
Abstract
The objective of this study was to review a single center's experience of upper limb revascularization over 20 years.
All patients undergoing operative or endovascular upper limb revascularization between June 1983 and July 2003 were identified.
One hundred eighty-four upper limb revascularization procedures were carried out on 172 patients. Sixty-one patients had a thromboembolic event (35%), 53 patients presented with a traumatic vascular injury (31%), and 29 patients had symptoms of chronic atherosclerotic upper limb ischemia (17%). Fifteen patients had subclavian steal syndrome, eight patients had thoracic outlet compression, and six patients had iatrogenic injuries of the upper limb arteries.
Fifty-five thromboembolectomies were performed, 37 under locoregional anesthesia. Ten patients (18.2%) died from cardiopulmonary causes following embolectomy.
Fifteen reversed saphenous vein bypass grafts were performed for traumatic damage. Twenty-seven patients had a primary repair, and five required a vein patch. One patient subsequently had an arm amputation, and two patients died.
Twelve patients presenting with chronic arm ischemia had a subclavian angioplasty, 12 patients had a proximal bypass, and in 5 patients, stenoses were stented. The mortality in this group was 6.9% (2 of 29).
The mortality for upper limb revascularization was 8.7%. Almost all deaths occurred after upper limb embolectomy, and the mortality of this procedure was similar to that of lower limb embolectomy. Deaths were the result of cardiac comorbidity, and this should be actively sought and treated if outcomes are to improve.
Keywords
Acute or chronic upper limb ischemia is an uncommon condition 1–3 that is responsible for between 15 and 18% of the procedures undertaken for critically ischemic limbs. 4,5 Thromboembolic disease, 1,6–11 vascular trauma, 3,12–15 and iatrogenic injury 16,17 are well recognized as common causes of acute upper limb ischemia. Subclavian artery atherosclerosis and thoracic outlet obstruction often present with chronic arm ischemia. 18 Iatrogenic or vascular injuries may also present with delayed symptoms of chronic arm ischemia. 16,17,19
Most patients with acute arm ischemia require urgent revascularization, but some selected cases can be managed successfully by an endovascular approach. 20 Angioplasty, with or without stent placement, and thrombolysis are being increasingly used for symptomatic chronic upper limb ischemia. 21 Previous publications suggest that conservative management of patients with acute arm ischemia results in functional limb impairment in up to three-quarters of patients managed in this way and is therefore not advocated. 9,22
Surgical techniques that are commonly employed for revascularization of the upper limb include thromboembolectomy, primary arterial repair with or without patch angioplasty, and autologous or venous bypass grafting. 2 These may occasionally be combined with concomitant cervical sympathectomy or cervical rib excision. In contrast, lower limb revascularization is a common procedure, with large numbers of published series of outcome following acute and chronic ischemia. 23–28
The purpose of this study was to review a single center's experience of acute and chronic upper limb revascularization over a 20-year period. The outcome of surgical and endovascular intervention is presented and compared with published series of upper and lower limb revascularization.
Methods
Patients undergoing upper limb revascularization procedures by the vascular team at Guy's and St. Thomas' Hospital between June 1983 and July 2003 were identified from prospectively maintained handwritten or computerized operating room and interventional radiology databases. Further data were obtained from patient case notes, the hospital mortality register, and the Trust's electronic databases and by telephone inquiry to the patient's general practitioner.
Patients were excluded if they had disease of the aortic arch or lesions below the proximal border of pronator teres (n = 89). Patients with occluded arteriovenous fistulae were also excluded. Fourteen patients who had been treated by isolated cervical rib resection or cervical sympathectomy were identified from the database but were not included in the analysis of the data. It was not possible to identify patients who were treated conservatively with anticoagulation over the same time period from these databases.
All of the prospective data was stored in a Microsoft Access 97 database and was retrospectively analyzed.
