
Abstract
Iliofemoral DVT constitutes approximately 20–25% of lower limb DVT and represents a specific subgroup of patients at highest risk for post-thrombotic syndrome (PTS). Anticoagulation alone has no significant thrombolytic activity and has not impact on PTS prevention.
Early thrombus removal has reduced PTS in uncontrolled reports and reviews but major trials are awaited. The optimal timing for treatment appear to be thrombus <2 weeks old and, methods for thrombus removal include direct open or suction thrombectomy, catheter directed thrombolysis (CDT), with or without percutaneous mechanical thrombectomy (PMT) devices. Three principle types of PMT device are in use (rotational, rheolytic and ultrasound enhanced devices) and are combined with CDT in pharmocomechanical thrombolysis (PhMT) to enhance early thrombus removal. These devices have individual device specific attributes and side effects that are additional to the bleeding complications of thrombolysis.
A number of additional interventions may be utilised to the improve results of CDT and PhMT. IVC filter deployment to reduce periprocedural PE, is supported by little evidence unless an indication for its use already exists. However, balloon venoplasty and vein stents undoubtedly vein patency after treatment.
Early thrombus removal comes with additional upfront costs derived from devices, imaging and critical care bed usage. However, significant potential savings from reduction in PTS and rethrombosis rates may reduce overall societal costs.
This review focuses on iliofemoral thrombosis, however, the less commonly encountered but clinically important subclavian vein thrombosis is also discussed.
Keywords
Iliofemoral deep vein thrombosis
Introduction
Standard treatment for lower-limb deep vein thrombosis (DVT) is therapeutic anticoagulation (immediate low-molecular-weight or unfractionated heparin overlapping with warfarin for an extended period), limb compression with graduated elastic hosiery and early ambulation. 1 Anticoagulation alone prevents thrombus propagation, reduces life-threatening pulmonary embolism (PE) and reduces the risk of recurrent DVT. This in turn reduces mortality and some of the morbidity associated with venous thromboembolism.
However, anticoagulants have no significant thrombolytic activity and because vein patency is not immediately restored permanent valvular and endothelial damage occurs. This causes distal venous hypertension and dilation that results in incompetence of otherwise normal valves.2–4 The eventual outcome is the unpredictable combination of occlusive and refluxive disease that commonly underlies the soft tissue changes and venous claudication of the post-thrombotic syndrome (PTS), and significantly reduces patients’ quality of life.5–8 Thus, despite optimal medical treatment some 25% of DVT patients develop PTS. Recurrent thrombosis also commonly occurs. 9
Iliac and/or common femoral vein DVT (iliofemoral DVT, Figures 1 and 2) rather than calf, popliteal and thigh vein DVT represent a specific subgroup of patients with the greatest thrombus load who are at highest risk for post-thrombotic morbidity.10–14 Incidences of PTS as high as 27% at six months and 50% after two years are described after iliofemoral DVT.15–17 This recognition has stimulated the use of interventions aimed at achieving early thrombus removal in iliofemoral DVT, with the expectation of reducing acute symptoms and post-thrombotic sequelae.18,19 Early thrombus removal resolves venous obstruction and can restore valve function in the thrombosed segment and prevent late onset valvular incompetence in uninvolved distal veins. This should reduce the incidence of PTS.20–22 Early thrombus removal by open surgery, suction thrombectomy or catheter-directed thrombolysis (CDT) (with or without percutaneous mechanical thrombectomy [PMT]) has been used to treat extensive proximal DVT. One recent trial demonstrated significant reduction in PTS at six months from 27% in controls to 3% after intervention.
15
This article focuses on interventions for thrombus removal with a view to providing guidance on managing proximal lower-limb DVT. Management of subclavian vein thrombosis is also discussed.
Sixty-five-year-old man presenting with right iliofemoral thrombosis rather than the more typical left-sided presentation Thrombosed and enlarged left external iliac vein (white arrow) in a 35-year-old woman presenting with May-Thurner syndrome

Thrombectomy
Direct open surgical thrombectomy (with or without arteriovenous fistula formation) and anticoagulation has advantages compared with anticoagulation alone in promoting valvular and endothelial salvage, improved iliofemoral vein patency and preservation of femoropopliteal valve function. 23 These factors lower ambulatory venous pressures and reduce leg swelling and other symptoms of PTS. However, open thrombectomy for iliofemoral DVT is not routine practice. Significant co-morbidity perceived need for general anaesthesia and the inherent potential for surgical complications are mitigating factors. There is still a role for aggressive surgical thrombectomy in younger, fitter patients with limb-threatening thrombosis.
