
Abstract
Pregnant women are at an increased risk of venous thromboembolism (VTE) and the consequences of an acute event in pregnancy can be debilitating, long-lasting or fatal. Screening for risk factors early in pregnancy and the provision of thromboprophylaxis are useful ways of preventing VTE in some women, but even when performed diligently, acute events are likely to remain common for the foreseeable future. It is therefore important for obstetric and non-obstetric clinicians to recognize the symptoms and signs of deep vein thrombosis and pulmonary embolism in pregnancy, to understand how a diagnosis can be reached in an effective yet safe manner and to be aware of the available treatment modalities.
Physiological changes in pregnancy and the extent of the clinical problem
One of the leading worldwide causes of maternal death is haemorrhage from the placental bed. 1 As a physiological response to this threat, a woman's blood clotting cascade is potentiated very soon after conception, with increases in circulating levels of fibrinogen and factors VII, VIII, X and XII being detectable early in the first trimester. Adding to this effect, there is a reduction in sensitivity to activated protein C in pregnancy and a fall in functional protein S levels, which usually hold the clotting cascade in check, while the thrombolytic effects of the plasminogen activator inhibitors are also reduced.2–4 Life-threatening haemorrhage from the placental bed most commonly arises in the first few hours after a woman has given birth, so it is of little surprise to find that the physiological pro-thrombotic drive of pregnancy remains pronounced over the same time course, whether measured by circulating levels of individual blood clotting factors or by global measures of coagulation during thromboelastography.2,5
One result of these physiological adaptations is that women have an increased risk of developing venous thromboembolism (VTE) during pregnancy and the puerperium. Specifically, the risk of VTE in the antenatal period is around 0.34–0.66 per 1000 women, consisting mainly of lower limb or pelvic deep venous thromboses (DVT). 6 Around 14% of these can be expected to result in pulmonary embolism (PE). 6 Clinical evidence also confirms that a pregnant woman's risk of VTE further increases immediately after the birth of the baby. In one large population-based case control study from the Netherlands, a sixty-fold increase in the risk of VTE was detected in the puerperium compared with non-pregnant controls. This correlates well with the clinical experience in the UK, which points to the puerperium as being a time of particular risk.7,8
Morbidity and mortality
The longterm morbidity associated with VTE during pregnancy and the puerperium may be greater than that experienced in the non-pregnant population. Mild to moderate symptoms of chronic venous insufficiency such as pain and the formation of varicose veins, dependent oedema or lower limb eczema arise in as many as 75% of people who have suffered a lower limb venous thrombosis. 9 More prolonged and severe symptoms may be encountered in women after a pregnancy-related event, however, possibly because of endocrine-driven peripheral vascular dilation or physical obstruction to venous flow in the pelvis and lower limbs, which persist even after resolution of the original clot. 10
Pregnancy-associated thromboses most commonly arise in ileofemoral veins, particularly on the left-hand side, possibly because of the close proximity of these vessels to the gravid uterus. 11 This is in contrast to the more common popliteofemoral location of thromboses in the non-pregnant population. The more proximal location of thromboses in pregnancy may be the reason that pregnant women are particularly susceptible to embolism. Indeed PE has been established as one of the leading causes of maternal death in the UK for more than 30 years – current figures show that for every 100,000 women who become pregnant, 0.79 will die of a PE in pregnancy or the puerperium. 12
Since pregnant women are particularly susceptible to VTE and since the risks of significant longterm morbidity and mortality are high in this population, it is important for obstetric and non-obstetric clinicians to recognize the common symptoms and signs of the disease. In addition, the diagnostic tools and therapeutic manoeuvres employed must be adjusted to account for the physical and physiological changes that accompany pregnancy.
