
Abstract
Radiofrequency ablation (RFA) has become a valued weapon in the phlebologist's armoury. It offers ease of use and reproducibility with good outcomes. However, as with all interventions, complications arise. In this review we examine the complications inherent with RFA and their relative risk, with their avoidance measures if available. Overall, we find that RFA offers a very safe procedure with rare severe complications.
Introduction
Varicose vein treatment is one of the most common vascular operations performed in the National Health Service 1 with the aim of reducing symptoms and the burden of skin ulceration. 2 The management of varicose veins has changed rapidly in recent years. Saphenofemoral ligation and stripping of the great saphenous vein (GSV) once used to be the standard treatment for GSV reflux but has been challenged and in some areas replaced by endovenous therapies.3,4 Evidence has favoured endovenous modalities in terms of reduced postoperative hospital stay, early return to work and low complication rates.3,5-7
The following endovenous therapies have emerged in practice:
Thermal ablation:
Laser, Radiofrequency, Steam, Cryotherapy.
Non-thermal ablation:
Foam sclerotherapy, Sapheon™ (glue), Clarivein™ (mechanical scarification and liquid sclerosant).
The authors have reviewed the potential complications and possible risks associated with radiofrequency ablation (RFA) of varicose veins.
Radiofrequency ablation
RFA of varicose veins was first described by Goldman in 2000 8 utilizing the VNUS ClosurePlus™ catheter (Covidien, Dublin, Ireland). Since then, two further catheters have been introduced – VNUS ClosureFast™ 9 and Olympus Celon RFITT™ (Olympus, Tetlow, Germany). 10
Radiofrequency energy thermally denatures vein wall collagen, leading first to vein wall inflammation, then fibrosis and finally to occlusion. Surrounding tissues are protected by tumescent local anaesthesia, which acts as both a heat sink and as anaesthetic. 11 The vein lumen is compressed by the tumescent solution around the tip of the catheter, improving energy transfer and reducing power requirements.
The original ClosurePlus™ catheter required a constant pullback technique of 3 cm/minute (0.05 cm/second), whereas the ClosureFAST™ catheter treats a 7 cm segment of vein for 20 seconds (0.33 cm/second). An electronic feedback mechanism with varying power maintains a constant catheter temperature of 120°C in the ClosureFAST™ and 85°C in the ClosurePlus™ system. The Olympus Celon RFITT™ provides bipolar electrode treatment and utilizes a pullback technique with an optimal speed of 1–1.4 cm/second. 12 ClosureFAST™ and RFITT™ have similar treatment profiles versus laser ablation but have not been directly compared. 12
The ability of RFA to treat varicose veins under local anaesthetic has aided the transformation from inpatient operation to outpatient or office-based procedure. The ease of use and high patient satisfaction have led to a surge of interest.13,14
Complications with RFA
All treatments for venous disease involve the risk of adverse events. It is important that the risk of a treatment is small compared with the likely benefits.
Early complications
Closure success
Short-term technical success is defined as the successful occlusion of the vein lumen. Immediate failure of the technique should be identified at the time of the procedure by the completion of a duplex ultrasound scan. Immediate technical success rates of more than 95% with RFA have been reported.3,12,15 A multicentre trial using the ClosureFAST™ catheter has achieved an occlusion rate of 99.6% at six months. 9
Pain
RFA has been found to be associated with less postoperative pain, a lower requirement for analgesia and a reduced impact on daily activities than other treatment modalities.3,5 Rasmussen et al. 3 reported a mean pain score of 1.21/10 during the first 10 days and the time to return to normal activity was only one day. In the VALVV randomized trial comparing RFA with laser ablation, RFA patients reported a mean pain score of 2.2/10 and an analgesia requirement of 10.9 tablets over 10 postoperative days. In all, 60% of patients returned to normal activities within three days. 5 The EVOLVeS study compared RFA with surgery and found that RFA patients returned to normal activities in 1.15 days and had a persistently improved pain score (compared with both baseline and surgery) throughout two years of follow-up. 15 Results from other studies also suggest low pain and analgesic requirements following RFA treatment. 16
Phlebitis
Thrombophlebitis is the presence of inflammation at the site of the treated GSV associated with localized inflammatory changes such as hyperaemia, oedema and tenderness. It can also occur in varicosities and has an association with deep vein thrombosis (DVT). 17 A recent meta-analysis reported an early phlebitis rate of 8% with RFA (by combining the results of three large trials). 7 Recent studies have reported rates of 7–9.6%.3,5 However, Shepherd et al. 5 also had one case of pulmonary embolism following RFA but with no evidence of deep vein thrombosis.