Aspiration catheter (suction) thrombectomy offers a minimally invasive direct approach to early thrombus removal and can, with selective adjunctive balloon angioplasty/stent placement, achieve successful recanalization. 24 Aspiration thrombectomy has potential safety advantages over open surgery and minimizes the risk of anticoagulation-related haemorrhagic complications. Aspiration thrombectomy may have particular relevance in patients with bleeding or other contraindications to thrombolysis. However, despite its potential, the dearth of good-quality publications suggests technical or outcome limitations with this treatment.
Thrombolytic therapy
Administration of thrombolytic agents that biologically impact on occluding thrombus has become the favoured method for treating proximal DVT. The basic mechanism of thrombolysis is the drug (thrombolytic agent)-induced activation of plasminogen, which is locally bound during thrombus formation, into the active enzyme plasmin that cleaves fibrin within thrombus into its degradation products. Therapeutic venous thrombolysis is supported by experimental observations and offers a non-surgical approach to thrombus removal, improving vein patency and post-thrombotic morbidity. 25 Thrombolysed veins demonstrate reduced residual thrombus load, preservation of endothelial function and retained valve competence compared with placebo.21,26 Although preserved valve function has been observed when early spontaneous clot lysis naturally restores vein patency after clinical DVT, spontaneous lysis is more typically a slow and incomplete process that results in valvular incompetence. 27
Three agents, streptokinase, urokinase and tissue plasminogin activator (TPA), have been used for venous thrombolysis. There are no data comparing one agent with another. However, streptokinase has limitations because of its allergenic properties. TPA and urokinase, both endogenous serine proteinase inhibitors, continue to be used although TPA is gaining prominence as the thrombolytic agent of choice in recent reports.
Systemic thrombolysis
Systemic thrombolytic drug administration provides significant objective longterm benefit compared with anticoagulation alone. 28 Randomized trial evidence, supported by Watson's 2004 Cochrane review, shows significant lysis and reduced post-thrombotic morbidity compared with controls.29–31 However, systemic thrombolysis is limited by circulating plasminogen activator inhibitors (PAI) that neutralize free plasminogin activators thereby achieving relatively modest thrombus clearance at the cost of significant bleeding complications. As a result, systemic thrombolysis is no longer recommended for DVT treatment.
Catheter-directed thrombolysis
Direct intrathrombus delivery of thrombolytic agent achieves local plasminogen activation and (by avoiding circulating PAI and antiplasmins) increases the likelihood of successful thrombolysis (Figures 3a and b).
32
Compared with systemic lysis, CDT improves thrombus removal while reducing drug dosage, treatment duration and bleeding complications, and has become preferred for early thrombus removal.33,34 Various catheter devices have been used to deliver CDT including end delivery, side delivery and pulse spray catheters. However, there are no data comparing one catheter type with another and, therefore, no evidence favouring the use of one catheter type over another for DVT thrombolysis therapy.
Venograms show left common and external iliac veins filled with thrombus (a), after catheter directed thrombolysis (b) and after intravenous stent insertion (c). An inferior vena cava filter (white arrow) was placed in this patient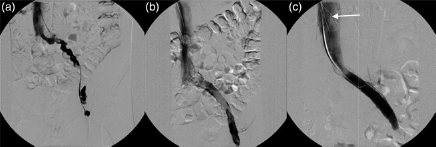
Reviews, registries and non-randomized data support CDT treatment, despite a 4–8% risk of local bleeding complications. The US National Venous Registry has demonstrated complete clot resolution in 65% of patients presenting with first-time iliofemoral DVT35,36 CDT improves the preservation of venous endothelium and valvular function and should reduce the risk of recurrent DVT and PTS.37,38 Achieving complete thrombus removal correlates with thrombus-free survival (primary patency) and improved longterm quality of life compared with veins with residual thrombus. 39 CDT results are further improved by treating venous pathologies such as May-Thurner syndrome and venous webs that are revealed after thrombus lysis.
Despite multiple publications on the subject, evidence of CDT from large controlled trials is nonexistent. In three small randomized controlled trials in the literature comparing CDT and anticoagulation with anticoagulation alone, CDT resulted in improved patency and decreased venous reflux.15,40,41 However, we still do not know for certain whether improved treatment patency translates into freedom from PTS.
