
Abstract
Endovenous laser ablation (EVLA) and radiofrequencey ablation have become the procedures of choice for the treatment of superficial venous insufficiency. Their minimally invasive technique and safety profile when compared with operative saphenectomy have led to this change. As EVLA has replaced saphenectomy as the procedure of choice, the distribution of complications has changed. We evaluated the most common and most devastating complications in the literature including burns, nerve injury, arteriovenous fistula (AVF), endothermal heat-induced thrombosis and deep venous thrombosis. The following review will discuss the most frequently encountered complications of treatment of superficial venous insufficiency using EVLA. The majority of the complications described can be avoided with the use of good surgical technique and appropriate duplex ultrasound guidance. Overall, EVLA has an excellent safety profile and should be considered among the first line for treatment of superficial venous reflux.
Keywords
Introduction
Common complications described in the literature by reporting country
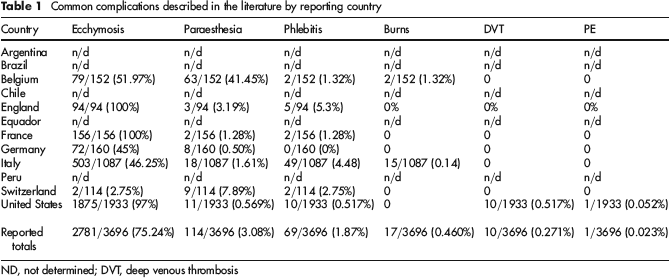
ND, not determined; DVT, deep venous thrombosis
Superficial burns
During EVLT, there can be a significant amount of heat dispersed around the vein intended for treatment. The heat generated by the laser during ablation leads to contraction of the collagen within the vein wall, denudation of the endothelium and ultimately venous contraction and occlusion. The majority of heat generated remains within the venous lumen. When the vein becomes epifascial or close to the skin surface, the patient can suffer a full thickness burn to the skin. Superficial burns have been extensively reported in the literature after endovenous ablation. Merchant et al. 1 first reported a 4.2% rate of skin burns in the first 143 of 286 limbs using RFA. They subsequently reported a 0% burn rate in their next 143 limbs treated. They attributed the decrease in the rate of skin burns to a better use of tumescent anaesthesia, allowing for more heat dissipation and less transmission directly to the overlying skin. Later, multinational registries have documented skin burn rates of 0.14–1.32% with EVLA. 2 In reviewing the literature, there appears to be a trend towards a higher incidence of skin burns with RFA than EVLA; however, there has never been a study showing statistical significance. While cutaneous skin burns can be painful and unsightly, they appear to be self-limited and do not appear to be associated with any other significant complications. They can be treated with local wound care and followed clinically to evaluate for skin infection. If the burn is apparent immediately at the time of ablation, it can be excised with primary wound closure. The incidence of skin burns is low, and most can be prevented by appropriate tumescent anaesthesia and avoiding treatment of veins that are close to the skin surface.
Nerve injury
The risk of nerve injury during EVLA is directly related to the relative proximity of several nerves to the most commonly ablated veins. The saphenous nerve, the largest cutaneous branch of the femoral nerve, travels along the path of the superficial femoral artery from the groin to the knee. At the popliteal fossa, it travels medially and approximates the great saphenous vein (GSV) at the level of the upper calf to the level of the ankle, where it splits into two branches. It is at greatest risk of injury in the mid- to distal calf where it can be directly injured from a needle stick or burned by transfer of energy from the laser. Injury to the great saphenous nerve causes a cutaneous paraesthesia, which is usually transient.
The sural nerve, also known as the short saphenous nerve, is a cutaneous nerve that originates in the mid-posterior calf that travels alongside the small saphenous vein (SSV) down to the lateral malleolus. It is at greatest risk of injury in the distal calf where it is in close proximity to the SSV, where it can be directly injured from a needle stick or from heat transfer during laser ablation. This relationship can be identified on ultrasound at the time of procedure (Figure 1). Injury to the sural nerve causes a cutaneous paresthesia, which is usually transient. Huisman et al. 3 found, in recent literature, a rate of sural nerve injury of 1.3–11% during EVLA of the SSV In their own population, they reported a 1.3% sural nerve injury rate with 100% recovery of sensation at six months.
The common peroneal nerve is a motor and sensory cutaneous nerve that descends within the lateral popliteal fossa, posterior to the head of the fibula. It lies in close proximity to the saphenopopliteal junction. While it is not at risk of direct needle injury during EVLA, it is at risk of being injured from heat transfer from the laser while treating the saphenopopliteal junction. In a cadaveric study by Balasubramaniam et al.,
4
93% of peroneal nerves were identified in the normal or low position, and were on average 2.3 and 1.6 cm away from the saphenopopliteal junction, respectively.
