
Abstract
Endovascular reconstruction has become the standard treatment of chronic obstruction of large veins. Stenting is done with increasing frequency to treat iliac venous obstructions, with or without associated inferior vena caval or femoral vein occlusions. Open reconstruction with venous bypass is performed today in patients who fail attempts at venous stenting or who are not candidates for endovascular reconstructions. Patients with primary or secondary malignancies invading the vena cava undergo open caval reconstruction at the time of tumour excision. Open venous reconstructions are still preferred in patients with large vein injuries due to blunt or penetrating trauma or in those who suffer iatrogenic venous injuries. Hybrid reconstruction can be performed with endophlebectomy of the common femoral or femoral veins combined with iliofemoral stenting.
Keywords
Introduction
Endovascular reconstruction with balloon angioplasty and stenting has become the standard of treatment in patients who present with symptomatic iliac vein obstruction (May–Thurner syndrome), with or without associated inferior vena caval or femoral vein obstructions. If there is associated acute or subacute thrombosis, it is frequently treated first with pharmacological or pharmacomechanical venous thrombectomy.
Open surgical reconstructions or hybrid repairs for chronic venous obstructions are offered to those symptomatic patients who are not candidates for standard endovascular therapy1,2 For patients with malignant tumours, invading the inferior vena cava (IVC), open resection and reconstruction with polytetrafluoroethylene (PTFE) or, rarely, with autologous graft, may be the only good option.3,4 We reported our experience with open and hybrid reconstructions performed in patients with non-malignant obstruction in the iliofemoral veins and the IVC.5,6 Our group also published on indications, techniques and results of open large vein reconstructions done in patients with malignant disease3,4 and in those with nutcracker syndrome.7,8
Open venous reconstruction
When to do it?
Open reconstruction should be considered in the following conditions:
When chronic venous occlusion cannot be crossed with a guidewire for stenting;
If the iliac vein occlusion is the result of previous trauma or iatrogenic injury that was associated with ligation or clipping of the iliac veins;
When iliac or iliocaval thrombosis is associated with a venous aneurysm;
When endovascular stenting failed;
In patients with hypoplasia or aplasia of the iliac veins;
For patients with malignant tumours, invading the IVC or iliac vein (Figure 1);
Expanded polytetrafluoroethylene (ePTFE) interposition graft implanted following excision of a malignant retroperitoneal tumour invading the infrarenal inferior vena cava
Venous reconstruction for trauma or iatrogenic venous injury, if stenting or stent-grafting is not possible.
When not to do it?
In patients with poor venous inflow due to extensive infrainguinal occlusive disease;
In patients with poor outflow due to extensive venous disease of the iliac vein or IVC;
In patients who are not candidates for anticoagulation;
If a saphenous vein is less than 4 mm in diameter, a Palma procedure should not be done;
When a prosthetic graft has to be anastomosed to the femoral vein and an arteriovenous fistula (AVF) cannot be performed due to associated PAD;
In patients with acute deep vein thrombosis (DVT) open bypass should be avoided if possible;
In poor surgical candidates due to possibility of long anaesthesia time and risk of bleeding.
Hybrid reconstructions
Hybrid reconstruction can be done to improve inflow to the iliofemoral stent with endophlebectomy of the common femoral or femoral vein, closing the vein with saphenous vein or bovine pericardial patch.
When to do it?
The main indication for hybrid procedures, that we first reported on in 2001, 1 is extensive thrombosis of the common femoral vein that prevents primary iliofemoral venous stenting. If these patients have good inflow at least through the profunda femoris vein, a groin incision is performed, the femoral veins and saphenous vein are exposed and endophlebectomy of the chronically occluded common femoral vein is done. The procedure is finished with saphenous vein or bovine pericardial patch angioplasty. Once inflow is assured, iliofemoral stenting is done with standard techniques.
When not to do it?
Poor inflow even to the profunda femoris vein;
If there are other contraindications for stenting and indications for open repair as listed above.
What are the results with open reconstructions and hybrid procedures?
We recently conducted a retrospective review of 60 patients who underwent open or hybrid reconstructions for chronic, non-malignant occlusion of the iliofemoral veins or the IVC between January 1985 and September 2009. 6 Sixty patients (26 men, 34 women, mean age 43 years) underwent 64 procedures. In all, 94% had leg swelling, 90% had venous claudication, 19% had active and 12% had healed ulcers (CEAP [clinical, aetiological, anatomical and pathological elements] classes: C3 = 30, C4 = 12, C5 = 8, C6 = 12). Twenty procedures (31%) followed failed endo vascular treatments.
