
Abstract
Varicose veins occur in up to one-third of Western populations and are associated with clinical manifestations ranging from asymptomatic, isolated varicose veins (C2 disease) to venous ulceration. While the development of less invasive treatment options, such as endovenous ablation and sclerotherapy, have been well accepted by patients they have led to increased utilization of scarce healthcare resources. While few would argue with the treatment of acute complications such as superficial venous thrombosis and variceal haemorrhage, the role of interventional treatment in the management of lifestyle limiting symptoms and the prevention of disease progression may be debatable. Good-quality evidence does suggest that surgical management of varicose veins is associated with improved quality of life at costs below the thresholds of many Western healthcare systems. However, the progression of isolated C2 disease to advanced chronic venous insufficiency occurs infrequently and the role of treatment to prevent such progression remains undefined at present.
Introduction
Varicose veins are the most common clinical manifestation of chronic venous disease, occurring in one-quarter to one-third of Western adult populations.1,2 They may be present either in isolation (CEAP clinical class 2) or in association with more advanced chronic venous disease. Even among patients with isolated C2 disease, the severity of clinical manifestations varies considerably including patients who are destined to remain asymptomatic, patients with acute complications such as superficial venous thrombosis and haemorrhage, those with lifestyle-limiting symptoms, and occasionally those who will progress to advanced skin changes and ulceration (C4–C6). As many as one-third of patients never seek medical attention for their varicose veins or chronic venous insufficiency, 3 but skin changes and ulceration may develop in 2–5% of Western populations. 4 Although a variety of treatments may alleviate the clinical manifestations of varicose veins, they are ultimately a chronic disease for which no true ‘cure’ is available. Although there are patients who seek treatment solely for cosmetic concerns, many of these manifestations may warrant treatment based upon medical or quality-of-life concerns.
Indications for the treatment of varicose veins in C2 disease
Symptomatic varicose veins
Symptoms associated with varicose veins include aching, heaviness, cramps, tingling and pruritis, the prevalence of which increase with age despite only a very limited association with the presence of trunk varicosities.4,8,9 No single symptom is pathognomonic for varicose veins and similar symptoms have been noted in 33% of men and 50% of women without varicose veins. 10 Women are more likely to report venous-associated leg symptoms than men. 11 However, despite the nonspecific symptoms associated with varicose veins, quality of life among afflicted patients is significantly lower than population norms. The physical domains of quality of life tend to be more adversely affected than the mental domains. 12 The treatment of symptomatic varicose veins based upon quality-of-life concerns has merit, but the medical rationale for treatment requires some consideration of the underlying pathophysiology.
Recent theories on the origin of varicose veins have focused on intrinsic structural and biochemical abnormalities of the vein wall. Such ‘weak wall’ theories hypothesize that varicose veins develop because of underlying connective tissue defects and altered venous tone. 13 16 Regardless of the underlying mechanisms, venous valvular incompetence or reflux is the primary haemodynamic abnormality in most cases of primary venous disease. There also appears to be an underlying inflammatory component to chronic venous disease as first suggested by the observation of leukocyte sequestration in the dependent lower extremities, as well as the upper extremities, of patients with chronic venous insufficiency. 17 19 This phenomenon appears to occur early in the course of chronic venous disease and has been observed both in limbs with varicose veins and with lipodermatosclerosis. 20 22 The microvascular endothelium is a critical regulatory site for inflammation and the interaction of leukocytes with the endothelium under conditions of venous hypertension appears to be important in the pathophysiology of chronic venous disease. Leukocyte adhesion, activation and migration are mediated by endothelial adhesion receptors, which function as counter ligands to those expressed on the leukocytes. It has been speculated that upregulation of endothelial adhesion molecule expression occurs in response to hydrostatic pressure-mediated changes in flow or shear23,24 and increased circulating levels of endothelial leukocyte adhesion molecule-1 (ELAM-1), intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) have been demonstrated in patients with chronic venous disease.19,20 Concurrent leukocyte activation20,22,25 is responsible for many of the subsequent manifestations of venous disease including increased capillary permeability and altered tissue re-modelling.
The treatment of C2 varicose veins is based more on relief of symptoms and an attempt to correct the altered haemodynamics than on an understanding of the cause. Options for the management of symptoms associated with varicose veins include pharmacological treatment, compression garments, and interventions directed towards either incompetent saphenous trunks (stripping, thermal ablation, foam sclerotherapy) or their tributaries (phlebectomy sclerotherapy).
