
Abstract
Objective:
To describe the background for – and mechanism of – catheter-directed thrombolysis (CDT) for iliofemoral deep venous thrombosis (DVT) accessed via the popliteal vein. Focus is on safety and efficacy.
Method:
From the Copenhagen experience we have looked into the systematically registrated risk factors, peri- and postprocedure complications for patients consecutively treated from 1999 to 2006. The patients were treated in a clinical ward. The patients were followed yearly with ultrasonography for assessment of patency and valve function. Inclusion and exclusion criteria have been published earlier.
Results
A total of 89 patients with 91 extremities with iliofemoral DVT were included (70 women and 19 men, mean age 29 years [range 14–59]). Only 11% of the patients were without any risk factor for DVT. CDT was performed without mortality and pulmonary embolism. Major bleeding occurred in two patients and minor bleeding in 27 patients, mostly from the puncture site. Stenting was necessary in 54 limbs. Five stents revealed occlusion, three procedural (2 reopened) and two late. The median follow-up was 87 months (range 17–148). At six years, 86% had competent iliofemoral (and popliteal) vein segment.
Conclusion:
CDT of iliofemoral DVT is a safe procedure. The patients can stay in a clinical vascular ward. The long-term efficacy is still durable in producing competent veins as concluded in our earlier published results.
Background
Catheter-directed thrombolysis (CDT) can be used as immediate thrombus removal, especially in the treatment for acute iliofemoral deep venous thrombosis (DVT). The rationale for CDT is to avoid morbidity in a post-thrombotic syndrome (PTS) by increasing venous patency, preventing damage of the venous valves and reflux. However, no consensus exists in this area because of lack of convincing evidence from randomized controlled trials. Additionally, controversies exist regarding the increased risk of pulmonary embolism (PE) and bleeding complications connected to this treatment modality. However, in the latest evidence-based clinical guidelines from the American College of Chest Physicians from 2008 early intervention for DVT using CDT or pharmacomechanical thrombolysis was recommended at a level 2B and 2C, respectively. 1 Today, the use of CDT is restricted to only some centres.
Since CDT is a relatively new treatment, it has to be safe and effective. The previously used systemic thrombolysis was associated with an increased risk of bleeding complications and was not found to be as effective as intrathrombus catheter delivery in a randomized trial in the arterial system. 2 Earlier, venous thrombectomy under general anaesthesia did not show clearly improved outcome compared with conventional anticoagulation therapy. 3 The method was associated with complications and a relatively high risk of re-thrombosis since it was not combined with additional stenting of the iliac stenosis. However, newer studies have combined venous thrombectomy with perioperative stenting with promising results. 4
DVT damage
The development of PTS is believed to be a consequence of ambulatory venous hypertension caused by venous valve incompetence and persistent luminal obstruction. The venous valves and the vein wall are believed to be damaged by inflammatory mediators associated with the presence of the acute thrombus or during the healing process with thrombus remodelling. In this process, leukocytes are activated with adhesion and migration through the basement membrane. 5 The transmission of the high deep venous pressure to the venous end of subcutaneous capillaries results in increased endothelial permeability and impaired capillary flow. The escape of large molecules into the interstitial tissue may explain the presence of interstitial oedema, hyper pigmentation and ulcer formation. 6 Observations indicate that the most severe post-thrombotic morbidity is associated with the highest venous pressures seen in patients with both venous obstruction and venous valve incompetence. 7 These patients have a higher risk of skin damage. 8
In a large study, several parameters that predicted the worst post-thrombotic morbidity were severity of venous symptoms at one month, iliofemoral thrombosis, previous ipsilateral thrombosis, female gender, older age and high body mass index, and iliofemoral location has been found to predispose to PTS more frequently than infrainguinal DVT. 9 Iliofemoral DVT predisposes patients to higher recurrence rates compared with infrainguinal DVT 10 and development of recurrent ipsilateral thrombosis has in several studies been found to be strongly associated with the risk for PTS. 11
Action of thrombolysis
The delivery of the thrombolytic agent (streptokinase, urokinase or tissue plasminogen activator [t-PA]) directly into the venous clot (high intrathrombus drug concentration) accelerates thrombolysis by converting the fibrin-bound plasminogen into the active enzyme plasmin thereby dissolving the clot. In this way a systemic influence is assumed to be minimized, thereby reducing the risk of complications for the patient. Unfractionated heparin is added to the lytic fluid. Today t-PA is the mostly used drug, due to short half-life, given as a minimum of 1 mg per hour with heparin adjusted in order to keep the activated partial thromboplastin time (APTT) on a level of maximum 100 seconds. This chemical action can be monitored clinically but more accurate by daily biochemical surveillance. The patients reveal symptom relief as soon as the thrombus load is reduced. Contraindications to CDT have been described in a previous publication from 2010. 12
DVT age prior to CDT
Before the patient is treated with CDT, a thorough anamnesis has to be obtained. Questions about the exact duration of symptoms, the cause or predisposing factor, previous episodes of DVT, information about thrombophilia, etc. should be covered. A very important issue connected to this treatment modality is the duration of symptoms, as the best results are seen when treating acute thrombosis supported by results from a multicentre registry from 1999. 13 Acute DVT refers to venous thrombosis for which symptoms have been present for a maximum of 14 days or for which diagnostic imaging indicates that venous thrombosis occurred within the last 14 days. 14 Longer duration of symptoms will influence the results negatively. 15 Do not stop with contraceptive pills before treatment.
