
Abstract
Despite the fact that venous thromboembolism (VTE) is one of the most widely studied areas in medicine, and despite the availability of data from numerous RCTs, there are many areas where the evidence is insufficient to allow grade A recommendations to be made. In these areas published guidelines often differ in their advice. In this chapter we primarily discuss the National Institute of Clinical and Health Excellence (NICE) VTE prophylaxis pathways in the context of other guidance published by the Scottish Intercollegiate Guideline Network and the American Colleges of Physicians and Chest Physicians. Evidence for the use of both mechanical and pharmacological thromboprophylaxis is discussed for both medical and surgical patients.
Introduction
A number of respected organizations have published guidance on venous thromboembolic (VTE) prophylaxis pathways in recent years, for example:
The American College of Chest Physicians (ACCP), June 2008; 1
American College of Physicians (ACP), November 2011; 2
Scottish Inter-Collegiate Guideline Network (SIGN), December 2010; 3
National Institute for Health and Clinical Excellence (NICE), January 2010. 4
In this chapter we will examine the VTE prophylaxis pathways published by NICE in 2011 5 with reference to the other publications where guidance differs. 6
It is, of course, well recognized that:
A significant proportion of surgical and medical patients admitted to hospital are at significantly increased risk of VTE as a consequence of innate and acquired factors;
VTE remains a common cause of potentially avoidable morbidity and mortality.
Before setting out specific pathways, most guidelines offer some general advice on reducing these risks as far as possible in a safe and patient-focused manner (Table 1).
General advice on reducing VTE risk (based on NICE pathways)

VTE, venous thromboembolism; HRT, hormone replacement therapy; BMI, body mass index
Maximizing the clinical and cost-effectiveness of VTE prophylaxis pathways, especially perhaps those involving mechanical devices, depends upon informing and engaging with patients. To that end, the choice of VTE prophylaxis should not only depend upon clinical circumstances but also, wherever possible, patient preference. While VTE prophylaxis pathways are based as far as possible upon data derived from large randomized controlled trials, such studies do not cover all types of patient or clinical circumstances, and there are some significant gaps in the ‘level 1’ evidence base. The implementation of prophylaxis pathways therefore needs to take into account patient-specific factors. Where clinicians deviate from evidence-based recommendations (pathways), or where patients decline prophylaxis, the reasons and potential consequences should be documented in the medical records and discussed with the patient.
Many (especially vascular) patients admitted to hospital are already on antiplatelet or anticoagulant therapy. It may be appropriate to offer such patients additional mechanical or pharmacological VTE prophylaxis if the benefits are judged to outweigh the risks. However, such additional measures are not usually advised in those taking vitamin K antagonists (VKAs) and who are within their therapeutic range (providing anticoagulant therapy is continued) or who are having therapeutic doses of low-molecular-weight (LMWH) or unfractionated (UFH) heparin, or fondaparinux.
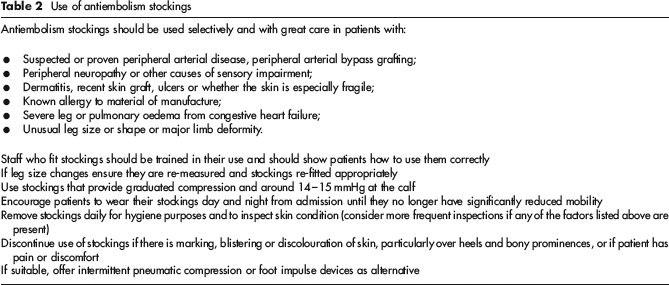
It should perhaps go without saying that the concept of primum non nocere applies to VTE prophylaxis as it does to all other areas of medicine and it is crucial to assess patients on an individual basis when making judgements about how to apply recommended VTE pathways. For example, antiembolism stockings (AES) should be used with particular care in certain patients and circumstances (Table 2).