The phlebotonics are a heterogeneous group of drugs, largely derived from plant extracts. Although not universally available, these include the saponins, such as horse chestnut seed extract (HSCE); the gamma benzopyrones (flavonoids), such as rutosides, diosmins, hesperidin and micronized purified flavonoid extract (MPFF); and synthetic products such as calcium dobesilate. 26 Any efficacy of these drugs presumably results from modification of the inflammatory processes discussed above. Aescin, the active component in HCSE, inhibits the activities of elastase and hyaluronidase, theoretically released from activated leukocytes in chronic venous disease.27,28 Decreased proteoglycan degradation may reduce vascular filtration, leading to a reduction in oedema. In animal models, MPFF decreases post-ischaemic leukocyte activation resulting in decreased macro-molecular permeability in the microcirculation. 29 Clinically, MPFF has been found to correspondingly decrease plasma levels of endothelial adhesion molecules (VCAM-1 and ICAM-1) in patients with venous disease. 29 It has been suggested that the reduction in adhesion molecules may be mediated by the known ability of the flavonoids to inhibit cytokine production through phosphodiesterase pathways. 28 Reduced leukocyte activation may also be responsible for the complement-modifying effects and diminished platelet aggregation observed with many of the flavonoids. 28 In addition to their effects on leukocyte activation, some, although not all, flavonoids have been demonstrated to inhibit prostanoid biosynthesis through the lipoxygenase and cyclooxygenase pathways. 28
There is also a suggestion of clinical benefit for at least some of the phlebotonic drugs. A meta-analysis of 44 randomized clinical trials evaluating oral phlebotonics demonstrated significant improvement in the signs and symptoms of oedema, although the results were inconclusive for other manifestations of venous disease. 30 Unfortunately, the overall data are of low quality with little long-term data on the safety and efficacy of these drugs. A similar meta-analysis of 17 randomized trials specifically evaluating horse chestnut seed extract (active component the saponin aescin), demonstrated significant improvement in the symptoms of leg pain, oedema and pruritis as well as a mean reduction in leg volume of 32.1 mL (95% confidence interval: 13.49–50.72). 27 Where available, the Guidelines of the Society for Vascular Surgery and the American Venous Forum (SVS/AVF) weakly recommend (2B) the use of phlebotonic drugs for the management of pain and swelling due to chronic venous disease. 26
Compression therapy has traditionally been considered standard therapy for the management of symptomatic varicose veins. Although inconsistently supported by data, the beneficial effects of compression in chronic venous disease have been variously attributed to increased venous flow velocities, reduced venous volumes, reduced ambulatory venous pressure, improved calf muscle pump function and reduced shear. Such haemodynamic benefits have been hypothesized to reduce oedema through counteraction of transcapillary starling forces, to enhance oxygen and nutrient diffusion to the skin, and to suppress cytokines such as vascular endothelial growth factor and tumour necrosis factor-a (TNF-α). 31 Unfortunately, many of the putative haemodynamic effects of compression are not consistently supported by the evidence. For example, time-averaged peak velocities in the popliteal vein in healthy volunteers were not significantly different with or without compression stockings in either the upright or supine positions. 32 Similarly, 20–30 mmHg compression stockings have not been shown to significantly reduce the diameters of refluxing saphenous veins in either the supine or standing position. 33 However, compression does appear to improve the ejection fraction of the calf muscle pump in patients with chronic venous disease, inelastic compression being more effective than elastic compression. 34 Perhaps more importantly, compression stockings increase wall shear stress in the calf veins and altered shear may be a critical mediator of the microcirculatory effects of compression stockings. 35 Endothelial cells are known to respond to changes in shear stress with modifications of their cytoskeletal structure and gene expression. 36 As for their role in deep venous thrombosis prophylaxis, compression-mediated increases in shear may favour an anti-thrombotic endothelium in the microcirculation. Low in vitro shear rates have been associated with erythrocyte adhesion to both activated platelets and neurophils. 