Results
One hundred seventy-two patients underwent 184 procedures over a 20-year period (Table 1). Acute arm ischemia was responsible for over two-thirds of upper limb revascularization procedures. The majority of patients presented with thromboembolic disease (35%) or acute traumatic arterial injury (31%). Two patients presented acutely following iatrogenic injury.
Case Mix of Patients Undergoing Upper Limb Revascularization
*Percentage mortality for surgical embolectomy.
More than half of the patients with chronic arm ischemia had an intrinsic atherosclerotic stenosis or occlusion of the subclavian or axillary arteries. Fifteen patients had symptoms consistent with subclavian steal syndrome, and eight patients presented with thoracic outlet obstruction. A further four patients with chronic arm ischemia had a delayed presentation following iatrogenic injury.
Thromboembolism
Thromboembolism was the single largest etiologic factor causing arm ischemia in this study (Table 2). Sixty-one patients with a mean age of 72.4 years underwent 68 procedures for thromboembolic disease. Sixty-two percent of the patients who presented with thromboembolic disease had associated atrial fibrillation. Seventeen patients underwent transthoracic or transesophageal echocardiography, but only three patients had detectable cardiac abnormalities. One patient had a mural thrombus, one patient had apical dyskinesia following an acute myocardial infarction, and one patient had both an atrial septal aneurysm and a large thrombus evident in the thoracic aorta.
Procedures Performed for Upper Limb Thromboembolisms (n = 61)
The brachial artery was the site of embolus in 52 patients (85%). In six patients, the embolus had become wedged in the axillary artery, and in three patients, the subclavian artery was occluded. Fifty patients had a primary thromboembolectomy, three patients had an embolectomy combined with a fasciotomy, and another two patients required a repeat embolectomy. Two-thirds of embolectomies were completed under locoregional anesthesia. Three patients had subclavian artery thrombolysis, one underwent brachial artery stenting, and two had axillary artery angioplasties. One patient developed a thrombosis following unsuccessful axillary angioplasty and underwent an operative thromboembolectomy.
Six patients required reexploration, four of whom had presented more than 16 hours after the onset of symptoms. Two patients required repeat embolectomies, and one patient required a fasciotomy for compartment syndrome. This patient subsequently died. No patients required primary or secondary amputation in this group. The 30-day mortality in the patients undergoing thromboembolectomy was 18.2% (n = 10). All of these deaths were attributable to cardiopulmonary causes, none being a consequence of arm ischemia or gangrene. Postmortem examinations to confirm the cause of death were performed in six of these patients. A greater proportion of these deaths occurred in those patients who required a general anesthetic (5 of 18) than in those patients who had the thromboembolectomy under local anesthetic (5 of 37), but this was not statistically significant. A further 11 patients had died within a year of surgery, leading to a 12-month mortality rate of 38.2% (n = 21). The median follow-up in this group was 9 months (0–17 months). Patients underwent clinical and duplex ultrasonographic assessment of their upper limb arterial supply at their postoperative visits. No patients had evidence of an arterial occlusion. The majority of patients were discharged back to their local hospitals. No patients from this series were referred back from the district hospitals with new symptoms or complications of upper limb ischemia.
Traumatic Injuries
Fifty-four procedures were carried out in 53 patients who presented with acute arm ischemia secondary to a traumatic injury (Figure 1). The mean age of this group was 33.4 years, and there was a male preponderance of 5.6:1. Accidental injury was the cause of arterial injury in 23 patients. Thirteen patients sustained upper limb vascular trauma from road traffic accidents, and another six patients sustained serious occupational lacerations. Stabbing and gunshot wounds accounted for upper limb vascular trauma in 11 patients. The majority of injuries (n = 44) were distal to teres major. Five subclavian arteries and four axillary arteries were injured in this series. Injuries that were distal to pronator teres were usually treated by plastic surgeons and were excluded from the database. Sixty percent of patients with vascular trauma were treated by primary repair or patch angioplasty (n = 32), and 15 patients were treated by autologous reversed venous bypass grafting. Nine patients sustained a permanent neurologic deficit as a consequence of their injury. The risk of permanent nerve injury was higher with lacerations proximal to teres major. Sixty percent of subclavian artery injuries were associated with brachial plexus injuries compared with 11% of brachial artery injuries that had coexistent median or radial nerve damage.