Risk factors for VTE
The Confidential Enquiries into Maternal Deaths, more recently packaged as a Department of Health publication called Saving Mothers’ Lives, is a form of clinical audit which has been published as a triennial report since 1957. 13 It gives details of all maternal deaths, formerly in England and Wales but more recently across the whole of the UK. In the most recent report, it was found that 89% of women who died from a PE in the UK between 2006 and 2008 had at least one identifiable risk factor. 12
While the Confidential Enquiries focus on maternal mortality, a more recent venture called the UK Obstetric Surveillance System (UKOSS) was instigated as a means of recording the incidence, management and outcomes of a series of serious but rare obstetric morbidities which did not necessarily result in maternal death. 14 In 2008, UKOSS presented case-controlled data detailing the care received by 143 women who had suffered a fatal or non-fatal PE in pregnancy. 15 In common with the Confidential Enquiries data, around 70% of women in the UKOSS study had readily identifiable risk factors for VTE, including multiparity (adjusted odds ratio 4.03 [95% CI 1.60–9.84]) and obesity with a body mass index (BMI) ≥ 30 kg/m2 (adjusted odds ratio 2.65 [95% CI 1.09–6.45]). Table 1 provides detail of some of the most frequently encountered clinical risk factors for VTE in pregnancy and the puerperium, together with their adjusted odds ratios. 16
Clinical risk factors for VTE in pregnancy and the Puerperium 16

VTE, venous thromboembolism; BMI, body mass index
On the basis that VTE in pregnancy could be preventable in some cases, the Royal College of Obstetricians and Gynaecologists (RCOG) has recommended that risk assessment for VTE should be performed for all pregnant women either before pregnancy or more commonly, at their first antenatal ‘booking’ appointment. 16 This assessment may be carried out by a midwife, general practitioner or hospital doctor, using the scheme detailed in Table 2 for risk stratification. In addition, however, the RCOG recommends that the highest risk women should be referred for personal review by a Trust-nominated Obstetric Haematology team. Women in this category include those with recurrent VTEs and those with a single previous VTE plus a family history of VTE or a known thrombophilic abnormality.
RCOG risk assessment for venous thromboembolism 16

Consider antenatal LMWH thromboprophylaxis for outpatients if score is ≥3
Consider postnatal LMWH thromboprophylaxis for six weeks for outpatients if score is ≥2
Consider antenatal and postnatal LMWH thromboprophylaxis for inpatients if score is ≥2
If the woman has an increased bleeding risk, discuss the case with a haematologist
VTE, venous thromboembolism; BMI, body mass index
Interestingly, while the more widespread use of thromboprophylactic agents in pregnancy may already be preventing many pregnancy-related VTEs, careful analysis of the UKOSS report suggests that even a strict adherence to current RCOG guidelines will have only a limited additional impact on reducing the incidence of acute pregnancy-related PEs. 15 It is therefore imperative that obstetric and non-obstetric clinicians remain vigilant for the condition and become familiar with appropriate diagnostic and treatment modalities.
Hospitalization in pregnancy
People hospitalized because of medical or surgical illnesses are at an increased risk of developing VTE. Being pregnant at the time of hospitalization compounds any other existing risk and this is reflected in the appearance of ‘pregnancy’ as a risk factor in current CQUIN-driven VTE assessments in hospitals. 17 CQUIN VTE risk assessments are of very limited clinical value, however, in women admitted to hospital due to an obstetric disease because of their generic, non-obstetric nature. An alternative approach to assessing the VTE risk of women admitted to antenatal or postnatal wards is provided by the RCOG VTE risk assessment tool (Table 2), 16 which lists the key risk factors likely to be found in this population and highlights the need for thromboprophylaxis in the highest risk groups. The individual elements presented in this table could be debated, but the pregnancy-specific approach to VTE risk assessment for hospitalized patients is nevertheless sound in principle.
Thromboprophylactic agents
Low-molecular-weight heparins (LMWHs) are considered to be safe to use in the antenatal period because they do not gain access to the fetal circulation by crossing the placenta, while their maternal safety profile is excellent. Although poor injection technique can lead to localized bruising, clinically significant maternal side-effects such as anaphylaxis, heparin-induced thrombocytopenia (HIT) and osteoporosis are rare. 18
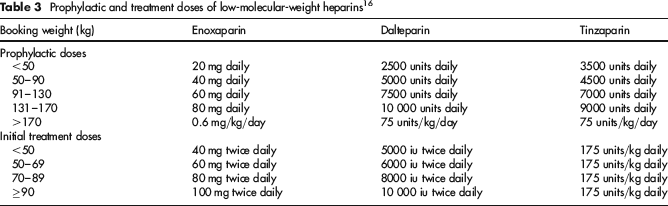
Current recommendations for LMWH prophylactic dosages are presented in Table 3. These are generally given once-daily but for women over 90 kg at booking, splitting the medication and giving it as two separate injections 12 hours apart may be worthwhile. 16 It is also sometimes necessary to use a slightly elevated or even a full anticoagulant dose of LMWH for women who are at an especially high risk of VTE in pregnancy, rather than a standard prophylactic dose. This strategy can be considered in the presence of antithrombin deficiency, some prosthetic heart valves, or if a woman has had a previous VTE while taking normal dose LMWH prophylaxis. In these circumstances, the advice of a haematologist who is experienced in providing care to pregnant women should always be sought.