Complications of CDT
There are several absolute and relative contraindications to thrombolysis. Allergy to the thrombolytic agent (common with streptokinase) is rarely encountered with TPA. Major bleeding complications tend to result from pre-existing compromise of the body's haemostatic ability and treatment should be avoided in the presence of bleeding diatheses, coagulopathy thrombocytopaenia, renal or hepatic failure or the presence of haemorrhage-prone tissue such as recent myocardial infarction or stroke, recent gastrointestinal bleed, major surgery or trauma, uncontrolled hypertension, metastatic malignancy or pregnancy. Bleeding complications remain the major concern of CDT; however, the majority are minor access site bleeds that can be minimized by using ultrasound-guided cannulation to reduce the likelihood of multiple vein puncture. Significant bleeding complications (haemoglobin drop ≥2 g/dL, transfusion requirement ≥2 units, critical bleed such as intracranial, retroperitoneal or major intestinal bleed) are also relatively rare with registry data suggesting a rate of 1–3%. Incidence of symptomatic PE, another major potential complication, is of the order of 1%; however, fatal PE and death are rare. 42
Who should be offered treatment
CDT is likely to offer the greatest benefit in biologically young and active patients with a long life-expectancy presenting with acute iliofemoral DVT, or any suitable patient presenting with a threatened limb. While the ideal patient should have no underlying malignancy, malignancy per se is not a contraindication to thrombolysis and cancer patients should not be automatically excluded. Comparable outcomes have been achieved in appropriately selected patients despite the presence of cancer. 43 Patients presenting with a history of chronic thrombosis, chronic drug abuse with groin injections, recalcitrant underlying stenotic lesions, previous failed attempts at angioplasty and stent insertion are unlikely to respond to CDT and should be excluded.
The most recent American College of Chest Physicians (ACCP) 2008 Guidelines now recommend CDT in selected patients with extensive acute symptoms (≤14 days), with good functional status and life-expectancy greater than one year who are at low risk of bleeding. 44 This recommendation is supported verbatim by the recently published UK National Institute for Health and Clinical Excellence (NICE) guideline development group draft document on venous thromboembolic diseases. 45
Further recommendations from ACCP include pharmacomechanical thrombolysis (PhMT) (discussed later) in preference to CDT alone where expertise is available and correction of underlying venous lesions using balloon angioplasty and stents.
However, because of the absence of good-quality evidence the ACCP guidelines assign CDT as a grade 2B recommendation, suggesting limitations of certainty of outcome and risks. Surprising, in the light of this absence of good evidence, is the fact that NICE's draft guideline has prioritized CDT in management of iliofemoral DVT.
When to treat
Thrombus age remains critical to the likely success of thrombolytic therapy and thrombus estimated to be less than two weeks old is generally accepted for CDT. Uncontrolled registry data also suggest thrombus less than 10 days old has better outcomes than that over 10 days of age; however, there is no universal consensus on when to treat. 46 Of the three major studies currently being undertaken, the USA ATTRACT trial and Dutch CAVA trial accept thrombus aged up to 14 days. Uniquely, the Norwegian Ca Vent Trial accepts thrombus up to 21 days in age.47–49 A method of extending treatment to non-acute DVT has also been proposed using prolonged low-dose CDT but this requires independent verification in larger studies. 50
The existing uncertainty of an upper thrombus age limit for effective lysis is compounded by the poor reliability of using clinical symptoms to determine thrombus age because new symptomatic thrombus may form on old asymptomatic clot. However, more objective methods of determining thrombus age remain elusive and clinical onset is likely to remain the best indicator for ageing thrombus for the foreseeable future.
Treatment technique
Prepared and consented patients are optimally managed in the interventional radiology suite. Following duplex confirmation of iliofemoral DVT, venous access is obtained by placing a vascular sheath distal to the thrombus, usually into the ipsilateral popliteal vein. Initial venography defines the anatomical distribution and proximal extent of the thrombus and the treatment catheter is advanced into the occluding thrombus. Typically, the thrombus is seeded with TPA (5 mg) followed by continuous slow infusion (1 mg/hour) and interval venograms are performed to assess the progress of clot dissolution. Treatment is continued for up to a maximum of 72 hours as treatment beyond this time risks progressive increase in complications. Heparin (500 U) is co-administered through the sheath during treatment to reduce the risk of pericatheter thrombosis. An increased dose is continued after thrombolysis to counter the tendency for rebound thrombosis. Fibrinogen should be monitored during treatment and levels maintained above 0.15 g/dL to reduce the risk of major bleeding. Activated partial thromboplastin time, platelet count and thrombin levels should also be monitored together with the international normalized ratio.