Use of antiembolism stockings
Medical patients
Medical inpatients (excluding stroke patients)
The NICE VTE prophylaxis pathway for medical (excluding stroke) inpatients is shown in Figure 1. Decisions regarding prophylaxis are based on weighing the risks of thrombosis against those of bleeding within 24 hours of admission and, crucially whenever the clinical situation changes. ACCP, ACP and SIGN guidelines all conclude that there is no evidence that AES improve clinical outcomes and so do not recommend them for routine use.2,4 NICE suggests considering mechanical prophylaxis if the use of pharmacological prophylaxis is contraindicated. Meta-analyses of available studies support the efficacy of pharmacological prophylaxis in reducing the risk of asymptomatic DVT and symptomatic DVT and PE.2,7 A recent Cochrane review presented similar findings.
8
With regard to pharmacological prophylaxis, NICE recommends LMWH, UFH or fondaparinux. Prophylaxis should be continued until the patient is no longer believed to be at increased risk of VTE.
NICE VTE prophylaxis pathway: general medical patients. VTE, venous thromboembolism; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin
Stroke patients
The NICE VTE prophylaxis pathway for stroke patients is shown in Figure 2. A large multicentre randomized trial has shown that AES are ineffective in preventing VTE in stroke patients and that they are associated with an increase in the rate of lower limb skin damage.2,9,10 As such, all current published guidelines suggest that AES should not be offered to patients with stroke.2–4 There remains little published evidence to support the use of pharmacological prophylaxis in acute stroke patients.
2
If a patient has risk factors for VTE, and a haemorrhagic stroke has been excluded, and the risk of bleeding (both haemorrhagic transformation of stroke and other bleeding) is low, NICE recommends LMWH until the acute event is over. If ongoing (24 hourly) assessment indicates the risk of VTE is low, NICE recommends no prophylaxis should be used. If haemorrhagic stroke has not been excluded and/or the risk of bleeding is high, NICE recommend considering either foot impulse or intermittent pneumatic compression devices.
4
NICE VTE prophylaxis pathway: stroke patients. VTE, venous thromboembolism; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin
Orthopaedic surgical patients
Elective joint replacement (hip or knee)
The NICE VTE prophylaxis pathway for orthopaedic patients undergoing joint replacement is shown in Figure 3. NICE recommends that such patients should be offered mechanical prophylaxis and this should be utilized until mobility is no longer significantly reduced.1,3,4 After surgery assuming there are no contraindications, pharmacological prophylaxis should be initiated. There is strong evidence that pharmacological prophylaxis reduces the risk of VTE and fatal PE in patients undergoing hip or knee replacement.1,3,4 A combination of pharmacological and mechanical methods decreased the incidence of DVT and symptomatic PE in a systematic review;
11
although a single randomized controlled trial (RCT) in hip surgery found no benefit of adding AES to fondaparinux.
12
LMWH, fondaparinux, VKAs, rivaroxaban and dabigatran are all effective in preventing DVT
3
LMWH is more effective than UFH and VKA with less bleeding complications.13–15 In total hip replacement (THR) fondaparinux is slightly more effective at reducing DVT but with a trend to more bleeding complications.3,16 Rivaroxaban is more effective in preventing DVT compared with enoxaparin in THR and total knee replacement (TKR) with a similar safety profile.17–19
NICE VTE prophylaxis pathway: elective joint replacement surgery. VTE, venous thromboembolism; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin
Dabigatran is as effective as enoxaparin in reducing VTE in both THR and TKR and is as safe.20,21 Mechanical methods of prophylaxis using AES or intermittent pneumatic compression (IPC) have been found to be effective in reducing DVT risk by a Cochrane review, either alone or in combination. 22 NICE guidelines suggest that pharmacological prophylaxis should be continued for 28–35 days after elective THR, and for 10–14 days after TKR 4 The ACCP guidelines suggest continuing prophylaxis for 35 days for both THR and TKR; SIGN guidelines do not specify the length of extended prophylaxis to be given.1,3 Thus, while the evidence supporting extended prophylaxis following elective THR and TKR is increasingly strong, the optimal duration has yet to be determined.3,23
Hip fracture and other orthopaedic patients
The NICE VTE prophylaxis pathway for patients with hip fracture is shown in Figure 4. Patients admitted with hip fracture should be given mechanical prophylaxis on admission as for elective joint replacement according to NICE guidelines. Provided there are no contraindications, pharmacological VTE prophylaxis should also be given.1,3,4 There are fewer studies of VTE prophylaxis in hip fracture surgery compared with elective joint replacement.
