
Abstract
The first CEAP (clinical, aetiological, anatomical and pathological elements) consensus document was published after a consensus conference of the American Venous Forum, held at the sixth annual meeting of the AVF in February 1994 in Maui, Hawaii. In the following years the CEAP classification was published in many international journals and books which has led to widespread international use of the CEAP classification since 1995. The aim of this paper is to review the benefits and limits of CEAP from the available literature. In an actual Medline analysis with the keywords ‘CEAP’ and ‘venous insufficiency’, 266 publications using the CEAP classification in venous diseases are available. The CEAP classification was accepted in the venous community and used in scientific publications, but in most of the cases only the clinical classification was used. Limitations of the first version including a lack of clear definition of clinical signs led to a revised version. The CEAP classification is the gold standard of classification of chronic venous disorders today. Nevertheless for proper use some facts have to be taken into account: the CEAP classification is not a severity classification, C2 summarizes all kinds of varicose veins, in C3 it may be difficult to separate venous and other reasons for oedema, and corona phlebectatica is not included in the classification. Further revisions of the CEAP classification may help to overcome the still-existing deficits.
Keywords
The first CEAP (clinical, aetiological, anatomical and pathological elements) consensus document was published after a consensus conference of the American Venous Forum, held at the sixth annual meeting of the AVF in February 1994 in Maui, Hawaii.1,2
CEAP classification

In the following years the CEAP classification was published in many international journals and books, which has led to widespread international use of the CEAP classification since 1995. 3 In an actual Medline analysis with the keywords ‘CEAP’ and ‘venous insufficiency’, 266 publications using the CEAP classification in venous diseases are available.
Early criticism of the CEAP classification
From the beginning the new CEAP classification was accepted in the venous community and used in scientific publications. However, in most of the cases only the clinical classification with the C-classes was used. The complete CEAP and also the severity score system were only used occasionally.
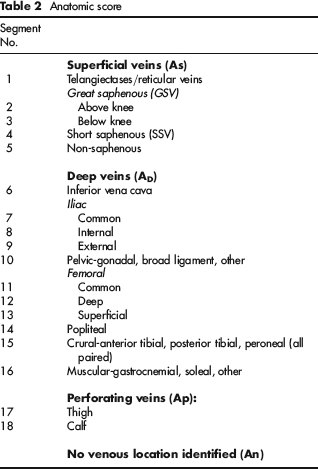
Anatomic score
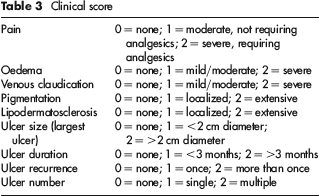
Clinical score
Nevertheless there is still heterogeneity of reporting standards even in randomized clinical trials. Thakur et al. 10 reviewed clinical trials of endovenous interventions for varicose veins and found that the CEAP classification was used in 17/28 randomized trials.
During the 40th World Congress of the Union Internationale de Phlebologie (UIP) in Rome 2001, a conference of experts suggested definitions and refinements of the clinical classification of CEAP. 11
As the clinical score in the CEAP classification was not used in many studies an ad hoc committee of the American Venous Forum presented a new venous severity score system in 2000. 12 In the meantime this venous clinical severity score (VCSS) has been revised. 13
Revision of the CEAP classification
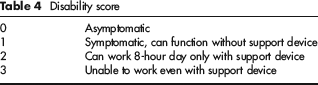
Disability score
Atrophie blanche (white atrophy): Localized, often circular whitish and atrophic skin areas surrounded by dilated capillaries and sometimes hyperpigmentation. Sign of severe CVD, and not to be confused with healed ulcer scars. Scars of healed ulceration may also exhibit atrophic skin with pigment changes, but are distinguishable by history of ulceration and appearance from atrophie blanche, and are excluded from this definition;
Corona phlebectatica: Fan-shaped pattern of numerous small intradermal veins on medial or lateral aspects of ankle and foot. Commonly thought to be an early sign of advanced venous disease. Synonyms include malleolar flare and ankle flare;
Eczema: Erythematous dermatitis, which may progress to blistering, weeping or scaling eruption of skin of leg. Most often located near varicose veins, but may be located anywhere in the leg. Usually seen in uncontrolled CVD, but may reflect sensitization to local therapy;
Oedema: Perceptible increase in volume of fluid in skin and subcutaneous tissue, characteristically indented with pressure. Venous oedema usually occurs in ankle region, but may extend to leg and foot;
Lipodermatosclerosis: (LDS) Localized chronic inflammation and fibrosis of skin and subcutaneous tissues of lower leg, sometimes associated with scarring or contracture of Achilles tendon. LDS is sometimes preceded by diffuse inflammatory oedema of the skin, which may be painful and which often is referred to as hypodermitis. LDS must be differentiated from lymphangitis, erysipelas or cellulitis by their characteristically different local signs and systemic features. LDS is a sign of severe CVD;
Pigmentation: Brownish darkening of skin, resulting from extravasated blood. Usually occurs in ankle region, but may extend to leg and foot;
Reticular vein: Dilated bluish subdermal vein, usually 1 mm to less than 3 mm in diameter. Usually tortuous. Excludes normal visible veins in persons with thin, transparent skin. Synonyms include blue veins, subdermal varices and venulectasies;
Teleangiectases: Confluence of dilated intradermal venules less than 1 mm in calibre. Synonyms include spider veins, hyphen webs and thread veins;
Varicose vein: Subcutaneous dilated vein 3 mm in diameter or larger, measured in upright position. May involve saphenous veins, saphenous tributaries or non-saphenous superficial leg veins. Varicose veins are usually tortuous, but tubular saphenous veins with demonstrated reflux may be classified as varicose veins. Synonyms include varix, varices and varicosities;
Venous ulcer: Full-thickness defect of skin, most frequently in ankle region, that fails to heal spontaneously and is sustained by CVD.