Classification of technical success of lysis
Although extent of thrombus clearance is a key predictor of early and continued patency there has been no standardization in reporting outcome. The amount of residual mural thrombus can be difficult to determine on venography and duplex imaging. The two-dimensional nature of venography in particular (even when multiplanar views are obtained) tends to underestimate residual disease. Intravenous ultrasound (IVUS) imaging allows more accurate detection of residual thrombus with the added advantage of being capable of detecting external sources of compression. However, IVUS technology is expensive and likely to remain so for the foreseeable future. IVUS is therefore unlikely to enter routine clinical use in a tariff-based publicly funded health system such as the NHS.
Percutaneous mechanical thrombectomy (PMT)
The goal of rapid thrombus removal while minimizing thrombolytic dose and complications has stimulated the development of PMT devices. Current PMT devices have rotational, rheolitic or ultrasound-enhanced mechanisms of action. When used with CDT in pharmacomechanical thrombolysis (PhMT) the treatment combines the benefits of CDT lysis with more aggressive thrombus removal, with the entire treatment being completed in hours rather than days. Some PMT devices have been used without CDT in patients deemed to be at high risk from thrombolysis-related bleeding. 51 However, retrospective reports suggest that PMT alone fails to remove adequate thrombus. 52
PhMT techniques have the same side-effect profile as CDT, although this is minimized by reductions in thrombolytic dosage and treatment times. They also have specific device-related side-effects.
Uncontrolled evidence suggests that PhMT is efficacious and typically improves treatment outcomes and PMT devices have been rapidly adopted into clinical practice in many European and North American centres.53,54 However, they might still be considered evolving (and expensive) technologies, that have limited trial evidence to support their use. Specifically, there are no randomized trials of PMT or PhMT versus CTD alone, no prospective studies and no studies reporting population-level data. 55
Results from the ATTRACT, CAVA and CAVENT trials should provide more objective comparative data to shape the future use of devices for accelerated thrombus removal.47–49 They may also provide guidance on the best indication for specific device types, their relative efficacy and need for adjunctive post-treatment intervention. However, it is their impact on re-thrombosis and PTS that are most eagerly awaited.
Rotational devices
Different types of high-velocity rotational devices effect thrombectomy by macerating thrombus prior to extraction. An example is the Trellis® isolated segmental device (Bacchus Vascular, Santa Clara, CA, USA). This acts by producing high-frequency sinusoidal waves in a nitinol wire that fragments thrombus between two isolating occlusion balloons. Thrombectomy is enhanced by infusing TPA (5–10 mg) into the isolated and fragmented thrombus prior to its removal. In comparison with CDT, rotational devices offer more effective thrombus removal in less time and with reduced doses of thrombolytic agent. They appear to be effective and may increase the proportion of patients offered thrombus removal to include those with bleeding contraindications for CDT. 56 They have also been demonstrated to be safe in terms of major bleeding complications, symptomatic PE, and other significant adverse events. 57 Rotational PMT devices undoubtedly achieve effective thrombus removal; however, their physical mechanism has the potential to cause significant endothelial injury, with an inherent theoretical risk of increasing recurrent thrombosis.