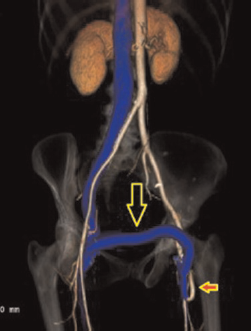
Fifty-two open procedures included 29 femoro-femoral bypass (Palma procedure with saphenous vein: 25, with PTFE: 4) (Figures 2 and 3), 16 femoral-iliac-infrahepatic IVC bypasses (vein: 3, PTFE: 13) and six complex, bifurcated bypasses. Twelve patients had hybrid repairs (femoral endophlebectomy patch angioplasty, venous stents). A femoral AVF was added in 41%.
Postoperative computed tomographic (CT) venogram of a Palma procedure with saphenous vein (arrow) for right iliac vein occlusion that could not be treated with endovascular techniques Expanded polytetrafluoroethylene (ePTFE) Palma graft (large arrow) for left iliac vein occlusion. Small arrow indicates a loop arteriovenous 4–7 mm ePTFE fistula between the graft and the superficial femoral artery
Early results
Early re-occlusions were frequent, it occurred in 17% after open repairs and in 33% after hybrid repairs. However, revision was successful in most patients and discharge patency was 96% after open repairs and 92% after hybrid repairs. There was no mortality, pulmonary embolism or extensive DVT, even when the bypass had early failure. Two patients had haematoma; six had wound complications.
Late results
Five-year primary and secondary patency was 43% (95% confidence interval [CI] 29–56%) and 58% (CI 42–72%), respectively. For Palma vein grafts it was 70% and 78%, for iliofemoral and ilioinfrahepatic IVC bypasses it was 75% and 86%, and for femoral-infrahepatic IVC bypasses it was 44% and 57%, respectively. Complex open reconstructions and hybrid procedures had low, 28% and 30% two-year secondary patency, respectively. Early and late secondary procedures were frequent; they were required in 38 patients.
Factors adversely affecting graft patency included the use of prosthetic grafts, smoking, male gender and, for the Palma procedure, endoscopic vein harvesting. For hybrid repair, extension of the stent into the common femoral vein patch versus proximal to the patch significantly increased secondary patency.
At last follow-up, 60% of the patients had no venous claudication and no or minimal swelling. In all, 85% of patients with patent bypass had no or minimal symptoms compared with only 10% of patients with occluded grafts. All ulcers with patent grafts healed; recurrence was 40% with patent versus 67% with occluded grafts.
In a recent publication, Vogel et al. 9 reported on improved results with hybrid iliofemoral venous reconstructions. Ten patients underwent hybrid repair, two with an arteriovenous fistula. There was one early death, one patient was lost to follow-up and five had more than six months of follow-up. Only one segmental femoral vein occlusion was noted. Four of five patients with longer than six months of follow-up had patent reconstruction; improvement in symptoms and in quality of life could be demonstrated.
Results of open reconstruction for malignancy
In a group of 29 patients who underwent IVC reconstruction with expanded PTFE graft (n = 28) and a panel graft using the femoral vein (n = 1), Bower et al. 3 from our group reported on two deaths within four months of surgery. The mean follow-up was 2.8 years (range, 2.7 months to 6.3 years). Only two late graft occlusions occurred: one at 7.5 months, the other, from tumour recurrence, at 6.3 years. There have been no other late graft-related complications. The authors concluded that vena cava replacement may be performed safely with low graft-related morbidity and good patency in carefully selected patients. Our current technique and recommendations for management of these frequently challenging patients have recently been reported in the Handbook of Venous Disorders. 4
Conclusions
Open surgical reconstructions are the best for obstruction of the iliofemoral veins and the IVC, but only in those patients who are not candidates for venous stents or who failed attempts at venous stenting. These procedures are challenging, with increased early failure rate but good response to early revisions, if needed. The Palma procedure using a vein graft and short iliofemoral or iliocaval PTFE bypasses have the best outcomes with durable symptomatic relief in over two-thirds of the patients. Endoscopic vein harvest, smoking, male gender and prosthetic grafts adversely affect outcome.