Duplex ultrasound of the small saphenous vein (SSV) and its proximity to the sural nerve
Chang et al. 5 found that EVLA without tumescence had a 36.5% incidence of local paraesthesias related to the neighbouring nerves. All of these injuries were self-limited and had completely resolved within three weeks. Merchant found that using RF, the paraesthesia rate with the addition of tumescence dropped from 15% to 9%. 6 Kabnick 7 later found that the paraesthesia rate for himself, Almeida and Min was 2.5%, 1.5% and N/A with RFA and 0.27%, 0.16% and 0% with EVLA, respectively. Many of these nerve injuries can be avoided by careful needle entry under ultrasound guidance, large volume tumescence and avoidance or judicious use of ablation in areas at high risk of nerve injury.
arteriovenous fistula
The risk of arteriovenous fistula (AVF) creation during venous ablation is extremely rare. There have been 11 cases of AVF reported in the literature to date, and the majority of them have occurred after EVLA. 8 14 Rudarakanchana et al. 8 have reported an incidence of 0.15% after RFA or EVLA. While the cause of AVF creation during endovenous ablation remains unknown, there are two likely aetiologies that are usually considered. Concomitant venous and arterial injuries during administration of tumescent anaesthesia, as well as transmission of thermal energy across the venous wall into the neighbouring artery, leading to late vascular wall degradation and formation of an AVF. The details of the procedure leading to AVF following EVLA are sparse. They have been witnessed in both an 810 nm diode laser as well as a 1320 nm Nd:YAG laser. Maximum energy density delivered that was documented was 61 J/cm.
Patient symptoms after AVF varied greatly. Six of 11 patients had no symptoms and their fistula was found in routine post-procedure duplex examination. Only three patients complained of leg swelling. One patient, who developed an AVF at the common femoral vein developed high-output cardiac failure, and decompensated while developing severe dyspnea, abdominal distention and leg swelling. 14
The majority of AVF were detected on postoperative duplex ultrasound (Figures 2 and 3). While one AVF was reported at two years after procedure, the majority were seen within the first 30 days of treatment. When duplex ultrasound showed the presence of AVF, but could not identify the location, further imaging with computerized tomography or magnetic resonance imaging was utilized to identify the fistula in the majority of patients. Interestingly, creation of an AVF was associated with a significantly high rate of GSV recanalization (3 of 7), while there have been no cases of SSV recanalization reported.
Duplex ultrasound of arteriovenous fistula (AVF) between the great saphenous vein (GSV) and a branch of the external pudendal artery (EPA). Common femoral artery (CFA), common femoral vein (CFV) and EPA) are also labelled Duplex ultrasound and Doppler tracing showing (a) arterialized flow in the GSV and (b) blunted waveforms and reversed flow in a branch of the external pudendal artery

The literature also supports a conservative approach to management of AVF associated with EVLA. Five patients required further intervention including open repair, embolization and stent grafting. While only three of 11 closed spontaneously, three were persistent in long-term follow-up and remained asymptomatic. The literature appears to support non-operative management and observation of the majority of AVF associated with EVLA. These patients can be followed with serial clinical exams and duplex ultrasound. Invasive imaging and surgical or endovascular treatment should be reserved for patients who become symptomatic.
While AVF following EVLA is a rare event, certain technical considerations may mitigate the risk. The branches of the deep external pudendal artery courses posterior to the proximal GSV, and the sural artery branches are in close proximity to the SSV in the popliteal fossa. It is important to utilize high-volume tumescent anaesthesia in these areas to separate the vein from any arterial branches as well as to dissipate the heat during ablation. Ultrasound guidance should also be utilized during needle entry as well as during infiltration of tumescent anaesthesia to guide against inadvertent concomitant arterial and venous injuries.
EHIT and DVT
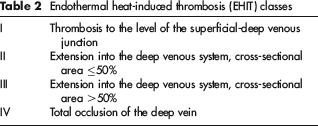
EHIT is defined as the propagation of thrombus from the superficial vein into a more central deep vein. This finding can have significant consequences as it can lead to DVT and pulmonary embolism (PE). In van den Bos‘ 15 review of the literature, the incidence of DVT after EVLA ranges between 0% and 5.7%. EHIT is classified on the extent of thrombus that has propagated into the deep system (Table 7). 7 EHIT I is generally considered to be clinically insignificant as there is no propagation of thrombus into the deep venous system. As such, it is usually not reported in the majority of the literature.
Puggioni et al.
16
evaluated 130 procedures retrospectively who were treated using either EVLA or RFA. The catheter was placed 1 cm from the saphenofemoral junction. They reported three (2.3%) patients with thrombus propagation into the deep system, consistent with an EHIT II (Figure 4). All these patients with thrombus propagation were treated using EVLA. Marsh et al.