Procedures carried out for upper limb trauma.
One above the elbow amputation was carried out for severe soft tissue burns associated with a ruptured false aneurysm of the brachial artery. The mortality in the traumatic injury group was 3.8%. These two patients were a 26-year-old male with severe multiple trauma who died from his injuries, having undergone a ligation of his subclavian artery in the emergency room, and a 72-year-old woman who died of a myocardial infarction in the early postoperative period following successful primary repair of a brachial artery. The median follow-up in this group was 6 months (0–48 months), but many of these patients failed to attend postoperative clinics. No patient had evidence of subsequent arterial occlusions.
Iatrogenic Injury
Two brachial thrombectomies were performed for thrombosis after insertion of an intra-arterial catheter. One of these patients died from preexisting respiratory failure exacerbated by postoperative bronchopneumonia.
Chronic Arm Ischemia from Atherosclerosis
Twenty-nine patients underwent 32 procedures for chronic ischemia caused by upper limb atherosclerosis (Figure 2). An additional six patients were identified who had undergone isolated cervical sympathectomy without further revascularization procedures. The mean age was 62.5 years, and this presentation was twice as common in women as in men. Ten patients were treated with a prosthetic bypass, which consisted of four carotid-subclavian, three axillary-axillary, a carotid-carotid, a carotid-brachial, and a subclavian-subclavian bypass. Two patients underwent autologous venous bypass. Another two patients were treated successfully by brachial endarterectomy, and the remainder were treated by angioplasty (n = 13) or stent placement (Wallstent, Boston Scientific, MA) (n = 5). Two patients required stenting following failed angioplasty, and one patient required a surgical bypass following failed stenting. One patient had a right cerebellar infarct following a left subclavian angioplasty, and another developed a brachial artery thrombosis and median nerve neuropraxia after subclavian stenting (Table 3). One patient who had a prosthetic bypass developed a neuropraxia in the distribution of the fifth and sixth cervical nerves, which fully recovered. Two patients died of cardiopulmonary causes. One patient died following subclavian artery thrombectomy and the other following subclavian artery stenting.
