
Abstract
Venous thromboembolism is a concern in the paediatric population and its incidence seems to be increasing. Symptoms and signs may be subtle so a high degree of suspicion is needed. Paediatric patients represent a unique challenge in the provision of anticoagulation due to their unique physiology.
Introduction
Venous thromboembolism (VTE) is an important and relatively frequent cause of morbidity and death in adults, both in the community and in the hospital inpatient population. To which end there has been a wealth of guidelines and protocols written to minimize the risk; indeed, the National Institute for Health and Clinical Excellence (NICE) requires that all hospitalized patients over 18 years of age are assessed for their risk of VTE and given appropriate prophylaxis. 1
In the paediatric hospital population, however, this is not the case. Only in the last decade has there has been a growing awareness that VTE is an issue in children and little evidence-based guidance on its prevention and treatment has been published.
Incidence
Historically due to the small numbers involved, there have been few studies examining the incidence of paediatric VTE.
Before 1962, there had been less than 50 cases of pulmonary embolism (PE) in children reported in the world literature. 2 A retrospective review of Scottish inpatients carried out by Jones and McIntyre 3 in 1975 identified 36 cases of venous thrombosis or phlebitis over a four-year period with a further 308 children with deep vein thrombosis (DVT) or PE being reported in the European literature over the subsequent 15 years. 4
Quoted figures derived from epidemiological studies and registry data suggest an incidence of 0.07–0.14 per 10,000 children, or 5.3 per 10,000 hospital admissions of children and 24 per 10,000 admissions to neonatal intensive care units (ICU). These estimates are based on a report from the Canadian Registry of 137 VTE patients between 1990 and 1992, and separate two-year studies of VTE performed in the Netherlands and a neonatal centre in Germany.5–7 A more recent report in 2011 from London found the incidence of paediatric VTE to be much higher, but again this is from a small, specialized paediatric ICU population. 8 Furthermore, Raffini et al. 9 have reported a 70% increase in the diagnosis of VTE over a six-year period in hospitalized paediatric patients across America.
Several theories have been postulated for this increase seen in VTE numbers, one of which is that we are far more aware of such events and so we look for them and thus find them.
It is noteworthy that VTE can occur in association with underlying neoplasms, congenital heart disease, systemic lupus erythematosus, renal failure, infectious diseases, central venous lines or major trauma.
The age distribution of the incidence rate is bimodal, with peaks seen in the neonatal and adolescent periods. 10 It has been proposed that VTE incidence peaks in neonates and infants in part because of their small blood vessel diameter and immature haematological system. Differences have been observed in the concentrations of coagulation cascade components with lower levels of anticoagulant proteins along with reduced fibrinolytic capacity; 11 this in part may reflect that these young patients were receiving treatment in subspecialized departments including paediatric ICU and oncology.
In teenage years, smoking and obesity are contributing factors. The fact that teenage girls have twice the rate of VTE compared with teenage boys has been attributed to pregnancies and the use of oral contraceptive medication. 12
Risk factors
A spontaneous VTE in the paediatric population is relatively unknown and is almost always associated with an underlying disease or risk factor. Both congenital and acquired conditions contribute to the development of thrombosis.
Acquired factors
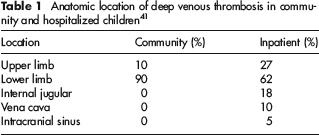
The presence of an indwelling venous catheter is the most significant risk factor for development of VTE in the paediatric population. The introduction of a catheter into a blood vessel can cause thrombosis by directly damaging the vessel endothelium, causing stasis by occluding the vessel or owing to the thrombogenic nature of the catheter material itself. The administration of substances that damage endothelial cells via catheters have also been implicated in thrombus formation in this context.13–15 In children who have developed a VTE, a central venous catheter is thought to trigger >90% of all neonatal venous thrombosis and >50% of all cases in other age groups4,5,8 (Table 1).