Technique
Often the popliteal vein is used for insertion of guide wires for the procedure. 12 The vein is accessed using micropuncture technique under ultrasound (US) guidance in order to avoid multiple punctures and a subsequent risk of bleeding. Fluoroscopy is helping to steer the wire in an intrathrombus position followed by a multi-side-hole catheter with tip occlusion. A venogram is made to map the precise extent of the thrombus. The precise composition of the thrombolytic fluid and volume injected per hour has been described in detail previously. 12
Some studies describe the use of the posterior tibial or sural vein approach in cases of popliteal or calf vein thrombosis.13,16 In our department, infusion of the thrombolytic agent is done using the pulse-spray technique in almost all cases. Venography is used to evaluate thrombolysis and is performed every 24 hours.
As patients are immobilized during treatment, the calf muscle pump is compromised and therefore an intermittent pneumatic compression device (IPC) is used in order to encourage maximal antegrade flow from the ankle through the previously thrombosed vein. The fluctuations of D-dimer during the treatment are very useful. The level will rise soon after thrombus resolution and CDT should continue at least some hours even though the level of D-dimer is almost normalized. These observations are done parallel to biplane venograms demonstrating fully lysed and patent vein segments (Figure 1).
A typical stenosis at the compression site at the end of the arrow. It is obvious that ballooning has no place here. Stent in the venous system is mandatory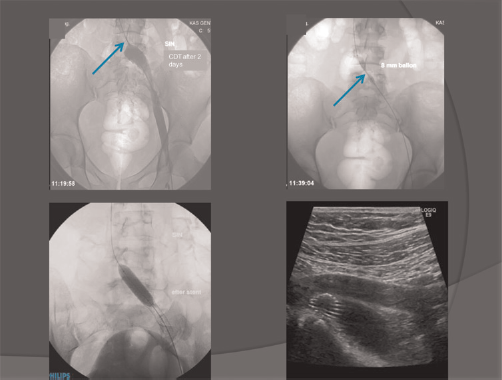
Vena cava filter
In some cases, the iliofemoral DVT extends into the inferior vena cava (IVC), and a prophylactic IVC filter can be inserted. The filter can be inserted from the contralateral femoral vein or from the jugular vein. One paper has described filter placement in all patients to prevent PE, 17 whereas others have used filters only in case of free floating thrombus in the IVC. 18 We have used retrievable filters only in cases of free floating thrombus in the IVC. 12 However, the need for a filter is questionable.
Biochemistry
Haemostasis monitoring is performed by daily analysis of haemoglobin, fibrinogen, APTT, thrombin time, antithrombin and platelet count. The APTT is monitored to assess the effect of intravascular use of unfractionated heparin. A high level of APTT or decline in fibrinogen and haemoglobin has to be observed and thereby the dose lowered or the infusion temporarily stopped parallel to a careful search for bleeding.
Monitoring in the clinical ward
The nursing staff has a great responsibility for making the stay of the patient as safe as possible. The patients are lying flat with the head tilted 30–40 degrees without permission for the toilet. No bladder catheterization is used. This regimen will keep the thrombolysis catheter in the correct position. Once per eight hours dedicated nurses are controlling for bleeding, specifically from the puncture site, in the urine and from the vagina. Blood pressure, pulse and oxygen saturation is controlled. The doctors are responsible for mixing the correct dosages of the lytic fluid and for taking care of the infusion machine. Often, bleeding from the popliteal fossa leads to an extra compression bandage. Continuous bleeding episodes call for supplementary blood samples as previously mentioned. A psychological aspect shall not be forgotten, while these patients are often young and anxious for the outcome. This requires handling with repeated explanations and care of the patients and their families.
Definitions of complications
Complications can be described as major and minor. Major bleeding is defined as intracranial bleeding or bleeding severe enough to result in death, surgery, and cessation of therapy or blood transfusion. Minor bleeding is defined as less severe bleeding that can be managed with local compression, sheath upsizing, and/or dose alterations of the thrombolytic agent. PE can be seen at admission or can occur during the procedure due to thrombus manipulation. 14
Results from the Copenhagen experience
Almost 200 patients have been treated with CDT in the Vascular Clinic in Copenhagen so far. For this chapter we have looked more carefully into the rate and type of complications than appears from our previous publications and looked at the long-term results in the group of patients treated in the period 1999–2006. The basis for the results presented here is 89 patients, two patients treated bilaterally meaning 91 extremities with acute iliofemoral DVT.