Endovenous heat-induced thrombosis
Thrombus can protrude into the common femoral vein (CFV) as well, an entity called endovenous heat-induced thrombosis (EHIT). 18 20 For safety, the manufacturers recommend the tip of the ablation catheter should be at least 2 cm from the saphenofemoral junction.
In EHIT, thrombus can be seen either:
At the level of the deep vein without protruding into CFV;
Projecting into the deep system with <50% luminal occlusion of CFV;
Protruding into the deep system with more than 50% luminal occlusion;
Causing complete occlusion of the deep system – in other words, a full DVT.
A recent small-scale study into GSV patency and EHIT after RFA showed a 2.7% (2/73) rate of class II EHIT with no DVT, 20 which corresponds to earlier work by Mozes et al. 19 of 2.1% and Lawrence et al.; 21 however, Proebstle et al. 9 found a rate of 0% from 252 patients with ClosureFAST and Marsh et al. 22 found a rate of 0.4% from 2470 limbs.
Cases of EHIT class II have been successfully treated with two weeks of low-molecular-weight heparin (LMWH) with complete resolution in all cases. 20 For classes III-IV full DVT treatment is recommended. 18
Deep vein thrombosis
DVT can develop in the calf deep veins or a thrombus can circulate from the treated superficial veins (as described above) following RFA. DVT after endovenous ablation is extremely rare and indeed most case series and trials show no evidence of DVT at all.3,7,23,24. This makes quoting advice and risks difficult – the 2011 Venous Forum meeting at the Royal Society of Medicine had a dedicated session for debate on this issue, due to limited evidence.
Most clinics quote risks of approximately 1:1000 and provide perioperative prophylaxis. 22 Concomitant small saphenous vein surgery or transluminal occlusion of perforator with RFA have been considered risk factors for high calf DVT. 22
Risks are reduced by the postprocedural use of compression stockings, the use of local anaesthetic and patients walking in and out. However, once again there are no detailed data for guidance.
Pharmacological prophylaxis may be used for all patients undergoing treatment or only in selected cases. Universal coverage prevents missed cases but is probably unnecessary in many patients. Selective treatment provided on the basis of risk assessment will miss some cases in need of prophylaxis and increase clinical load.
Patients at high risk of DVT (active malignancy, age over 60, known coagulation disorders, one or more significant medical co-morbidities, use of oestrogen-containing oral contraceptive pills or hormonal replacement therapy, and previous history of phlebitis or DVT) should have an injection of LMWH before the endovenous treatment. There is no evidence for prolonged anticoagulation as a prophylatic measure (beyond the day of treatment), but in the high-risk group, self-administration of LMWH can be suggested until the patient is fully mobile. Some surgeons request that female patients stop oestrogen-containing oral contraceptive pills or hormone replacement therapy a month before treatment. There is no evidence in support of this practice, and there is a risk of unwanted pregnancy.
During ultrasound-guided endovenous therapy, the presence of any thrombus in deep veins is easy to recognize and should be treated with appropriate anticoagulation. For total deep vein occlusion, full DVT treatment should be instigated while for partial occlusion of a deep vein, a short course of it may be sufficient.
Air travel of more than four hours duration (especially in high-risk group patients) is generally discouraged for two weeks following RFA treatment, but again evidence is lacking due to the rarity of DVT after ablation. Some surgeons extend this delay to 4–6 weeks. Patients should be advised to reduce their risk by keeping well-hydrated, wearing compression stockings and exercising their calf muscles.
Wound problems and skin burns
Other early complications including wound problems (6–8%) and skin burns (8%) have been reported following RFA.5,7 The incidence of skin burns has reduced since the advent of tumescent anaesthesia from 1.8% to 0.5%. 25 The treated vein may be palpable as a cord; however, this rarely causes significant discomfort, and is poorly reported in studies.
Lignocaine toxicity
The routine use of tumescent anaesthesia in a clinic room setting has now become an established way to treat varicose veins. Tumescent anaesthesia consists of lactated Ringer's or normal saline fluid combined with lidocaine, epinephrine and optionally bicarbonate to form a 0.1% anaesthetic solution (or 1 mg per mL). 11 Tumescent anaesthesia has been found to be very safe in large series, 26 and previous work on tumescent local anaesthetic has shown that used subcutaneously a dose of 35 mg/kg is safe and extremely effective in vein surgery.
In an average 70 kg man this equates to 2450 mL – a substantial safety margin for most endothermal procedures (35mg/kg for 70 kg person = 2450 mg = 2450 mL of 0.1% solution). Despite this, surgeons and phlebologists should be aware of the potential for adverse events due to lidocaine injection. Complications of early or mild toxicity of lidocaine may cause light-headedness, dizziness, tinnitus, confusion and drowsiness. It is important to talk to the patient throughout the procedure and to discontinue injection if suspicious of any of these symptoms arising. Tonic–clonic convulsions leading to progressive loss of consciousness, coma, respiratory depression and arrest are the signs of serious toxicity.