Rheolytic devices
Rheolysis works by power pulse spray injection of thrombolytic agent (TPA 5–10 mg) into the occluded segment followed (15–20 minutes later) by high-pressure saline jet injection to fragment the thrombus. Thrombectomy is completed by a saline jet vacuum that pulls fragmented thrombus into the device catheter where it is pulverized and evacuated. An example is the Angiojet® catheter (Possis Medical, Minneapolis, MN, USA). 58 Rheolytic devices cause less endothelial damage (compared with rotational devices); however, they can cause significant haemolysis and release of intracellular contents (potassium, adenosine and haemoglobin). This can cause bradyarrhythmias, anaemia, haemoglobinuria and renal dysfunction. These serious potential complications are attenuated by reducing rheolytic treatment times. Venographic demonstration of residual thrombus after completion of rheolytic therapy means that thrombolysis invariably has to be continued beyond the immediate rheolytic period. This mitigates some of the proposed advantages of rheolytic PMT over standard CDT Despite this there are reports showing that rheolytic PhMT limits the dose and duration of CDT, and improves success rates. This is associated with shorter hospital and intensive care stay and decreases costs.59,60
Ultrasound-enhanced CDT
Ultrasound energy increases uptake and penetration of thrombolytic agent into thrombus and has produced promising clinical results. Ultrasound-enhanced CDT (UE-CDT) treatment catheters contain multiple transducers (along the treatment tip) delivering an even dose of ultrasound energy radially along the infusion zone. The high-frequency low-energy ultrasound (approximately 2 mHz and 0.45 W) acts on fibrin to disaggregate the fibrin matrix and expose additional plasminogen receptor sites to the thrombolytic agent.61,62 Unlike rotational devices, UE-CDT devices such as the EKOS endowave system (EKOS Corp, Bothell, WA, USA) requires obligatory thrombolysis to achieve their effect. UE-CDT has potential advantages in causing less endothelial damage than rotational devices and less haemolysis than rheolytic devices. However, the absence of any true mechanical action means they have longer treatment times (typically in the region of 20–30 hours), thereby increasing potential risks from thrombolysis. Compared with standard CDT, UE-CDT increases rates of complete lysis and reduces complications.
Adjunctive interventions
Adjunctive interventions may be employed during CDT and PhMT to improve outcome and reduce complications. Prophylactic inferior vena cava (IVC) filters are placed to reduce thrombolysis-associated PE (Figures 3c and 4). Although frequently performed, this practice is controversial because there is no evidence to support its routine use. Specifically, no increase in PE was identified in patients who underwent standard CDT without filter placement in one study.
63
Rotational and rheolytic PhMT devices by physically disturbing the thrombus load may potentially cause more PEs than standard CDT. However, routine use of filters remains unproven even for PhMT devices. As IVC filters have complications such as thrombosis, migration and perforation, they should be employed only where pre-existing indications exist. Indications include patients who develop iliofemoral DVT while on therapeutic anticoagulation and diagnosis of iliofemoral DVT in patients with contraindications to anticoagulation. Evidence of PE on diagnosis of DVT and presence of free-floating thrombus in the IVC are other reported indications. On balance, selective rather than obligatory IVC filter placement appears to be safe and can be recommended for units planning to establish a CDT/PhMT service. When inserted temporary IVC filters should be used and a planned removal policy should be in place.
Balloon dilation of intravenous stents (dark arrow) inserted into left common and external iliac veins. Also shown are an inferior vena cava filter (white arrow) and a body piercing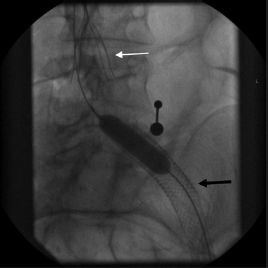
Balloon venoplasty and insertion of large-diameter stents (Figures 3c and 4) are other interventions that improve primary and secondary patency. Uncontrolled case series and registry data suggest that best outcomes follow stenting of underlying venous anomalies such as May-Thurner syndrome or idiopathic lesions, while less favourable outcomes follow treatment in the presence of extrinsic compression or thrombophilia.64,65 There is no controlled evidence upon which strong recommendations on indications for adjunctive stenting can be made. Clinical reality is that sustained success is not universal as stent occlusions and collapse may complicate stent insertion. Future trial evidence should inform on indications for stent insertion and clarify their additional benefit over CDT and balloon angioplasty alone. Currently, stent usage continues to be guided by individual clinical judgement. This mandates vigilant follow-up to assess ongoing patency, to detect stent thrombosis and to allow early salvage manoeuvres to maintain secondary patency. 66 When stents are inserted patients should be maintained on medium term warfarin and antiplatelet therapy should probably be prescribed (Figure 4).
Costs of DVT treatment
Accelerated thrombus removal comes at an additional financial cost to standard anticoagulation therapy. CDT and PhMT are expensive because of costs associated with additional devices, interventional suite use and ongoing in-treatment imaging, angioplasty catheters, venous stents, IVC filters and critical care bed occupancy. These significant upfront costs present a challenge to healthcare purchasers. However, available evidence indicates that thrombus lysis should reduce re-thrombosis and PTS. This should lead to significant reductions in overall societal costs of iliofemoral DVT as follows: there should be indirect savings from improvements in patients’ health and quality of life, and improved productivity, and direct healthcare savings in PTS treatment costs such as leg ulcer management.