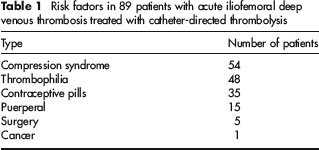
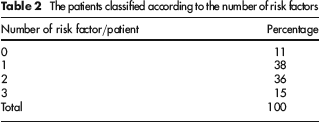
The material consists of 70 women and 19 men with mean age of 29 years (range 14–57 years). All patients with a surgical or puerperal procedure (20 patients) waited a minimum of seven days before CDT. As expected a lot of risk factors are present in this category of patients with substantial overlap. Only a minor part of the material could not be identified as having any obvious reason (Tables 1 and 2).
Risk factors in 89 patients with acute iliofemoral deep venous thrombosis treated with catheter-directed thrombolysis
The patients classified according to the number of risk factors
Complications associated with catheter-directed thrombolysis in 89 patients (91 extremities), Copenhagen experience

PE, pulmonary embolism
*Some patients had more than one type of minor bleeding
Often the question concerning PE occurring during treatment has been raised. PE is a ‘none existing’ problem during CDT in our material. The clot disappearance is a dissolving process rather than a ‘clot fracture’ process. Another point is the fact that most iliofemoral DVT episodes are left-sided with an underlying compression syndrome in almost half of the cases thus preventing PE at least theoretically. Finally, we have inserted a retrievable cava filter in eight patients with a floating thrombus. Sometimes, the retrieved filter demonstrated thrombus inside, but this does not necessarily speak for a possible risk of PE. On the other hand, an empty filter can mean that clot material has been lysed by the t-PA. The low procedural occurrence of PE is already published many years ago.13,16 Reports of only very few deaths directly related to CDT have been published. 13
Efficacy
The average time for CDT was 2 1/2 days. Stenting was performed in 54 procedures (61%). In five cases two stents were necessary to cover the obstructive lesion. A Wallstent was used in most cases. In three cases a procedural stent occlusion occurred with successful re-CDT in two patients supplemented with an extra stent in one case. At follow-up one patient had a stent-related occlusion without success after re-CDT Removal of a stent in another patient was done due to pain in the groin. Substitution with a polytetrafluoroethylene (PTFE) graft solved the problem.
The patients were followed yearly with US examination for patency in the supine position and valve sufficiency in a standing position. Retrograde flow >1/2 second was defined to be reflux in all vein segments except >1 second in the common femoral vein. The outcome for the treated limbs is seen as a Kaplan-Meier plot in Figure 2. The mean follow-up was 87 months (range 17–148 months).
Kaplan–Meier plot illustrating competent vein after catheter-directed thrombolysis (CDT) for acute iliofemoral deep venous thrombosis (DVT) meaning patent veins without reflux
Patients had been kept on anticoagulation (AC) treatment along with recommendation for short compression stockings for two years. Lifelong AC treatment had been advocated strictly in almost 40% of the material due to prior PE, cava atresia and severe thrombophilia.
These results are based on the longest follow-up study presented in the literature, and the results are still at the same level compared with previous results from our group of patients with shorter mean follow-up. Concerning PTS judged from the Villata score we have published on 109 patients with a mean follow-up of 71 months demonstrating PTS in 16.5% of the patients with same technical success rate 20 also reflecting greater quality of life (QOL) in patients with competent veins compared with those with valve insufficiency and/or chronic occlusion.
Recommendations
Concerning safety
Although no consensus exists in the endovascular treatment approach to iliofemoral DVT, we believe we have demonstrated a safe and effective treatment strategy. Using simple and constant precautions before and during CDT, the treatment is a minimal risk for the patient. Our recommendations are a thorough anamnesis, continuation of contraceptive pills during treatment, micropuncture technique using US guidance and bedridden flat. Careful observation once every eight hours checking for bleeding as well as haemostasis monitoring with analysis of haemoglobin, fibrinogen, APTT, thrombin time, antithrombin and platelet count are very important aspects to ensure a safe treatment. All the above-mentioned factors make it possible to treat these patients in a clinical ward and not in the intensive care unit.
Concerning efficacy
The immediate success is based on a high thrombolytic concentration and a high volume injection rate. Use of IPC is used to facilitate flow in the thrombo-lysed vein segment. Following D-dimer together with repeated biplane venograms are recommended. Eager stent placement in the iliac vein is necessary. A post procedural regimen with AC treatment, use of compression stockings and close follow-up is also very important for an optimal outcome.
Conclusion
CDT is a safe treatment modality performed under conditions with simple biochemical monitoring and careful nursing in a clinical ward without any reported mortality in the last decennium directly related to CDT. The complications are minor concerning bleeding, and PE almost does not exist. Using standards for the technical aspects of the procedure, the real long-term efficacy is demonstrated being on a high level. Randomized controlled trials appearing in some years will hopefully support the initial reports by significantly preventing PTS.