
Abstract
Coiling (or looping) of the artery is a rare morphologic entity, most frequently described in the internal carotid artery. In other arteries, coiling is rarely reported because it remains asymptomatic and without clinical relevance unless inadvertently injured, as for diagnostic or monitoring purposes. We present a case of an unusually difficult thrombectomy of the brachial artery after occlusion following withdrawal of the arterial cannula placed for monitoring during cardiac surgery owing to coiling of the distal part of the artery, which produced the “spring-squeeze phenomenon” during balloon catheter thrombectomy.
Coiling (or looping) of the artery is a rare morphologic entity, 1 most frequently described in the internal carotid artery 2 as a single cause of cerebrovascular insufficiency or combined with carotid atherosclerosis. 3
In other arteries, coiling is rarely reported because it remains asymptomatic and without clinical relevance unless inadvertently injured, 1 as for diagnostic or monitoring purposes.
We present a case of an unusually difficult thrombectomy of the brachial artery after occlusion following withdrawal of the arterial cannula placed for monitoring during cardiac surgery owing to coiling of the distal part of the artery, which produced the “spring-squeeze phenomenon” during balloon catheter thrombectomy. In the available English literature, we could not find a similar case that complicated an otherwise routinely performed procedure.
Case Report
A 71-year-old female was admitted to our cardiac surgery clinic for a coronary artery bypass graft (CABG) procedure. Three months earlier, she had an acute inferoposterior myocardial infarction. She complained of chest pain 2 years before the myocardial infarction, with dyspnea and vertigo.
During previous hospitalization, echocardiography showed an ejection fraction of 45%, with mitral and tricuspid regurgitation of 2+. Duplex scanning of the supra-aortic branches showed kinking of the left internal carotid artery, with elongation of the right internal carotid artery and tortuosity of both vertebral arteries. Coronarography showed significant stenosis of the left descending artery and circumflex artery, with occlusion of the right coronary artery. She was indicated for CABG and classified as New York Heart Association III with Euroscore 7. Beating-heart CABG was performed with one left descending artery–left internal mammary artery graft and one venous right coronary artery graft. The surgical procedure and early postoperative course were uneventful, with a 1-day intensive care unit stay.
On the fifth postoperative day, she complained of pain in the right hand and arm, with paresthesia and arm weakness. On physical examination, her right hand was pale and tender, with hand and arm weakness and absent wrist and brachial pulse. A spot mark was seen in the right cubital fold that originated from the arterial cannula placed prior to CABG for blood pressure monitoring and removed 2 days earlier.
Because duplex ultrasonography was unavailable at the moment, urgent arteriography was performed. Thrombotic occlusion of the distal third of the brachial artery and cubital artery down to the bifurcation (Figure 1) was seen, and urgent thrombectomy was indicated.
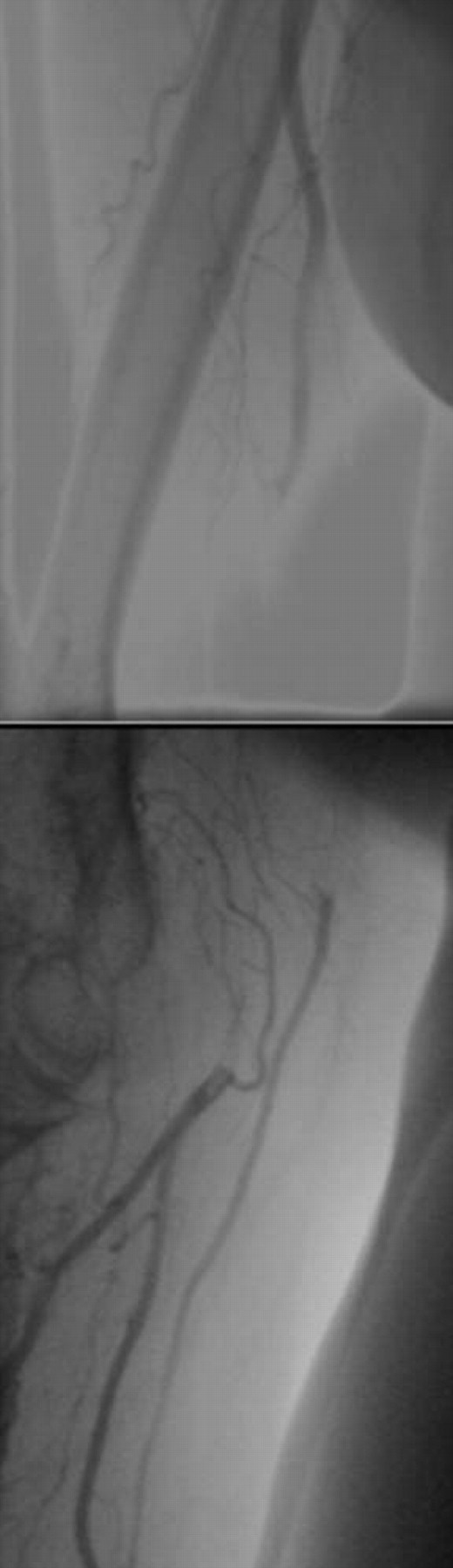
Arteriography of the right arm: thrombotic occlusion of the distal brachial and cubital artery, with patent distal arteries but without verification of any morphologic disturbance.
Surgery was performed under axillary block anesthesia with the patient in the supine position with the arm extended at the auxiliary table. An oblique skin incision was placed in the cubital fold, and the distal cubital artery and proximal radial and ulnar arteries were dissected. After administration of 5,000 IU of heparin, transverse arteriotomy was made in the cubital artery, just above the bifurcation. Total occlusion was found, with fresh thrombus that was easily removed from the incision zone and with prompt backflow bleeding from the distal arteries. No thrombus was found in the radial and ulnar artery after balloon catheter thrombectomy. After clamping the artery distally to the arteriotomy, the balloon catheter was easily introduced into the brachial artery. During thrombectomy, some unusual resistance was felt during withdrawal of the catheter, but fresh thrombus was delivered, and a moderate pulsating flow was established. The arteriotomy was closed with continuous 6-0 polypropylene suture. Prior to closing, the wound artery was palpated, but the pulse was weak. Not having a flowmeter, we tried to palpate the pulse upward the brachial artery and found a strong, regular pulse.
Further exploration of the brachial artery was done by extending the skin incision along the medial fold of the bicipital muscle and dissecting the distal portion of the artery. An uncommon coiling of the artery was found (Figure 2). After clamping the artery proximal to the coiled part, we resected the artery 2 cm in length and found additional thrombus within the lumen (Figure 3). Oblique end-to-end anastomosis was performed to reconstruct the artery (Figure 4), with prompt pulsating filling of the distal artery. Duplex ultrasonography was performed 2 days later and showed good patency and adequate flow through the anastomosed part of the artery. We concluded that thrombectomy through the coiled part of the artery produced the spring-squeeze phenomenon, which precluded the success of the initial procedure.