Anatomic location of deep venous thrombosis in community and hospitalized children 41
Children with osteomyelitis or meningococcal infections, specifically Staphylococcus aureus, that possess the Panton-Valentine leukocidin gene have been demonstrated to be at increased risk of developing VTE.16,17
Between 9% and 22.6% of children with VTE will have an underlying malignancy. 5 Acute lymphoblastic leukaemia (ALL) appears to be the most common malignancy associated with thrombosis in children. The reported rate of VTE in childhood ALL varies from 1.1% to 36.7%, with an overall average of 3.2%.18,19 Of note, the high rate of 36.7% was observed in the PARKAA trial, but only 1.6% of these documented events were symptomatic. 19
Children with systemic lupus erythematosus (SLE) may develop antiphospholipid antibodies. Montes de Oca, 20 in a Parisian study of 120 children with SLE, found 9% of the cohort developed a thrombotic episode and that half these children had recurrent thrombotic episodes. Furthermore, longitudinal studies observing children diagnosed with SLE demonstrate higher rates of thrombotic episodes, up to 20%. 21
In paediatric trauma patients, there are very few studies on VTE incidence. Of those that have been conducted, Grandas et al. documented three cases of DVT in a review of 2746 paediatric trauma patients. Similarly, Truitt et al. evaluated 3637 paediatric trauma patients and found the overall incidence of VTE to be <0.1%. Overall, there is a low incidence of VTE unless there is an associated risk factor such as prolonged immobilization, prolonged surgery, neurological deficit or central venous catheter use.21–23
Congenital factors
The contribution of congenital thrombophilia to childhood thrombosis remains controversial. In the large majority of available family studies of thrombophilic patients, members younger than 15 years were excluded from the evaluation. 24
The thrombotic risk in otherwise healthy children with a single identified thrombophilic defect appears to be extremely low and is mainly caused by a combination of at least two prothrombotic risk factors; an underlying clinical condition and a triggering risk factor.
The incidence of factor V Leiden is between 0% and 5% in the general population, with the highest prevalence among whites. There is some evidence that factor V Leiden homozygosity is associated with both primary and secondary VTE in children, although this evidence is conflicting. Tormene et al. 26 showed no increase in thrombotic events in either heterozygous or homozygous carriers of the factor V Leiden mutation, which is in contrast to Aschka 27 who reported an increased risk of thrombosis in the newborn and teenagers.
The second most common inherited defect is the prothrombin gene mutation (G20210A). Its prevalence is 2% in the white population and 4–5% in the Mediterranean population. 27 Most children with the prothrombin gene mutation do not develop thrombosis until adult life.25,28
Protein S, protein C or antithrombin III deficiency is clearly associated with an increased risk of thromboembolic events during childhood. 28 Homozygous deficiency in these conditions will often present in the neonatal period.
Defects affecting factor V, prothrombin, protein S, protein C or antithrombin III play a causal role in thrombotic events. Outside extreme circumstances such as cancer, the need for prolonged immobilization, cardiovascular surgery or the insertion of central venous lines, routine screening for thrombophilia before the age of 15 years does not appear to be warranted. Putting together key acquired and congenital risk factors, approximately 95% of cases of VTE in paediatric patients occur in those with cancer, following surgery or trauma, or in the context of congenital heart disease or systemic lupus erythematosus.
longterm outcomes
All-cause mortality for paediatric patients who develop VTE is high at 17% but this probably reflects the underlying conditions suffered. Direct VTE-related mortality is around 1–2%, and this figure has remained consistent in several publications and within registry data. In those children whose deaths were directly attributable to VTE, PE was the most common cause of death, although in a significant proportion of cases a central venous catheter-related DVT was the primary event.4,6,7
Buck et al. reviewed paediatric autopsy findings over a 25-year period and concluded that the risk of a clinically important PE was 25 per 100,000 hospital admissions. Of these, only half had premortem symptoms and the cause of the PE was noted in only 40%. 29
Post-thrombotic syndrome (PTS) is also increasingly recognized in children, but the scale of this problem is ill-defined due to a lack of consistency in reporting and scoring systems. PTS results from damage to deep venous valves in the affected limb, causing venous hypertension with extravasation of red cells, fibrinogen and inflammatory mediators. This presents as pain, swelling, skin pigmentation and, in some cases, ulceration. Depending on the diagnostic criteria used, the incidence of PTS ranges from 12% to 63%.30,31 Unlike adults, however, symptoms are usually mild with few paediatric patients developing venous ulceration. The severity of symptoms does seem to correlate with the degree of clot burden and the vessels involved. 32
Also in contrast to adults, DVT in children can frequently be found in the upper venous system following catheter insertion and no validated systems exist to define and grade PTS of the upper extremities. If DVT and PTS are not considered, signs such as head swelling and visible chest veins may be missed or dismissed.
The cumulative incidence of a first VTE recurrence is 5-18% with one study reporting a rate as high as 21%. Risk of recurrent VTE after a spontaneous first thrombotic event appears to be significantly higher in patients with lupus anticoagulant.31,33 With regards to neonates, there has been no meaningful follow-up study to determine the rate of recurrent VTE.