Management of lidocaine toxicity involves standard resuscitation techniques, however patients may require extended resuscitation. 27 Hypoxia needs to be prevented and hypotension and arrhythmias treated. Grand mal convulsions may require treatment with intravenous diazepam. Lipid emulsion therapy has recently emerged as a significant aid in managing toxicity.
Late complications
Skin pigmentation
Skin discolouration or hyperpigmentation may occur following endovenous treatment due to the residual blood trapped within the veins. This normally resolves over a few months. The pooled rate of bruising and skin pigmentation of 19% following RFA has been reported in a meta-analysis. 7 Other studies have reported lower rates of skin staining, between 6% and 9%.3,5 RFA (both VNUS and RFiTT) has been shown to cause less pain and ecchymosis than laser ablation.12,28 The risk of this complication can be lessened by careful application of tumescence and avoiding treating very superficial veins with RFA.
Nerve damage (paraesthesia)
Nerve damage is one of the most common causes of litigation after varicose veins surgery. 29 Paraesthesia or numbness may arise following RFA but in most cases improves over the course of a few weeks.
In a review of case series of patients who underwent RFA, the median rate of paraesthesia has been reported as high as 13%, 30 with other studies reporting it as 4.8–12%.3,5 In the meta-analysis reported by Nesbitt et al., 7 the pooled rate of paraesthesia from three large studies was 20% at three months. Significant reduction in the incidence of paraesthesia has been shown after the introduction of tumescent local anaesthesia to the RFA procedure – from 14.5% to 9.1%. 25 For treatment of the short saphenous vein, a study of laser ablation has shown that mid-calf cannulation may avoid thermal damage to the sural nerve (3% versus 20%, P < 0.05) 31
Recurrence
Patients with late failure of RFA may remain asymptomatic or present with recurrent varicose veins (REVAS). 32 REVAS is a clinical definition that represents true recurrences in addition to residual varicosities and the progression of venous disease. Therefore, the presence or absence of REVAS is dependent not only on efficacy of the treatment to the saphenous trunk but also the management plan for the varicosities. 33 It certainly has an influence on patients34,35 and therefore the concept of REVAS and asymptomatic recurrence should be carefully explained. The management of patient expectations plays a large role in treatment satisfaction. 36
The long-term outcome for RFA has also been assessed in a number of studies. In a meta-analysis, van den Bos et al. 24 have looked into 64 eligible studies comparing laser, RFA, surgery and foam sclerotherapy. They identified that estimated pooled success rates at three years for RFA was 84%. Recent separate one- and three-year follow-up data have shown an absence of reflux in 95.2% at 12 months 3 and 92.6% at 36 months postprocedure. 23
Recanalization of a vein could be due to either reflux from a tributary or an incompetent perforator. Similarly, if the main lumen is patent reflux from the groin due to an accessory vein can also lead to failure and recurrence. 37 Technical problems such as difficult access, problems in advancing the catheter or a tortuous GSV can all play a role in failure of the procedure or incomplete occlusion of the vein ultimately causing recurrence. 37 Neovascularization, though less frequent with RFA than surgery 7 is also considered a cause for REVAS and has been seen in 2.8–7% of cases.15,38 Insufficient energy delivery and too-rapid pullback have been adjudged causes for incomplete obliteration of the vein lumen.9,23 RFA for recurrence has been shown to cause less pain and bruising than surgery as well as taking less time. 39
Discussion
Complication rates associated with radiofrequency ablation of varicose veins
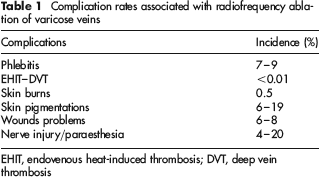
EHIT, endovenous heat-induced thrombosis; DVT, deep vein thrombosis
The routine use of tumescent anaesthesia in a clinic room setting has now become an established and viable way to treat varicose veins.
There are certain points, which need to be carefully addressed during the RFA technique to avoid complications: 37
Adequate vein emptying by leg elevation;
Tumescent anaesthesia should be instilled below the saphenous fascia and above the deep muscular fascia surrounding the vein using ultrasound guidance;
The GSV should be compressed to separate it from the inflow tributaries;
Appropriate use of tumescent anaesthesia and maintenance of an adequate probe temperature are vital to the RFA technique.
The advantages of RFA are far greater than its associated risks. A full explanation of the procedure along with its relevant risks is important in managing patient expectations. With the increased use of endovenous therapy it is likely that the incidence of varicose vein litigation will decrease in step.