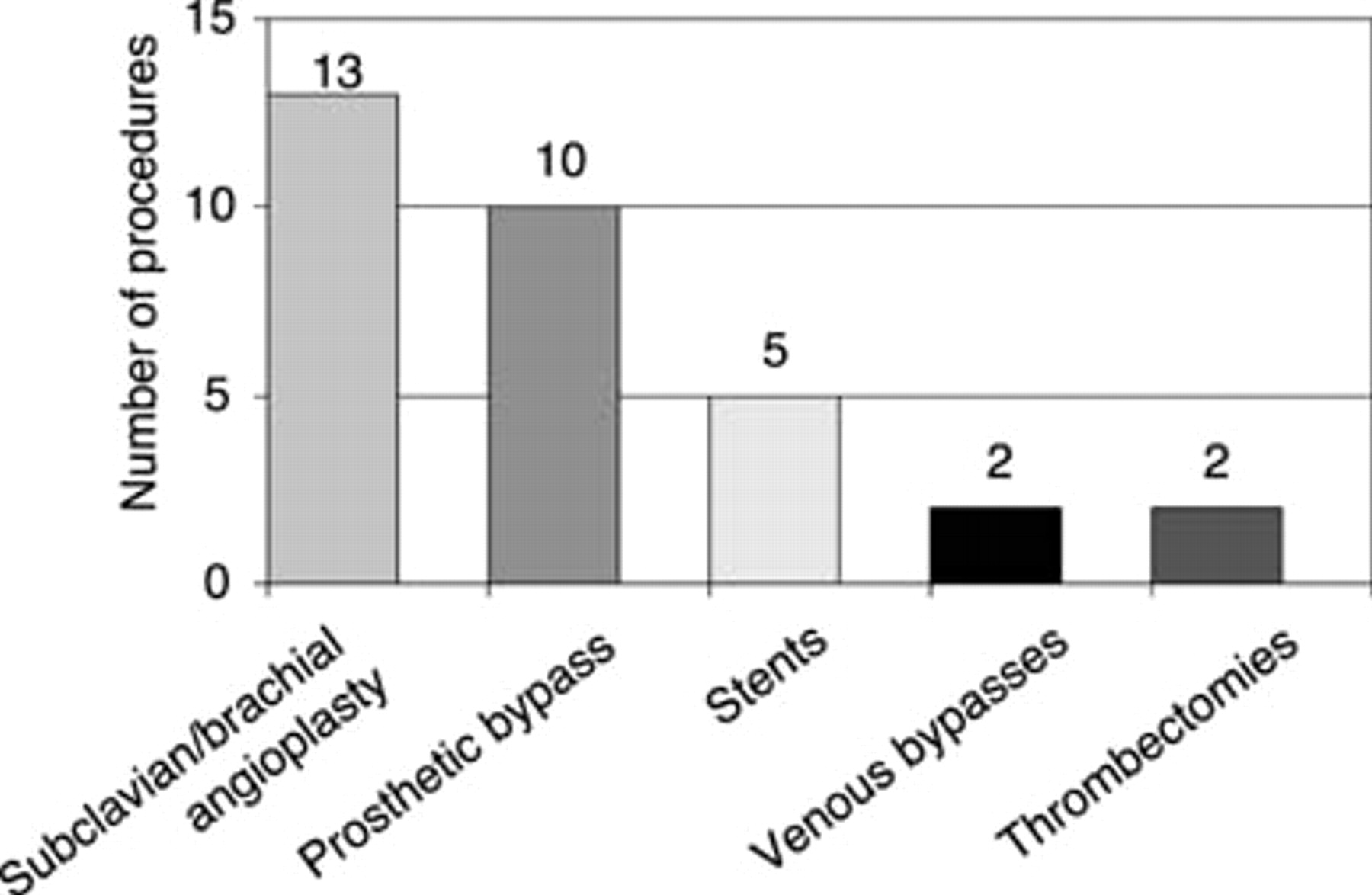
Procedures carried out for atherosclerosis causing chronic upper limb ischemia.
Endovascular Procedures for Chronic Upper Limb Ischemia (n = 26)
Patients with successful revascularization for chronic ischemia were followed up annually. Their median follow-up for bypass procedures was 5 years (range 0–19 years). All grafts were patent clinically or on duplex ultrasonography after 5 years. The median follow-up time for endovascular treatment was 3 years (range 0–7 years). The patency rate for technically successful angioplasties was 92% (12 of 13) at 3 years.
Subclavian and Coronary-Subclavian Steal Syndrome
Fifteen patients were treated for subclavian steal syndrome as diagnosed by arterial duplex ultrasonography and arteriography. This condition was also more common in women (F:M = 3:2), and most had a left-sided subclavian stenosis lesion (13 of 15). The mean age of these patients was 62.7 years. Five patients with subclavian steal syndrome had had a previous left internal mammary artery coronary bypass graft and presented with worsening angina on arm exertion with demonstrable retrograde flow through the previous left internal mammary artery graft. Three of these patients had previously been unsuccessfully treated by angioplasty and underwent carotid to subclavian bypass grafting. Nine patients had prosthetic carotid-subclavian bypass grafts, five had subclavian angioplasties, and one had a subclavian stent. One patient suffered a transient ischemic attack following angioplasty, but there were no major strokes and no patient died. Patients with upper limb revascularization for subclavian steal syndrome were followed up yearly for a median time of 3 years (range 0–9 years). Duplex ultrasonographic scanning of the bypass grafts showed 100% graft patency at 3 years.