Prophylactic and treatment doses of low-molecular-weight heparins 16
Diagnosis of an acute deep venous thrombosis in pregnancy
The symptoms of a DVT in pregnancy may include pain in either the leg or the lower abdomen, most commonly in the left iliac fossa. Physical signs may include discolouration and swelling of the leg on the affected side. These symptoms and signs are not universal, though, and conversely, they may be present as normal phenomena of pregnancy. Furthermore, although D-dimer testing is useful in the non-pregnant population, it is of little use in pregnancy. Results are usually elevated beyond the normal non-pregnant range and the test will often therefore give a false sense of concern. 19 Therefore, when a DVT is suspected in a pregnant woman on clinical grounds, anticoagulation should be started without delay according to the LMWH dosage scheme set out in Table 3, then the diagnosis confirmed or refuted by objective testing.
Initially, a compression duplex ultrasound scan should be requested on the suspect limb, 20 with consideration being given to bilateral scanning if the symptoms or signs are ill-defined. If the level of clinical suspicion remains high despite a negative ultrasound scan, full anticoagulation should be continued and the test repeated one week later, beyond which time, discontinuation of the therapy can be considered. Continued outpatient surveillance in the following weeks is, however, advisable if the woman's presenting complaints remain unchanged. Lower limb and pelvic venography are rarely now performed in pregnancy.
Current guidelines suggest that as a good practice point, full blood count, coagulation screen, urea and electrolytes and liver function tests should be taken before anticoagulation is commenced. 21 This recommendation is based upon the concern that women with other pre-existing unidentified pathologies could be adversely affected by high doses of LMWH.
Diagnosis of an acute pulmonary embolism in pregnancy
In common with DVT, the clinical symptoms and signs of PE such as shortness of breath, chest pain and chest wall tenderness may be present as normal phenomena in pregnancy. Again, D-dimers are of little diagnostic use and may be misleading. Current recommendations, therefore, are to perform a full blood count, clotting screen, urea and electrolytes, liver function tests and ECG when there is a high index of clinical suspicion. 21 Arterial blood gas analysis may also usefully be performed, then LMWH commenced at a therapeutic dose while diagnostic tests are organized.
As an initial step, bilateral compression duplex ultrasound scans should be performed in an attempt to identify an iliofemoral thrombosis. In the presence of a positive result and symptoms or signs of PE, the diagnosis can be assumed without recourse to chest imaging.
22
If no iliofemoral thrombosis is identified, however, chest imaging should be offered. An algorithm for diagnosis of a PE in pregnancy is presented in Figure la and b. In this example, perfusion (Q) scanning is included. Some clinicians prefer to employ combined ventilation/perfusion (V/Q) scanning while others prefer to bypass this test completely, since computed tomography pulmonary angiography (CTPA) is less likely to give an equivocal result, at least in the non-pregnant population.
23
(a,b) Algorithm for the diagnosis of pulmonary embolism in pregnancy
As a key issue, it should be remembered that at each stage, a pregnant woman must be informed of the risks and benefits of investigations to her own health and to the health of her unborn baby. A V/Q scan imparts little risk to the pregnant woman but after V/Q scanning in pregnancy, the offspring's risk of fatal childhood malignancy rises from 1:1,000,000 to around 1:280,000. 24 This risk can be reduced by omitting the ventilation phase of this investigation. By way of comparison, CTPA imparts an increased risk of breast cancer to a woman, which may be in the region of 13.6% from a baseline risk of 1:200, 25 although some authors have suggested that this figure is an overestimate. 26 It is accepted, however, that radiation exposure to the fetus is minimal during a CTPA. Concerns have nevertheless been raised about possible fetal thyroid damage from the use of iodinated contrast media during CTPA, so in these circumstances, surveillance of the neonate's thyroid function may be required. 27
Thrombophilia testing in the acute phase of VTE
Knowledge of a woman's inherited and acquired thrombophilia status is rarely helpful when dealing with a possible acute VTE in pregnancy or the puerperium. Neither the need for investigations nor the optimal form of treatment for a confirmed lesion is usually altered. In addition, thrombophilia screening results are difficult to interpret in pregnancy, because of the physiological changes to the clotting cascade previously detailed. If thrombophilia testing is arranged despite these drawbacks, the results should be interpreted by a haematologist experienced in managing pregnant women with thromboses.
More usefully, if a woman has suffered an acute VTE in pregnancy or the puerperium, her thrombophilia status should be checked at least six weeks after she has given birth and several weeks after she has stopped taking anticoagulant medications, which in practice, usually leads to testing 3–4 months after the baby has been born. The results will then be useful in determining the woman's likelihood of recurrence of the disease, particularly in any future pregnancy or when she is exposed to additional pregnancy-unrelated thrombotic risks.