1
Combined mechanical and pharmacological prophylaxis is likely to be most effective but no RCTs directly address this question.
1
A Cochrane systematic review of VTE prophylaxis in patients undergoing hip fracture surgery found that both UFH and LMWH protected against DVT without an increase in bleeding rates.
24
The largest RCT has found that fondaparinux significantly reduced VTE compared with enoxaparin with no increased bleeding.
25
Prolonged prophylaxis with fondaparinux is effective after hip fracture surgery
26
and SIGN Guideline 111 recommends a treatment duration of 28 days.
27
In addition, there is good evidence that if hip fracture surgery is likely to be delayed, VTE prophylaxis should be commenced prior to surgery.
28
NICE VTE prophylaxis pathway: hip fracture and other patients. VTE, venous thromboembolism; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin
Non-orthopaedic surgical patients
The NICE VTE prophylaxis pathways for certain groups of non-orthopaedic surgical patients are shown in Figure 5.
NICE VTE prophylaxis pathway: non-orthopaedic surgery. VTE, venous thromboembolism; LMWH, low-molecular-weight heparin; UFH, unfractionated heparin
Cardiac surgery
Overall, there is little RCT evidence supporting VTE prophylaxis pathways in patients undergoing cardiac surgery. 4 If VTE risk is determined to be increased, mechanical prophylaxis should probably be offered on admission and continued until mobility is no longer significantly reduced. If the risk of major bleeding is assessed to be low, NICE recommends that LMWH should also be given and continued until the patient is mobile (usually 5–7 days). 4 The ACCP and SIGN guidelines recommend similar.1,3 The ACCP guidelines point out that the evidence for routine VTE prophylaxis in these patients is limited; that the overall risk of clinically important VTE is low in this population; and that many cardiac procedures require routine postoperative anticoagulation. 1 LMWH is the anticoagulant of choice, given the higher incidence of heparin-induced thrombocytopenia (HIT) with UFH.
Gastrointestinal surgery
VTE prophylaxis should be offered as for cardiac surgery with the addition of fondaparinux as an alternative to LMWH, in both the NICE and SIGN guidance.3,4 The ACCP guidelines differ with regard to mechanical prophylaxis. They suggest only using mechanical methods of prophylaxis if there are multiple risk factors or if there is a high risk of bleeding contraindicating the use of pharmacological methods, despite citing evidence for their effectiveness. 1 Meta-analyses of RCTs have found that both UFH and LMWH significantly reduce the incidence of asymptomatic DVT, symptomatic DVT and PE, fatal PE and total mortality in surgical patients, but with a significant increase in major (but not fatal) bleeding.29–31 LMWH has comparable efficacy to UFH, but is less likely to cause HIT and is administered only once daily.30,31 One RCT found similar results for fondaparinux. 32 In addition, there is level 1 evidence that AES reduce the rate of DVT in surgical patients, and increase the efficacy of LMWH and UFH.22,33 With regard to extended prophylaxis after hospital discharge, there is good evidence that the peak incidence of postoperative VTE occurs at three weeks. 34 There is little evidence available that confirms the cost-effectiveness of extended prophylaxis, and all of the aforementioned guidelines recommend its use on a case-by-case basis, particularly where there are multiple VTE risk factors present.1,3,4
Bariatric surgery
NICE and SIGN guidelines suggest that all bariatric surgery patients should be offered mechanical prophylaxis at admission and continue until there is a return to premorbid mobility.3,4 In addition, fondaparinux or LMWH should be added until discharge if the risk of major bleeding is low. ACCP guidelines recommend pharmacological prophylaxis for all bariatric patients with or without IPC devices, but not AES, as for high-risk gastrointestinal surgery patients. 1 Only one small RCT of VTE prophylaxis after bariatric surgery has been published, 35 and the evidence either for an increased incidence of VTE in this population or of the effectiveness of prophylaxis remains poor.