Thoracic Outlet Syndrome
Eight patients (M:F = 1:1.7) underwent revascularization procedures for ischemia of the upper limb associated with thoracic outlet obstruction. Their mean age was 47 years. Four prosthetic and two venous bypasses were required to restore blood flow. Five of these were for subclavian artery aneurysms. Two patients who underwent successful thrombolysis had subsequent cervical rib excisions. There were no deaths in this group.
Iatrogenic Injury
Four patients required intervention for chronic arm ischemia caused by iatrogenic vascular injury. Two patients presented with radiation arteritis, causing a stenosis of the subclavian artery and a thrombosis of a subclavian artery. They were treated by angioplasty and thrombolysis, respectively. The other two patients developed radial artery false aneurysms secondary to intra-arterial line insertion. These were treated by ligation, and this did not cause ischemia of the forearm.
Discussion
The true incidence of upper limb ischemia is difficult to assess because patients treated conservatively are rarely identified and most figures are derived from published surgical series. 1 Series that combine acute and chronic ischemia are extremely rare. 5,13,29,30 Acute arm ischemia usually requires intervention and is often caused by thromboembolic disease, trauma, or iatrogenic injury. 31 Atherosclerosis, extrinsic compression, 11,32 and large vessel arteritis more commonly affect the subclavian and axillary arteries. Patients with these conditions may present with either acute thromboembolism or chronic arm ischemia.
Cardiac sources for emboli account for the great majority of thromboemboli, 1 and in our series, two-thirds of these patients had coexisting atrial fibrillation. The majority of patients (84%) with thromboembolism also had associated ischemic heart disease or a recent myocardial infarction. Emboli derived from the heart that lodge in the upper limb are most likely to occlude the brachial and axillary arteries. 33 Ninety-five percent of patients in the thromboembolic series presented with either a brachial or an axillary artery embolism.
Conservative and delayed management of thromboembolic disease of the upper limb has been shown to lead to amputation in 8% and residual functional impairment in between 50 and 75% of limbs. 9,10,22,34 Vascular intervention is therefore indicated in most patients to avoid these complications. 5,35 The Fogarty embolectomy balloon catheter (Edwards Life Sciences, Irvine, CA) introduced in 1963 36 remains the best method for removing brachial emboli. Thrombolysis combined with angioplasty is being increasingly used for brachial and distal emboli 37 but is associated with complications in up to a third of all patients treated, 38,39 with a risk of death, hemorrhage (5%), 35 and stroke (2%). 40 Delay in instigation of thrombolytic therapy or incomplete lysis of the arterial occlusion is associated with persistent tissue ischemia, a systemic inflammatory response resulting in cessation of microcirculatory flow causing skeletal muscle infarction and occasionally reperfusion injury. 41
Only one patient in the present series developed compartment syndrome after embolectomy. Compartment syndrome of the arm is rare 42 and is more commonly associated with musculoskeletal injury. 43 This is attributed to the thinner and weaker anterior antebrachial fascia of the lower forearm. Three fasciotomies were performed in our embolectomy series to prevent the possibility of compartment syndrome. These three patients presented with ischemic symptoms lasting more than 12 hours. Another series of upper limb vascular trauma suggested that a prophylactic fasciotomy should be performed when ischemia exceeds 6 to 8 hours. 43
Repeat embolization occurs more frequently when anticoagulants are omitted in the perioperative period (11 vs 33%). 44,45 This is associated with a higher mortality rate. 46 Six patients in the present series required reexploration for critical ischemia, but a second embolectomy was performed only in two cases (3.6%). This occurred despite anticoagulation being prescribed to all patients. One patient died after a reexploration in which no evidence of thrombus was found.
Although the mortality rate of 18.2% in the present series is high, 1 it is comparable to that of other published series of upper limb thromboembolectomies (Table 4). No limbs were lost in this series, and no deaths occurred as a consequence of gangrene or limb ischemia. This is probably because most of the patients had some form of revascularization, with no reported ischemic contractures up to 1-year follow-up.
