device
On gaining access, a 5-Fr sheath is exchanged for an 8-Fr sheath to accommodate the Trellis catheter. Once the catheter is advanced and parked 1–2 cm above the segment of interest, starting always in the most proximal (in relation to the heart) venous thombosed area, the distal (in relation to the catheter) balloon is inflated. Noteworthy, the longest treatment length zone that can be treated at once is 30 cm. Subsequently, the guidewire is exchanged by the sinusoidal wire and the proximal (in relation to the catheter) balloon is inflated. A combination of recombinant tissue plasminogen activator (r-tPA) mixed with heparinized saline is then infused according to each operator's preference.
After 15–20 minutes of treatment, the proximal balloon is deflated and fragments of thrombus along with residual r-tPA are aspirated through the side port while flushing the infusion port. Subsequently, the distal balloon is deflated and the catheter re-positioned to treat more distal venous segments. After treating the entire thrombosed venous segment, venogram is performed to gauge the success of the procedure. If residual thrombus is demonstrated, a couple of options can be chosen: (1) repeating an additional course of PMT, (2) angioplasty and/or stenting if iliac vein stenosis and/or residual thrombus is present, or (3) placement of infusion catheter in areas of residual thrombus for CDT An illustrative case of proximal DVT treated with the Trellis device is shown in Figures 1-3.
One of the advantages of the Trellis system over CDT is its potential safety in patients with relative contraindication to thrombolytic agents due to proximal and distal balloon protection. Theoretically, a decent amount of lytic medication can be retrieved with thrombus before it reaches the systemic circulation. In addition, aspiration of thrombus particles is accomplished while the distal balloon is inflated, potentially reducing distal embolic events.
Angiojet® Rheolytic System
Similar to the Trellis, venous access is obtained. An angled glide catheter is advanced and parked into the IVC. The device is advanced over the wire and turned on starting from proximal to distal in the venous segment. High pressure of saline jets generated by a drive unit fragment the thrombus and are aspirated via the effluent port. To treat the entire thrombosed segment, the catheter is withdrawn in 1-cm segments and 2–3 passes may be necessary. ‘Power-pulse’ spray is also possible which allows thrombus impregnation with thrombolytics for 15–20 minutes. The aspiration port is subsequently opened and the device is used again to aspirate residual thrombus and thromoblytics. A completion venogram is obtained to decide between completion of the procedure, re-treatment or continuous CDT drip. If an underlying iliac vein stenosis is uncovered, it should be treated with PTA and stenting (Figure 2).
Left leg venogram with iliofemoral thrombosis, (a) Arrows demonstrate thrombus in the common femoral and external iliac vein, (b) Venogram with catheter in the external iliac vein revealing acute thrombus and chronic webs (arrow) pharmacomechanical thrombolysis using the Trellis device. Arrows demonstrate the proximal (black) and distal (white) occlusion balloons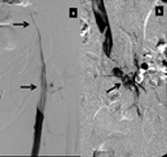

The system drawback is the amount of fluid necessary to be infused in order to dissolve thrombus. In patients with renal or cardiac failure a larger amount of fluids may render the procedure impeditive due to fluid restriction. In addition, provoked haemolysis with increased bilirubin release in patients with liver failure may also be another potential contraindication.
Venogram following pharmacomechanical thrombolysis. Resolution of acute thrombus with residual webs and common iliac vein compression (arrow)
Venous stenting and angioplasty
Limited data on venous angioplasty and stenting post-thrombolysis exist. Patients with significant residual stenosis or thrombus found in venography or intravascular ultrasound are potential candidates for angioplasty and stenting.
21
Other indications are residual stenosis with the presence of collaterals, intraluminal filling defects or poor venous outflow. We advocate the use of self-expanding over balloon-expandable stents for the iliac veins, covering all venous segments with residual disease in order to achieve good inflow and good outflow (Figure 4).
Venogram following iliac vein stenting (18 mm × 90 mm Wallstent). Stent extends from inferior vena cava to the external iliac vein (arrows)
Clinical outcomes
Published studies on PMT

r-tPA, recombinant tissue plasminogen activator; PMT, pharmacomechanical thrombectomy
Kasijaran et al. 15 analysing their initial experience using the Angiojet on 17 patients demonstrated the overall (>50%) thrombus removal in 59% of the patients. Another centre also utilizing the Angiojet device in 23 limbs reported complete and partial thrombus (50–99%) resolution in 65% and 35%, respectively. 19 A comparison between the Angiojet versus CDT only using urokinase showed reduced treatment duration and lower costs with the Angiojet® pulse system. 18 Lin et al. 24 in 93 patients treated for symptomatic proximal DVT showed lower mean intensive care unit stay and overall length of hospital stay, and lower total hospital cost with Angiojet® when compared with CDT only.