Diagnosis
The clinical presentation of VTE depends on the location of the thrombus. Most paediatric venous thrombi are catheter-related, and therefore are located in the venous system cannulated by the catheter. Many are asymptomatic so a degree of suspicion is required.
Venography is considered the gold standard for the diagnosis of DVT, but it is rarely used today because it is painful, invasive and peripheral venous access can be difficult to obtain in children. Duplex ultrasound (DUS), invasive venography, computed tomography venography (CTV) and magnetic resonance venography (MRV) can all be used to diagnose venous thrombosis in children or neonates.
DUS imaging is the first modality that should be considered because it is non-invasive, safe, painless, inexpensive, portable and readily available. It is also able to reliably distinguish between acute and chronic thrombus, although the small diameter of a child's blood vessel may make the images difficult to interpret. For suspected central vein thrombosis, DUS is less reliable; in this scenario cross-sectional imaging with CTV or MRV is useful. CTV is also the preferred modality in the investigation of suspected PE as it is less invasive than conventional venography, relatively quicker, and more accurate, although CT has not been validated in children. 34
Treatment
Anticoagulation is the mainstay of therapy for VTE in children. An intravenous unfractionated heparin (UFH) is the most common agent used in the initial period as it is readily available and has a short half-life. UFH is a heterogeneous glycosaminoglycan with a molecular weight ranging from 3000 to 30,000 kDa. UFH was initially isolated from the livers of pigs and dogs, but now the majority of commercial UFH preparations currently available are isolated from porcine intestinal mucosa or bovine lung. 35
Neonates have an impaired ability to synthesize thrombin, and typically possess plasma levels of thrombin similar to that of an adult receiving therapeutic doses of heparin. Adolescent paediatric patients typically possess approximately 25% less thrombin than adults. The presence of decreased antithrombin in these patients conveys intrinsic resistance to the effects of heparin. 36 Few trials of UFH dosing have been conducted in paediatric populations. The majority of evidence available is based upon a handful of cohort studies. Monitoring of UFH is necessary due to its relatively narrow therapeutic window and an activated partial thromboplastin time of 1.5–2.5 times normal values should be aimed for. 37
Low-molecular-weight heparins (LMWH) are prepared by altering UFH chains to isolate the region containing the sequence required for binding to antithrombin. Their anticoagulant effect is actioned by potentiating the antithrombin-mediated inhibitor of factor X. LMWH are increasingly being used because they experience less competitive plasma binding and their pharmacokinetics are more predictable than UFH, eliciting a more predictable anticoagulant response, so monitoring is not needed. LMWH have a longer half-life and reduced reversibility compared with UFH, so are best used when prompt reversal is unlikely to be required. Further advantages of LMWH include that venous cannulation is not required, and the risk of heparin-induced thrombocytopaenia and osteoporosis is decreased. 38
Once therapeutic anticoagulation has been established, oral anticoagulation is usually commenced for longer-term therapy. This is done using vitamin K antagonists, including warfarin, phenprocoumon and acenocoumarol. Vitamin K antagonists exert their action by inhibiting vitamin K epoxide reductase, thus reducing the amount of vitamin K available to synthesize the vitamin Independent clotting factors. 39 Factor VII has the shortest half-life of all the vitamin K-dependent clotting factors, hence is the first factor affected. Factor II (prothrombin) has a much longer half-life and levels of factor II do not decrease until days 5–6 of therapy. 39 Reduced levels of factor VII are not thought to be as significant as low factor II levels in producing an anticoagulant effect, hence full anticoagulation is often not achieved until days 5–6 of therapy.
Regular blood monitoring of adults and children receiving warfarin is imperative and children receiving warfarin may require more frequent monitoring than their adult counterparts due to the complexity of their underlying medical condition. The effect of warfarin therapy is measured by the international normalized ratio which compares a patient's prothrombin time against that of a control. Breast-fed infants are particularly sensitive to oral anticoagulants as they ingest low concentrations of vitamin K in breast milk, thus the effects of vitamin K synthesis blockade is more profound, so extra care needs to be taken.
Major bleeding from anticoagulation therapy is rare. Minor bleeding complications occur but can be managed with optimal supportive care. Paediatric patients with uncomplicated venous thrombosis are usually treated for 3–6 months. If inflammatory markers remain persistently raised, a central catheter needs to remain in situ or if there is recurrent thrombosis then anticoagulation may need to be continued for the longer term.