17
later reviewed 2470 patients treated with either RFA (n = 2120) or EVLA (n = 350). They reported seven patients with thrombus propagation into the deep system, consistent with an EHIT II-IV, with no significant difference in EHITs between EVLA (3) or RFA (4). Interestingly, they did report 15 isolated gastrocnemius or soleal muscle DVTs and one PE. Sadek and Kabnick have retrospectively evaluated 3083 of their patients who were treated with either EVLA or RFA. They found 74 EHIT II patients, with no significant difference between groups (18 [1.9%] in the EVLA group and 56 [2.6] in the RFA group, P = 0.31).
18
Duplex ultrasound demonstrating an endothermal heat-induced thrombosis (EHIT) II: thrombus with a cross-sectional diameter less than 50%
All patients who undergo EVLA should have routine duplex ultrasound screening to evaluate for successful ablation of the treated vein segment as well as to evaluate for thrombus propagation. Kabnick et al.
7
recommended treatment of EHIT II patients with low-molecular-weight heparin until resolution of the thrombus on ultrasound. Sadek and Kabnick
18
have gone further in developing a treatment algorithm for EHIT based upon propagation severity (Figure 5).
Treatment algorithm for EHIT based upon propagation severity. US: ultrasound, EHIT: endothermal heat-induced thrombosis, LMWH: low-molecular-weight heparin, C: Coumadin (i.e. anticoagulation) Endothermal heat-induced thrombosis (EHIT) classes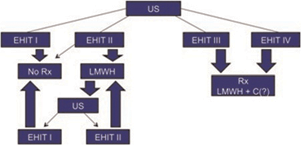
Pain and bruising
Open saphenectomy as well as endovenous ablation of the saphenous vein is strongly associated with pain and bruising at the site of the treated vein. Many authors have included ecchymosis as a complication of EVLA (Table 1). The published rate varied from 2.75% to 100% in the countries that reported complications. The wide variation between reported rates is likely due to the expectation that most or all patients will experience some pain and bruising from the procedure. Some centres either reported all of the patients that had any ecchymosis (i.e. UK, France, US), while others only reports patients that had more bruising than was expected (i.e. Switzerland). While we agree that pain and bruising is an expected finding after EVLT, there have been recent advances in laser technology that have shown these to be decreasing.
The initial wavelengths that were used to treat venous insufficiency were on the lower end of the spectrum (810, 940, 980 and 1064 nm) and they targeted haemoglobin as the chromophore. The development of lasers with higher wavelength (1320 and 1470 nm) involved water as the target chromophore. There have been several studies that demonstrate higher wavelength lasers are associated with less pain and bruising. Water-based lasers appear to be more efficient than haemoglobin-based lasers in absorbing light energy. Kabnick 19 found the 980 nm laser had significantly less pain and bruising with similar efficacy when compared with the 810 nm. The 1320 nm laser was later compared with the 940 nm laser, further demonstrating significantly less pain and bruising with similar efficacy with the higher wavelength laser. 20 Mackay 21 reported similar findings when performing patients with bilateral venous insufficiency with a 1320 nm laser on one leg and a 810 nm laser on the other. Although there have been no randomized trials evaluating the 1470 nm laser, we have found less pain and bruising in these patients compared with our other EVLA patients. We believe that the 1470 nm wavelength laser should be the device of choice to optimize postoperative recovery. 22
Further developments in endovenous laser technology have included the development of the jacket-tip fibre and the radial-emitting tip, both designed to eliminate direct contact with the vein wall. In addition, these new fibres limit the density of power that is distributed directly to the vein wall. In one randomized study utilizing the 980 nm laser comparing the jacket-tip fibre to the bare-tip fibre, the jacket-tip had nearly half as much pain as the bare-tip group. 23 In a pilot study by Kabnick, evaluating four groups of 810 and 1470 nm wavelengths with bare-tip and jacket-tip lasers, the combination of lasers with higher wavelength in combination with jacket-tip was associated with the lowest rate of vein wall perforation, likely leading to lower rates of pain and bruising.
Conclusions
Although there are reported complications of EVLA, they are extremely infrequent occurrences. The majority of these complications can be avoided with excellent duplex ultrasound technique and appropriate tumescence. Further problems can be prevented with early detection of complications and treatment when necessary. It is important to understand that in the last decade since the first use of EVLA, the complication rate has continued to fall. This can be explained by improving imaging technology better operative technique, a better understanding of the anatomic relationships of the treated veins, arteries and nerves, and early treatment of complications. Inexperienced users of EVLA should pay heed to the large volumes of literature that have described the potential pitfalls to help minimize their complications by learning from prior mistakes. Overall, EVLA has an excellent safety profile and should be considered among the first line for the treatment of superficial venous reflux.