Dissected coiled brachial artery.

Resected specimen of the artery with the thrombus removed: the thrombus on the left was removed at the initial balloon catheter thrombectomy; the part on the right was found within the resected part of the artery and in the proximal brachial artery.

Brachial artery after reconstruction.
The postoperative course was uneventful as far as the reconstructed artery was concerned but was complicated by the instability of the sternum, which required surgical treatment, and iliac femoral deep venous thrombosis, which postponed rehabilitation. The patient received low-molecular-weight heparin and oral anticoagulants, with satisfactory vein recanalization during the following year. Further investigations for coagulation disorders showed no antithrombin III, protein S, or protein C deficiency. Antiphospholipid antibodies were negative, and homocysteine levels were normal.
Three years after brachial artery reconstruction, the patient had no complaints about her right arm and hand function, except for occasional paresthesia.
Discussion
The brachial artery is not used for long-term catheterization and routine hemodynamic monitoring because a high incidence of ischemic complications is anticipated. However, direct brachial artery puncture is used increasingly for day-case arteriography and in patients with severe aortoiliac disease. In expert hands, low complication rates are reported, but the risks of brachial artery puncture may be higher when it is performed by someone less experienced. 4
In the series of Moran and colleagues, brachial artery thrombosis occurred in 4 (1.7%) of 157 patients who had long-term catheters placed for infusion of chemotherapeutic agents. 5 The authors suggested that long-term brachial artery catheterization was associated with a low incidence of permanent ischemic complications. Likewise, Kline and colleagues reported 1.5% brachial artery thrombosis in 532 of 34,291 transbrachial cardiac catheterizations performed at the Cleveland Clinic from 1980 to 1988, 6 and McCollum and Mavor reported 0.9% brachial artery thrombosis during a 3-year period after 12,158 cardiac catheterizations were performed. 7
Because of the unpredictability of ischemic symptoms occurring after brachial artery thrombosis, the need for bypass graft surgery when thrombectomy is delayed, and the good results with early surgical intervention, early exploration of brachial artery complications after cardiac catheterization and appropriate repair are recommended. 7
According to the experience of Kline and colleagues, a surgical delay of more than 1 day after postcatheterization thrombosis of the brachial artery was associated with a higher incidence of recurrent thrombosis (12% vs 2%; p = .025). 6 The liberal use of segmental arterial resection and overnight heparin anticoagulation seemed, especially, to reduce the risk of early failure in all patients, but improvement was particularly marked in women (25% vs 6%; p = .0004). Prolonged time of cardiac catheterization (over 4 hours), a delay in diagnosis of more than 24 hours, and omitting the use of systemic heparinization at the time of diagnosis are three factors that appear to increase the likelihood of late failures. 8
Except for supra-aortic branches, morphologic arterial variations represent a benign and incidental finding. Del Corso and colleagues reported that atherosclerosis, hypertension, and aging may play an important role in producing carotid abnormalities, with aging seeming to be more important than atherosclerosis. 9 Similarly, coiling was more frequently associated with arterial hypertension alone in males and with arterial hypertension associated with other risk factors in females, showing a statistically significant difference in the series of Prencipe and colleagues. 10
All of these factors were present in our patient; moreover, kinking and elongation of both internal carotid arteries were found, with tortuosity of both vertebral arteries.
Surgical correction of coiling and particularly brachial artery thrombectomy should be routine in experienced team hands. As we did in our patient, in all instances of isolated kinking and coiling in the series of Poulias and colleagues, straightening was obtained by segmental resection of the common carotid artery and end-to-end anastomosis. 11
Arteriography was inconclusive in our patient. It did not elucidate the morphology of the thrombosed artery and might lead an inexperienced surgeon to overlook unsatisfactory thrombectomy, in the absence of a flowmeter. Noninvasive color Doppler ultrasonography, which is easily repeatable, can provide useful data for the morphologic evaluation of dolichoarterial disease, 12 but it was not available until 2 days after the procedure owing to technical reasons.