Possible barriers to CDT in UK
Iliofemoral DVT mainly presents to nurse-led DVT clinics and busy doctors manning medical admission units who have little or no direct links with local vascular interventional radiology services. Lack of awareness of CDT/PhMT techniques in these settings has meant that iliofemoral DVT tends to be managed to the same protocols as infrainguinal DVT. Overly cautious attitudes to CDT, probably biased by physicians’ experiences from systemic thrombolysis, mean that patients are not often referred for treatment. There may also be a failure of frontline medical clinicians to appreciate the longterm consequences of inadequately managed iliofemoral DVT on post-thrombotic morbidity. Availability of interventional radiology expertise and resources are further barriers in many UK district general hospitals.
Conclusions
The increasing incidence of lower-limb DVT is underpinned by increases in its major risk factors as follows: increase in ageing population, surgical interventions, contraceptive pill usage, long-haul travel and obesity. Incidence of iliofemoral DVT is therefore likely to increase for the foreseeable future. It is vital that major vascular units develop links to local DVT services and agree protocols for an effective strategy for early thrombus removal and definitive treatment of underlying venous pathologies.
Patients presenting with suspected acute iliofemoral DVT should have a thorough clinical assessment and rapid contrast computed tomography from chest to pelvis to define the proximal extent of thrombus, to diagnose co-existent PE, and to detect gross pathology that might underlie the thrombotic process or be a contraindication to thrombolysis.
Immediate anticoagulation, elevation and compression should be commenced; however, vena cava filters should probably be reserved for patients who have free-floating caval thrombus, proven PE or who are already anticoagulated or have a contraindication to anticoagulation. Active patients who have a life-expectancy >1 year should be selected for accelerated thrombus removal by CDT or PhMT where available. Otherwise fit patients who have a strong contraindication to thrombolysis could undergo contemporary venous thrombectomy or segmental mechanical thrombectomy using a rotational device. Identification of any underlying venous stenosis on completion venography should be corrected with venoplasty and stenting as required to provide unobstructed venous drainage from the axial vein to the vena cava. Following successful intervention patients should be maintained on oral anticoagulation (probably with antiplatelet medication when a stent has been placed) for an extended period. The role of the newer factor XA inhibitors in the context of venous thromboembolism has yet to be determined. However, they may challenge the existing anticoagulation pathways in future.
Upper-extremity DVT (subclavian vein thrombosis, Paget-Schroetter syndrome or effort thrombosis)
Introduction
Acute upper-extremity DVT (UEDVT) represents up to 4% of all DVTS. Secondary UEDVT usually has an identifiable cause such as axillary/subclavian vein catheterization, direct trauma or cancer as predisposing factors and will not be considered further. Primary UEDVT differs from lower-limb DVT in its pathophysiology and demographic profile and has a poor association with the usual risk factors for DVT. The aetiology of UEDVT is subclavian vein compression in the narrow space of the thoracic inlet formed by the anterior aspect of the first rib, the medial clavicle and their related musculature, and is triggered by repetitive exercise. Primary UEDVT typically presents in young otherwise healthy individuals, often in association with recent effort (Figure 5a). UEDVT has tended to be more aggressively managed with thrombolysis and surgery compared with iliofemoral DVT. Initial treatment with anticoagulants is usually followed by selective use of thrombolytic therapy. Treatment is then completed by thoracic outlet decompression with the aim of reducing risk of recurrence in these young patients. Despite this seemingly straightforward strategy the management of UEDVT is notable for its many controversies. Areas of variable practice include whether early surgical thoracic outlet decompression should be undertaken after thrombolysis, which surgical approach should be used to optimize decompression, and whether any underlying venous lesion should be treated with percutaneous venoplasty or open surgical repair. More recently, even the necessity of any endovascular intervention (thrombolysis) before surgical decompression has been questioned.
67
Venogram showing axillary/subclavian vein thrombosis in a 20-year-old woman after strenuous skiing holiday (a). Venogram after catheter-directed thrombolysis, anterior first rib resection and direct surgical venolysis, endovenectomy and vein patch angioplasty (b)
Unfortunately, UEDVT management also has a poor evidence base to support the variations in practice. Existing data are limited and derived from uncontrolled small series from enthusiasts. The following are particular areas of controversy following successful thrombolysis.