Gynaecological, thoracic and urological surgery
NICE VTE prophylaxis recommendations are as for cardiac surgery.3,4 ACCP guidelines differ slightly as for gastrointestinal surgery. They only recommend the use of mechanical methods of prophylaxis where there is a high risk of bleeding, or in patients undergoing major cancer surgery. 1 Extended prophylaxis for 28 days for major cancer surgery in the abdomen or pelvis should be considered on a case-by-case basis.1,3,4 Pharmacological prophylaxis (LMWH or UFH) has been found on systematic review to significantly reduce DVT rates in patients having surgery for gynaecological cancer, 36 but there is limited evidence regarding the preferred duration of treatment in these patients. There are no high-quality trials assessing the effectiveness of methods of mechanical prophylaxis in gynaecological surgery. Thoracic surgery appears to be associated with VTE risks similar to those seen after major gastrointestinal surgery, 1 and in the absence of good-quality evidence of the effectiveness of VTE prophylaxis in this population, the guidelines suggest following the recommendations for gastrointestinal surgery.1,3,4 VTE risks following major urological procedures are considered to be similar to those in gastrointestinal and gynaecological surgery. As there are very few RCTs of VTE prophylaxis in urological surgery, recommendations are often extrapolated from these other groups.1,3,29 Continuation of prophylaxis after hospital discharge has not been evaluated in urological surgery. 1
Neurological (cranial or spinal) surgery
If VTE risk is increased offer mechanical prophylaxis on admission and continue until mobility is no longer significantly reduced. In addition, if the risk of major bleeding is low, LMWH should be given and continued until the patient is mobile (usually 5–7 days).1,3,4 Patients undergoing major neurosurgical procedures are at high risk of VTE. 37 Mechanical prophylaxis is often preferred due to the devastating consequences of postoperative intracranial bleeding. 3 Small RCTs have confirmed the efficacy of AES and IPC in this situation;1,38,39 however, there was no increase in the rate of intracranial bleeding in a meta-analysis of trials using either LMWH or mechanical prophylaxis. 40
Major vascular surgery and other surgery, e.g. high-risk ENT or plastic surgical procedures
Both the NICE and SIGN guidelines suggest the provision of mechanical prophylaxis on admission to these patients with the proviso that an expert opinion is required prior to fitting AES for a patient with peripheral arterial disease (Table 2).3,4 Pharmacological prophylaxis is then given if the risk of major bleeding is low. The ACCP guidelines suggest the use of LMWH or fondaparinux without mechanical prophylaxis, but only in patients undergoing major vascular procedures and who have additional VTE risk factors. 1 A meta-analysis of VTE prophylaxis in aortic surgery has concluded that there is no evidence to support its routine use. 41 There is a lack of evidence available to support the use of VTE prophylaxis in patients undergoing high-risk ENT and plastic surgical procedures. 3
Day surgery
Patients undergoing day surgery should be offered mechanical prophylaxis if they are considered to have an increased VTE risk. In addition, if the risk of major bleeding is low, fondaparinux or LMWH should be added until mobility is no longer significantly reduced, including after discharge.1,3,4
Conclusion
VTE is one of the most widely studied areas of medicine with numerous RCTs generating ‘level 1’ evidence on which ‘grade A’ recommendations can be based. However, generalizing these data to, and implementing the resulting VTE prophylaxis pathways in, an increasingly diverse contemporary cohort of UK patients requires care and thought. For example, there are no RCTs in the morbidly obese, those with known thrombophilia, or in the very elderly. Furthermore, nearly all of the trials are in white (US and European) patients whose propensity to VTE may be quite different from those patients with a different racial and cultural heritage. There are still, therefore, significant gaps in our knowledge. Where only level 2 or 3 evidence is available we are on much less secure ground and it is not therefore surprising that guidelines and pathways can differ. There is clearly an urgent need for further good-quality research in this area.