Clinical classification
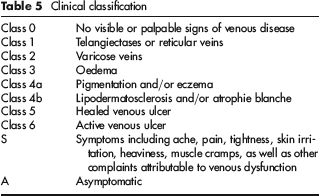
Each clinical class can be associated to clinical symptoms and in this case marked ‘S’ – symptomatic or the absence of symptoms marked in this case ‘A’ – asymptomatic. Symptoms include aching, pain, tightness, skin irritation, heaviness, muscle cramps and other complaints attributable to venous dysfunction. 3
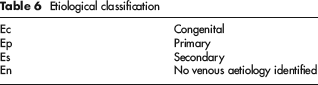
Etiological classification
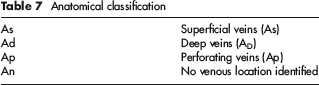
Anatomical classification
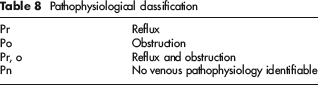
Pathophysiological classification
Level of investigation

IVUS, intravascular ultrasonography; CT, computed tomography; MRV, magnetic resonance venography
The use of the complete CEAP classification with a documentation of all clinical findings and anatomical segments, the level of investigation and the date is recommended for scientific use. For use in the daily practice the Basic CEAP is recommended. In this case the single highest descriptor can be used for clinical classification. A patient with teleangiectases, varicose veins, oedema with atrophy and healed venous ulcers would be classified as C5 whereas in the full CEAP format he would be a patient classified as C1, 2, 3, 4b, 5. In addition, a simplified anatomical classification divided into superficial, deep or perforating veins is used. 3
Discussion
The CEAP classification is the gold standard of classification of CVDs today. Nevertheless for proper use some facts have to be taken into account:
CEAP classification is not a severity classification but describes the clinical and functional situation of the patient. To classify the severity of the disease additional tools like the VCSS or Quality of Life scales have to be used; 14
In the C1 class teleangiectases and reticular veins are summarized although they may have different implications for clinical symptoms;
In the C2 class all kinds of varicose veins are summarized. Saphenous veins in the interfacial space, accessory saphenous veins and non-saphenous tributaries may have different implications not only for the severity of the disease but also for the risk of progression of the disease, clinical symptoms and the choice of treatment. The anatomical classification may add this information. However varicose veins may have a small or a large diameter with implications for clinical symptoms and for the choice of treatment option. The diameter of the vein is not included in the CEAP classification;
The C3 class is defined as oedema in the lower legs. This includes minimal oedema, which occurs only in the evening as well as extensive oedema of the leg. In addition, oedema may not only be caused by venous insufficiency but also by other diseases like cardiac insufficiency or drug treatment. These different diseases may be combined as varicose veins are prevalent in more than 20% of the population and the main cause of the swelling may be difficult to evaluate;
Corona phlebectatica is still not a part of the clinical classification and summarized in the C1 class defined as teleangiectases and reticular veins. However teleangiectases at the foot as corona phlebectatica has a completely different implication for the venous disease compared with isolated teleangiectases in the thigh region. At least corona is now part of the revised VCSS classification; 14
In the severe stages of CVD lymphatic involvement and lymphoedema is a frequent finding. This is not classified in the CEAP classification;
It has to be mentioned that also the critical class C0 can be assorted with pathological venous findings not visible or palpable. Examples are post-thrombotic changes without clinical signs, insufficient saphenous veins without varicose veins and functional venous insufficiency in obesity.
Although the CEAP classes are not a severity classification, reflux prevalence increases with higher C-stages in the superficial veins. 15 Patients’ reported quality of life also decreases significantly with higher C-classes. 16 The clinical class of CEAP also correlates significantly with foot volumetric parameters in CVD patients. 17
Further revisions of the CEAP classification may help to overcome the still-existing deficits of the classification.