Comparison of Guy's and St. Thomas' Upper Limb Embolectomy Outcome with Published Series
The 30-day and 1-year mortality following lower limb thromboembolectomies 47 is similar to the mortality reported in this upper limb series. This supports the concept that mortality following thromboembolectomy is a consequence of the patients' comorbidity rather than the embolus itself. 9 The higher mortality rate of patients having general anesthesia compared with those treated under locoregional anesthesia may reflect this increased cardiovascular risk. Although this difference was not statistically significant, it may well represent a type II error as a consequence of a small sample size.
The mechanism of injury and outcome of vascular trauma vary with the locality and cause. 48 A single-center series of 112 penetrating upper limb injuries over 3 years from South Africa reported that most were the result of stab wounds and gunshot injuries. 3 The mortality in this series was 3%, and only one limb was amputated. Road traffic accidents and penetrating stab injuries are the most common cause of vascular trauma in the United Kingdom, with large series being rare. 49 A single-center series from Belfast reported 22 upper limb arterial injuries over 10 years, but the relevant outcome for these patients was not provided. 50,51 Lower limb vascular injuries are twice as common as those of the upper limb, 3,52 with 20- to 30-year-old males being the usual victims. 53
The most common causes of injury in the present series were lacerations from either accidental, occupational, or road traffic injuries. Stab injuries and missile injuries are still rare causes of upper limb ischemia in central London, and no proximal upper limb injuries in this series required a median sternotomy. Most deaths in young patients with vascular trauma are the result of multiple organ injury, 53 and in our series, this cause was responsible for one death.
Chronic ischemia of the upper limb can be managed either with bypass grafts, angioplasty, or stent placement. A combined surgical and endovascular approach has been used successfully in some centers, which have reported a lower mortality than transthoracic procedures. 20 Transthoracic and extrathoracic 54 approaches to the subclavian artery and brachiocephalic trunk have both been used to manage proximal lesions. The transthoracic approach has a combined morbidity and mortality of up to 16%. 55,56 No transthoracic approaches were used in our patients with chronic arm ischemia, and only two patients died from revascularization for chronic ischemia. Surgical bypass grafts for brachial artery occlusions can be performed with low morbidity and mortality rates in specialist centers. 57
Endovascular treatment of upper limb arterial lesions has been used in this unit since 1995 and is confined to nontraumatic and chronic arterial lesions. The majority of these procedures were performed from 1999 onward (see Tables 2 and 3). Endovascular treatment for all cases of chronic ischemia was associated with more complications (8 of 28 procedures vs 2 of 31 procedures) than an open surgical approach in this series. This may be partly a consequence of the initial learning curve of percutaneous intervention. Although endovascular treatment is less invasive and avoids a general anesthetic, it still carries a risk of serious complications, such as cerebral emboli, restenosis, and failure to cross the occluding lesion. 56,58,59
Fewer than 10 patients a year required surgical treatment for upper limb ischemia in a large central London hospital complex. The most common causes were brachial emboli and trauma, and most traumatic injuries were from occupational or accidental causes. Although limb loss was rare, thromboembolectomy still had a considerable mortality, which was similar to the reported mortality rates following lower limb embolectomy. This postoperative mortality almost certainly reflects the patient's comorbidity rather than the ischemic consequences of embolization.
There are no published randomized trials to date comparing general with locoregional anesthesia for upper limb revascularization. Survival benefits have been postulated for locoregional anesthesia in patients undergoing lower limb revascularization 60 and carotid endarterectomy. 61
Thromboembolectomy should therefore probably be performed under local anesthesia whenever possible. The presence of coexistent ischemic heart disease, hypertension, diabetes, and chronic airway disease in patients with arm ischemia is the major cause of postoperative complications and deaths. By 1 year, another large cohort of these patients will have died from cardiac causes. More effort must be made toward diagnosing and treating the underlying cardiac comorbidity in this high-risk group of patients. 62