37 The clinical relevance of this observation is suggested by the finding that the use of compression stockings in healthy volunteers is associated with significant increases in tissue factor pathway inhibitor levels. 38 Similar to the anti-inflammatory effects of the phlebotonic drugs, compression-mediated increases in shear may also lead to an antiinflammatory microcirculatory endothelium, an observation that may have relevance in chronic venous disease. Preconditioning cultured endothelial cells under conditions of high shear stress results in dramatic reductions in neutrophil adhesion, possibly due to reduced upregulation of E-selectin by inflammatory stimuli such as TNF-α. 36 Clinically, suppression of a variety of cytokines has been observed in the skin of ulcer patients treated with compression bandages. 39
Although the role of compression in advanced venous disease is well supported by the evidence, the clinical benefit of compression in C2 disease is substantially less clear. Observational data suggest that compression will provide some symptomatic relief in about 30% of patients with varicose veins. 40 Comparisons to placebo are very limited, but also suggest some improvement in symptoms with the use of compression stockings. 41 A small randomized trial evaluating the utility of compression during pregnancy found stockings to be superior to no compression in the relief of symptoms, but to be ineffective in preventing emergent varicosities. 42 However, the symptomatic improvement seen with compression stockings is clearly less than after surgical treatment of varicose veins 40 and approximate that associated with the phlebotonic drugs. A randomized trial including 246 patients demonstrated compression therapy to be equivalent to HCSE but superior to placebo in reducing plethysmographically determined leg volume. Although no patient important outcomes were included in this trial, both HSCE and compression provided a relatively modest, approximately 25%, reduction in oedema volume. 43 The authors of one systematic review concluded that the benefits of compression as a first-line treatment are limited. 41 Although the SVS/AVF guidelines weakly (Grade 2C) recommend moderate compression for patients with symptomatic varicose veins, compression is not recommended as primary treatment in patients who are candidates for saphenous ablation (Grade 1B). 26
In contrast to the evidence for compression, high-quality evidence does support the value of surgery in the management of symptomatic varicose veins. All domains of the SF-36 improved after high ligation and stripping in 137 patients with varicose veins, reaching statistical significance for mental health and approaching significance for general health. 12 The Aberdeen varicose vein questionnaire showed a highly significant improvement after surgery. The REACTIV trial 40 randomized patients with varicose veins to conservative management versus surgery and demonstrated significantly greater improvement in symptoms and quality of life in the surgical group. Although 31% of patients did have some improvement with compression hosiery alone, 51.6% of patients assigned to conservative management crossed over to surgical treatment by the third year of follow-up. Surgery was more expensive, but its incremental cost-effectiveness ratio of £4682 per quality-adjusted life year (QALY) gained was well below the National Health Service willingness to pay threshold of £20,000 per QALY 44 Interventional management with either surgical or endovenous techniques is well supported by the data and is recommended as the treatment of choice for symptomatic saphenous vein reflux in C2 disease. 26
Prevention of disease progression
Varicose veins and chronic venous insufficiency are slowly progressive, chronic conditions. However, it is not entirely clear that concerns regarding progression are a valid indication for the treatment of isolated C2 disease. Although up to 10% of varicose veins patients presenting to specialized clinics may have ulcers, 45 progression from C2 disease to advanced chronic venous insufficiency is reasonably rare. While the prevalence of varicose veins in Western populations may be as high as 30–50%,4,46 that of skin changes and ulceration is only 2 to 5% of Western populations. 4 However, open ulcers constitute only 20–25% of the total and the population prevalence of open and healed ulcers may be closer to 1%.47,48 Despite concerns about disease progression, most patients with C2 disease do not progress to skin changes and ulceration.