Treatment with low-molecular-weight heparin
LMWH are the anticoagulants of choice for the treatment of an acute VTE in pregnancy and they are also favoured by many clinicians in the Puerperium. They compare favourably to unfractionated heparin in terms of efficacy while there is a reduced risk of obstetric haemorrhage, HIT and heparin-induced osteoporosis compared with unfractionated heparin, even when high doses are used for a pro-longed period of time.18,28,29 There are no fetal concerns with its use since placental passage is negligible and it poses no risk to the neonate during breastfeeding. 30
When an acute VTE is suspected, treatment with LMWH should be started at a full therapeutic dose, according to the scheme detailed in Table 3. Enoxaparin and dalteparin require twice-daily injections. 21 Tinzaparin can be given once-daily although women over 90 kg in weight may benefit from a twice-daily regimen instead. 31 Doses are usually calculated on the basis of the woman's booking weight.
It is generally considered that there is no benefit gained by monitoring plasma anti Xa levels since no clear therapeutic benefit has been shown for the practice and since the accuracy of the test has been questioned, but clinical practice is variable in this respect. 32 Some haematologists prefer to document the peak anti Xa level three hours post-dose, approximately one week after treatment has started, particularly in obese women, in women with previous recurrent VTEs and in women with nephrosis. In these cases, anti Xa levels between 0.5 and 1.2 IU/mL give reassurance. The routine monitoring of platelet counts is not now recommended. 33
Treatment with warfarin
The use of warfarin is uncommon in pregnancy because it readily gains access to the fetal circulation by passage across the placenta. Its use in the first trimester is associated with development of the ‘warfarin syndrome’ in around 10% of cases. In the second trimester, it may cause recurrent intracranial micro-haemorrhages, leading to subtle longterm neurological effects. 34 In the third trimester, the concerns of a major intracranial bleed and placental abruption arise. 35 In rare cases requiring warfarin therapy rather than use of a LMWH during pregnancy, the advice of a haematologist experienced in caring for pregnant women is mandatory.
In contrast, after the birth of the baby, warfarin has a good safety profile. Treatment is usually commenced two to three days postpartum but beyond that time, warfarin is not associated with a significantly increased risk of obstetric haemorrhage and, in addition, little of the drug is found in breast milk so adverse neonatal effects have not been recorded clinically. 36 Warfarin may be of particular use when prolonged postnatal anticoagulation is planned, for example, when a woman has suffered an acute VTE towards the end of her pregnancy.
Relative contraindications to anticoagulants in pregnancy and the Puerperium
Although antepartum haemorrhage is a risk factor for VTE, it also poses a direct threat to the life of a woman and her developing baby. Similarly, postpartum haemorrhage can lead to exsanguination in the most extreme cases. 1 For these reasons, caution must be employed when the use of an anticoagulant is being considered in anyone with risk factors for obstetric haemorrhage. In general, women who are experiencing active bleeding during pregnancy or the puerperium should not be given LMWH or warfarin. In addition, omission of the medication should be considered for women with placenta praevia, placenta accreta, a known bleeding diathesis, or likely need for delivery of the baby in the following 12 hours. 16 If either LMWH or warfarin are being considered in such circumstances, it is imperative that decision-making team includes the services of an experienced haematologist.
Duration of treatment
After an acute VTE in pregnancy, treatment with LMWH is normally continued until the birth of the baby and for at least six weeks afterwards, although warfarin can be used as an alternative postnatal medication. 21 In addition, the total duration of anticoagulation should be at least three months, so women diagnosed at the end of their pregnancy or after the birth of their baby will face a longer period of postnatal anticoagulation than others. 37 This prolonged anticoagulation period is based on the principle that the physiological changes of pregnancy render women at an increased risk of recurrence of VTE if the level of anticoagulation is reduced too early. The clinically optimal duration for full anticoagulation, however, has not been investigated in a formal manner.
Management during induction of labour and in established labour
Few women have their acute VTE diagnosed as an intrapartum event, possibly because labour spans only a number of hours rather than days or weeks, or possibly because the symptoms and signs of an acute VTE are masked by the symptoms and signs of labour. A more common problem facing clinicians is the consideration of how to manage a woman's spontaneous labour, induction of labour or elective caesarean section if therapeutic LMWH has been commenced antenatally.
Management options should be based upon the principle that high circulating levels of LMWH increase the risks of haemorrhage at the placental bed during labour and immediately after the birth of the baby. In addition, high circulating levels of LMWH preclude the use of regional (epidural or spinal) anaesthetic. 38 Therefore, ideally, LMWH administration should cease around 24 hours before either labour or elective caesarean section. This is relatively easy to achieve for an elective caesarean section, but when a vaginal birth is being planned, induction at around 39 weeks’ gestation will prevent most women from labouring in an anticoagulated state, reducing their risk of haemorrhage and maintaining their full range of options for analgesia and anaesthesia. Resumption of anticoagulation at a prophylactic dose is usually recommended around four hours after the birth of the baby, with a return to full therapeutic doses within the following 12 hours. 21