Comparative procedure-related data on CDT versus PMT
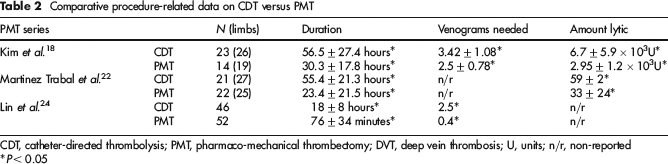
CDT, catheter-directed thrombolysis; PMT, pharmacomechanical thrombectomy; DVT, deep vein thrombosis; U, units; n/r, non-reported
*P < 0.05
Outcomes of PMT alone or CDT versus PMT
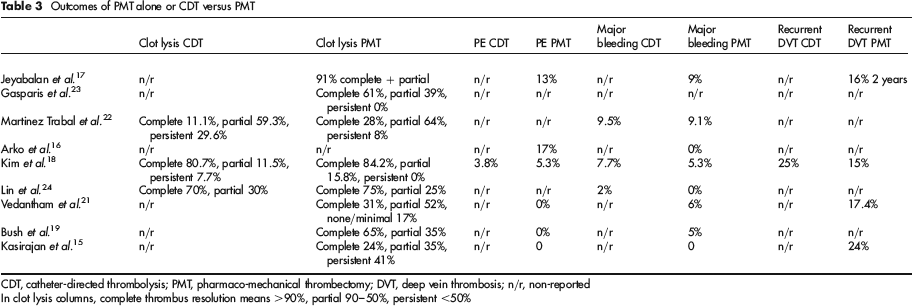
CDT, catheter-directed thrombolysis; PMT, pharmacomechanical thrombectomy; DVT, deep vein thrombosis; n/r, non-reported
In clot lysis columns, complete thrombus resolution means >90%, partial 90–50%, persistent <50%
Limitations
There are several limitations in the available literature that explain the weak recommendation grade reported. 12 First, the vast majority of data on the topic are based on the low evidence-based level of PMT series due to their retrospective designs. Second, according to the same guidelines published the inclusion and exclusion criteria for thrombolysis remain quite extensive. Thus, recruitment is also a limiting factor to enrol patients.
Two articles outlined some of the pertinent obstacles limiting indication of thrombolysis and PMT. Klein et al. 14 found only 12 (2%) patients from a pool of 576 patients with DVT over a six-month period in our institution. The most common cause for exclusion was short life-expectancy secondary to active malignancy. 14 In another series of 394 patients with DVT, 95 had iliac involvement and at least one contraindication to thrombolytic therapy was present in up to 75%. 27 The most common exclusion impediments for an intervention were prolonged symptom duration, renal impairment, advanced age and active malignancy.
The ongoing ATTRACT trial is a randomized trial that was designed to enrol 692 candidates to either PMT with anticoagulation versus anticoagulation alone. 28 All patients with symptomatic proximal DVT will be monitored to assess the incidence of PTS at two-year follow-up. 28 In addition, quality of life, safety and other cost analyses are expected to be addressed.
Conclusions
VTE is a cause of substantial morbidity and mortality generating a major socioeconomic burden in Western societies. Studies have shown that early thrombus may reduce valvular damage and improve venous patency. Preserving venous haemodynamics may alter the natural history of DVT and prevent or reduce PTS. PMT expedites the thrombolysis process with lower use of thrombolytic use and thus can achieve similar results to CDT with less risk and cost.
Footnotes
Available PMT systems for treatment of DVT
PMT, pharmacomechanical thrombectomy; DVT, deep vein thrombosis
Trellis™-8 Peripheral Infusion System
Angiojet® Rheolytic System
Length (cm)
Treatment Zone (cm)
Catheter
Length (cm)
Sheath (Fr)
Guidewire
Vessel diameter (mm)
80
10
XMI RX+®
135
4
0.014′
2–5
80
15
Spiroflex™
135
4
0.014′
2–5
80
30
XVG®
140
5
0.014′
3–8
120
15
Xpeedior®
120
6
0.035′
4–12
120
30
DVX®
90
6
0.035′
4–12