The development of advanced chronic venous disease is a multifactorial phenomenon. Among patients with advanced chronic venous insufficiency, females generally predominate at all ages with a female-to-male ratio of 2:1 to 3:1. 47 49 The incidence of venous ulcer is highest in older patients and initial ulceration occurs after age 50 in 60% of patients. 50 Many factors such as gender and parity lose their significance when adjusted for age. Other prognostic factors that have been associated with more severe venous insufficiency include weight, a history of thrombophlebitis, the post-thrombotic syndrome, exposure to environmental heat, and occupations including being a pensioner or housewife. 51 Disease progression in legs contralateral to limbs managed for varicosities has been associated with a family history of venous disease as well as >4 hours a day of continuous standing, obesity and failure to use compression stockings. 52 Genetic factors may also play a role in progression to advanced chronic venous disease and a relationship between the C282Y polymorphism in the haemochromatosis (HFE) gene and venous ulceration has been described.53,54 Some symptoms, such as a ‘feeling of swelling’, 55 and physical findings, such as corona phlebectatica, may also be early markers of progression to advanced disease. 56
Distribution of reflux in patients with venous ulcers
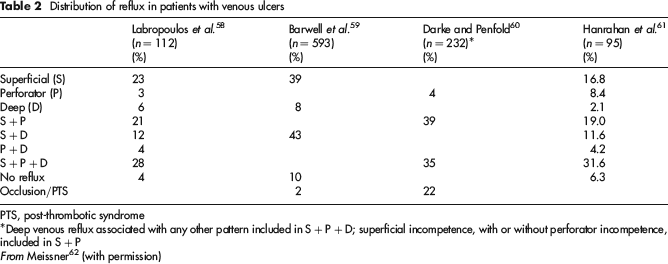
PTS, post-thrombotic syndrome
*Deep venous reflux associated with any other pattern included in S + P + D; superficial incompetence, with or without perforator incompetence, included in S + P
From Meissner (with permission)
Unfortunately, as most patients with symptomatic primary disease are treated early after presentation, the rate of progression from uncomplicated varicose veins to skin changes and ulceration remains very poorly defined. Some studies have suggested progression to skin changes and ulceration in as many as 22% and 4% of patients an average of four years after initial presentation. 6 However, most studies have suggested lower rates of progression to advanced venous disease. In one small study of 36 patients in whom varicose vein surgery was deferred for a median of 20 months, no patient developed a new ulcer and new lipodermatosclerosis developed in one of 50 limbs at risk. 57 However, as the authors noted, this was a select group that was felt likely to remain stable while awaiting operation. Kostas et al. 52 followed 73 contralateral limbs, 93% of which were without symptoms, for five years after unilateral varicose vein surgery. Although a clinical deterioration of ≥2 CEAP classes was noted in 23 (32%) limbs, only 2 (3%) limbs progressed to C4 disease and no limb developed an ulcer. The best data perhaps come from the Bonn Vein Study II, in which the incidence of progression to C3–C6 disease was only 2% per year. 55
Although the development of skin changes and ulceration undoubtedly progress from less advanced C2 disease, it is not entirely clear that the risk of progression warrants treatment of most patients with C2 disease. Data regarding the number needed to treat are sparse, although one Swedish study suggests that 100 patients with symptomatic varicose veins would need to be treated to prevent one ulcer. 55 The cost-effectiveness of such a strategy is unknown, although it is likely that strategies to identify those patients with risk factors placing them at high risk for progression would be much more efficient. Unfortunately, compliance with behavioural modifications (weight loss, compression) that might decrease the risk of disease progression in at-risk patients is low. 52 An expert group convened by the Pacific Vascular Symposium 6 with the express goal of reducing the incidence of venous ulcers by 50% concluded that more research on the natural history of primary chronic venous insufficiency is required and that additional information on the factors responsible for disease progression, including clinical, mechanical, humoral, genetic and endothelial risk factors, is needed. 55
Summary
Varicose veins are among the most common afflictions of Western civilization, developing in up to one-third of the population. The clinical manifestations of varicose veins also vary broadly from relatively asymptomatic C2 disease to advanced skin changes and ulceration. Well-established indications for the treatment include the development of complications such as advanced skin changes and ulceration, variceal haemorrhage, and recurrent superficial phlebitis. Less clear indications for treatment include cosmetic concerns, lifestyle-limiting symptoms and prevention of disease progression. Although cosmetic indications are certainly of importance to some patients and may warrant treatment, there is little medical rationale for treatment in such cases. However, many patients do present with lifestyle-limiting symptoms and the weight of the evidence suggests that although there may be a role for phlebotonic drugs and compression, surgical extirpation or ablation of incompetent superficial veins leads to superior symptom relief and quality of life. In contrast, the limited existing data suggest that only a minority of patients with C2 disease progress to advanced chronic venous insufficiency. Routine surgical treatment for the sole indication of preventing progression to advanced chronic venous disease is likely less cost-effective than strategies to identify patients at high risk of disease progression. The factors influencing the progression of chronic venous disease are poorly characterized, but include a number of clinical risk factors as well as the magnitude, duration and anatomic distribution of reflux.