Venous stents
Upper-extremity venous stents may be deployed for intrinsic venous abnormalities that are revealed after lysis. However, unlike lower-limb DVT, post-thrombolysis subclavian vein stenting without thoracic outlet decompression (and in particular first rib excision) invariably leads to stent fracture and vein occlusion. Stents are therefore contraindicated unless rib resection has been performed. 68 Placement of a subclavian stent remains controversial even when the first rib has been successfully excised because of stresses placed on these stents during normal upper-limb movements. 69
Thoracic outlet decompression
Surgical correction of thoracic outlet anatomy has been an area of historical controversy in UEDVT management. Correction of the compressing aetiology, usually achieved by first rib and local muscle excision, has not been considered an essential part of treatment by all commentators and many have tended to favour a conservative approach.70–72 Advocates of this conservative approach promote a course of longterm anticoagulation, with only selected patients (demonstrating continued symptoms) undergoing delayed rib resection. This results in a 30% reduction in first rib resections. The delay also allows time for resolution of the acute phlebitic process and shrinking of collaterals such that any subsequent surgery is performed in a less hostile environment. Other authors promote surgical intervention during the acute admission, citing increased risks of re-thrombosis, repeat hospital admission and possible loss of previously re-canalized subclavian veins as limitations of the conservative approach. Same admission surgery has been shown to reduce risk of re-thrombosis and has not been associated with any significant increase in perioperative morbidity and mortality.73,74
Surgical approaches to thoracic outlet decompression
There is no definite agreement on the approach taken to achieve effective decompression even among promoters of early surgical intervention. The transaxillary approach has stood the test of time and is the operation most commonly performed in UK centres.75–77 However, because the damaged vein is not easily accessible via this approach, transaxillary decompression is usually followed with adjunctive balloon venoplasty to correct residual venous lesions. The axillary hairline incision offers superior cosmesis, particularly in young women. Also, by avoiding interference with the pectoral girdle, transaxillary resection has been promoted for competitive athletes. However, there is no evidence to support this. Opponents of transaxillary resection highlight poor operative views, limited decompression of the anterior aspect of the first rib and poor access to the subclavian vein as particular limitations. Direct infraclavicular first rib resection is performed using a transverse incision in the medial infraclavicular area and deepened onto the anterior surface of the subclavian vein and the medial aspect of the first rib.74,78 This incision affords complete excision of the subclavius muscle and tendon, the costoclavicular ligament and the anterior portion of the first rib to achieve comprehensive decompression (Figure 6). When required, a paraclavicular approach (supraclavicular and infraclavicular incisions) can be used to access the thrombosed vein from the junction of subclavian and internal jugular vein to the axillary vein.
79
Chest X-ray of patient in Figure 5 showing posterior remnant of first rib (thin arrow) and surgical skin clips (bold arrow)
Percutaneous angioplasty versus surgical venoplasty
Whether the thrombolysed vein, which is never perfectly normal, should be followed by percutaneous balloon venoplasty (the only option after conservative therapy and transaxillary decompression) or by direct open vein reconstruction presents a further area of variable practice. Angioplasty is commonly performed; however, recalcitrant vein stenoses can be particularly resistant to treatment. Cutting balloon angioplasty may be required for effective dilation. 71 Timing of angioplasty is also variable with intraoperative rather than interval angioplasty being advocated to reduce the risk of early re-thrombosis.80,81 Venolysis and direct reconstruction of the diseased vein is a surgical alternative to angioplasty. 79 The infraclavicular approach allows circumferential access to the vein and its surrounding inflammatory covering for complete venolysis and vein reconstruction (Figure 5b). Venoplasty may be achieved by vein patch angioplasty, vein grafts or panel vein grafting as required. Paraclavicular incisions provide full access to the thoracic inlet and allow complete first rib resection (seldom required) and circumferential venolysis from the axillary vein through to the termination of the subclavian vein at the innominate. 82
Conclusion
The established management approach of post-thrombolysis transaxillary first rib resection and selective percutaneous venoplasty is being challenged. Following thrombolysis, infraclavicular first rib excision (including its related musculature and ligaments) together with complete venolysis of the diseased subclavian vein is now being advocated. This approach allows vein repair of any underlying lesions revealed after thrombolysis. This direct surgical correction of underlying venous pathology may lead to more durable results, although this remains to be evidenced. Transaxillary first rib resection with selective venoplasty should be compared with direct infraclavicular rib resection and vein repair in future trials.